
Abstract
Background:
Cognitive decline among people living with HIV (PLWH) is growing concern as world populations become increasing older including higher proportions of PLWH. It is vitally important to understand psychosocial predictors of age-related cognitive decline men who have sex with men (MSM) living with HIV.
Objectives:
The current study seeks to examine psychosocial risk factors the contribute to the risk of age-related cognitive impairment as measured by Cardiovascular Risk Factors, Aging, and Incidence of Dementia (CAIDE) score in a racially diverse sample of MSM living with HIV.
Design:
The present analysis utilizes data from the baseline (n = 196) and 6-month follow-up (n = 135) time points of a longitudinal cohort study of PLWH.
Methods:
Using a self-report survey, we examine the associations between psychosocial predictors (e.g. trauma, mental health, chronic pain, sleep disturbance, etc.) and risk of dementia using the CAIDE risk score. Analyses include linear and logistic regression.
Results:
In adjusted model stress, chronic pain, Black racial identity, and having a sexual identity that is bisexual or another category are all positively associated with CAIDE scores. Childhood sexual abuse history was negatively associated with CAIDE scores indicating a protective effect. Sleep disorder has a positive association with CAIDE scores after adjusting for the baseline CAIDE scores.
Conclusion:
These results indicate modifiable correlates of cognitive risk (stress and chronic pain). Interventions should seek to address these comorbid factors including the consideration of minority stress and stigma. Interventions should seek to reach Black and bisexual men living with HIV, including possible cultural tailoring to interventions and messaging. Lastly, future research should examine the impact of variation within childhood sexual abuse histories to better understand their association with cognitive impairment later in life. This may include considering the nature, severity, and potential treatment of trauma symptoms.
Plain language summary
Why was the study done? Older people are becoming a larger portion of our communities including older people living with HIV. It’s important to understand what makes older people more likely to have memory problems as they age including older people living with HIV. What did the researchers do? We asked 196 middle-aged and older adults who have HIV to answer questions about their health including things that we know might make them more likely to have memory problems later in life. What did the researchers find? We found that having more stress or reoccurring pain was related to being more likely to have memory problems later in life. People who have trouble sleeping were more likely to have memory problems later in life. We also found that Black people were more likely to have memory problems later in life. People who had been abused sexually as children were less likely to have memory problems later in life. What do the findings mean? These findings help us understand things that may make someone more likely to have memory problems later in life. These include things that could be changed like reoccurring pain and troubles sleeping. It also highlighted that Black people may need more support to prevent memory problems later in life.
Background
It is estimated that by 2050, 21.1% of the worldwide population will consist of individuals 60 and over. 1 The United States is no exception to the rise of the aging population. For the first time in recorded history, older adults are estimated to outnumber children under 18 within the next decade.1–3 Within this context, aging-related cognitive impairment is a prominent health concern. 1 People living with dementia in the United States are set to increase from 7 million in 2020 to 9 million by 2030. 4
Aging-related cognitive impairment
Dementia, which also includes Alzheimer’s disease, affects individuals and their cognitive functioning 5 including one’s ability to clearly think, learn, and remember 6 as well as mood, personality, and affect eventually necessitating care-giving. 5
Age is the strongest risk factor associated with cognitive decline (World Health Organization, 2019), 7 while other identified risk factors include low education level, an inactive lifestyle, hypertension, diabetes, midlife obesity, smoking, and depression. 8 In particular, studies revealed that cardiovascular risk factors also predict cognitive dysfunction and dementia as people age. 9 The Cardiovascular Risk Factors, Aging, and Incidence of Dementia (CAIDE) risk score is widely used to help predict dementia risk.10,11 CAIDE risk scores are based on easily available midlife risk factors and underscore the necessity to consider and identify other modifiable risk factors that might impact aging individuals and their cognitive decline. 12 Other risk factors in the calculation of CAIDE include age, hypertension, hypercholesterolemia, physical inactivity, obesity, and educational level. 11
Cognitive impairment in people living with HIV
Parallel to the increase in the aging population, the number of individuals living with human immunodeficiency virus (HIV) is also growing. 13 Currently, more than 35 million people worldwide live with HIV, with 1.2 million living in the United States. 14 Effective antiretroviral therapy (ART) has improved the life expectancy of people living with HIV.13,15 In 2018, 51% of those living with HIV were older than 50 years. 16 By 2030, it is estimated that 70% of people living with HIV (PLWH) in the United States will be over the age of 50, which is a 20% increase from 2015. 13 Additionally, 10% of people newly diagnosed with HIV are over the age of 55. 17
Despite the effectiveness of ART, HIV targets the central nervous system after infection and can lead to neurological, behavioral, and cognitive complications. 18 Research is not in agreement whether HIV accelerates aging in general. 13 A study aiming to assess cognitive decline among PLHIV had unique contributions to this field of research recruited a sample of 457 PLHIV (Median age = 52) and observed cognitive decline longitudinally, collecting data at baseline, 12 months, and 24 months. 19 Most participants remained cognitively stable across time points, with a small portion experiencing statistically meaningful decline (6% at Month-12 and 7% at Month-24). 19 The authors attributed this to viral suppression, but further added that 31 and 21 percent of participants showed subtle cognitive decline at months 12 and 24 respectively indicating that PLHIV experience ongoing albeit subtle cognitive changes resulting in impaired cognition regardless of viral suppression. Another study conducted in 2017 measuring 96 HIV-positive and 44 comparable HIV-negative participants whose cognition was tested at baseline and 18 months found that a higher portion of HIV-positive participants showed a relevant decline over 18 months compared with HIV-negative participants. 20
Notably, individuals with HIV may be impacted by HAND; HIV-associated neurocognitive disorders. 21 HAND is defined as an impairment in cognitive functioning, including asymptomatic neurocognitive impairment, mild neurocognitive disorder, and HIV-associated dementia (HAD). 22 HAND is said to affect one in two persons living with HIV. 23 Research suggests that with the introduction of ART, severe dementia is not as widespread, although cognitive impairments are common. 21 A recent meta-analysis of 123 studies showed a 42.6% global prevalence of HAND, although indicating a milder form of cognitive impairment representing HAD as uncommon. 21 Similarly, Heaton et al.24,25 claimed that mild neurocognitive deficits were found in 45% of PLWH in the areas of functioning, learning, and memory, while others argue that neurocognitive impairment can impact as many as 40% of PLWH.
The rates of vascular risk factors and disease increase with age and are also elevated in those with HIV, 9 which contribute to cognitive decline based on a current systematic review and meta-analysis of the literature. 26 Race, gender, psychosocial risk factors, and antiretroviral adherence can impact this. There can be various other factors present that impact aging PLWH and their cognitive functioning, such as childhood trauma, pain, sleep quality, isolation, and racial disparities.
Childhood trauma and cognitive decline
Adverse childhood experiences (ACEs) are traumatic experiences that include household dysfunction or physical or sexual abuse before 18 years of age. 27 Within the United States, 45% of youth have experienced one or more traumatic experiences, while 10% have experienced three or more traumatic experiences. 28 Research suggests that such experiences can impact an individual throughout life, including increased health risk behaviors, health status, and diseases. In addition to the research above, ACEs are recognized as predictors of HIV risk 29 and can contribute to risks that can increase transmission, including drinking and drug use, intimate partner violence, and sexual risk behaviors. 30
The research appears inconclusive when determining whether traumatic childhood experiences have a relationship to cognitive decline, with reported inconsistencies in measuring childhood exposure and the various pathways to cognitive decline. 31 For example, in one study, ACEs are significantly associated with subjective cognitive decline, and the strength of this association increases with the number of traumatic childhood experiences. 32 Yet others have suggested a lack of clarity regarding whether early life stress was related to cognitive functioning pointing out the importance of the difference in effect by trauma type. 33 The association between adverse experience and cognitive impairment among PLWH is less known, though one study revealed that the exposure to trauma, economic hardship, and stress are related to cognitive decline among aging PLWH. 14
Racial disparities and cognitive decline
In 2019, according to the Centers for Disease Control and Prevention, Black/African Americans were the largest group living with HIV at 40%, equating to eight times the rate of HIV infection compared to non-Latino Whites and Hispanic/Latino three times the rate of infection compared to non-Latino Whites. 34
Cross-sectional studies have shown cognitive impairment in PLWH to be more prominent in some Latino 35 and Black 36 individuals as compared to whites. A recent study found Latino PLWH at higher risk of early cognitive decline compared with White and Black PLWH and concluded that medical comorbidities explained only some of the decline, but most were unexplained. 37 Structural, institutional, sociocultural, and biomedical factors may contribute 37 as well as the impact of structural racism that influences health and health inequities. 38
Other aspects associated with HIV
Studies find that pain has been reported as one of the most common symptoms found in PLWH at all stages of the disease. 39 Pain is associated with many negative outcomes among PLWH including sleep quality,39,40 ability to work, mood, 39 mental health, drug abuse, health care access, and ART adherence, but less is known about the association between pain and cognitive impairment among PLWH. 41 In a recent study, social isolation was significantly associated with poor cognitive function, reporting that those with HAND were more likely to experience social isolation. 42
Current study
The current study seeks to examine psychosocial risk factors for cognitive impairment risk as measured by CAIDE score in a racially diverse sample of men who have sex with men (MSM) living with HIV. We hypothesize that negative biopsychosocial predictors (pain, sleep problems, negative mental health indicators, internalized stigma, discrimination, and trauma) will be associated with higher cognitive impairment risk and that positive biopsychosocial predictors (resilience, social support) will be associated with lower cognitive impairment risk.
Method
Study design
In the present study, we used data from a recently concluded longitudinal cohort study on HIV and hypertension among MSM in Hawaii and Philadelphia. Participants were recruited from eight sites, including academic medical centers (e.g. Clint Spencer Clinic), governmental organizations (e.g. Hawaii Department of Health), and nongovernmental organizations (e.g. Life Foundation) beginning in May 2019 and ending in May 2023. The sample constituted a community-based convenience sample. Trained interviewers screened MSM at the study sites before consenting eligible participants. During enrollment, participants completed a Computer-Assisted Self0Interview (CASI) psychological and behavioral assessment. Given that most of the data collection occurred during the COVID-19 pandemic, CASI allowed for ease of data collection while social-distancing. CASI is a common data collection technique in HIV and sexual health research, which may have some benefits such as reductions in social-desirability bias with sensitive topics such as sexual risk behaviors,43,44 and studies have suggested limited differences between self-administered and interview-administered survey responses. 45 In 2020 80% and 2023 90% of U.S. citizens had smartphones (currently 97% among people ages 30–49 and 89% among ages 50–64, 76% among ages 65 and older). 46 Across incomes, smartphone coverage is 90% or higher except for those who earn less than $30,000 annually who have 79% coverage. 46 Every 6 months for the next 3 years (36 months), participants were contacted to complete the same CASI assessments with the actual time to completion averaging approximately 8.5 months. This study was approved by the University of Hawaii Institutional Review Board (2018-00508).
Participants
The selection criteria for participating were: (1) the participant was aged 18 or above; (2) the participant self-identified as a a cisgender man assigned male at birth (termed ‘biological male’ in the survey); (3) the participant self-reported having had sex with men (oral, anal, or both); and (4) the participant had a verifiable HIV-positive status. Participants were excluded from the present analysis if: (1) younger than age 39 and (2) having completed 35% or less of the survey. No additional exclusions were applied. This additional age restriction was meant to duplicate the ages targeted by the CAIDE score in previous work.11,47 This resulted in n = 196 at the baseline and 173 at the 6-month follow-up time points.
Measures
Demographics
Participants were asked to report their age, race/ethnicity, sexual identity, education, and annual household income. To make the analyses simpler, those demographics were dichotomized (age, sexual identity, education, and income) or categorized into four groups (race/ethnicity). Specifically, age was dichotomized by a cutoff of 64 to make it consistent with the maximum age reported in the CAIDE risk score calculation. Race/ethnicity contained four categories: white, black, Native Hawaiian and Pacific Islander (NHPI) & Asian, and other race/ethnicity, whereas the ‘other’ category included Indigenous, Latinx, and multiracial. Sexual identity had categories of gay and other, where the ‘other’ category combined bisexual, heterosexual, and other sexual orientation. Education was dichotomized by whether an at least Bachelor’s degree was completed. Annual house income was dichotomized by a cutoff of $20,000, the approximate poverty line for a family of two in Hawaii.
Pain
Pain was measured by a single question asking the number of days that pain made it hard for usual activities such as self-care, work, or reaction during the past 30 days using the Centers of Disease Control Health-Related Quality of Life Measure. 48
Sleep
Sleep was measured by a single question asking the number of days that one felt not getting enough rest or sleep during the past 30 days using the Centers of Disease Control Health-Related Quality of Life Measure. 48
Mental health
Mental health variables contained depression, generalized anxiety, and perceived stress. Depression was measured by the 10-item Center for Epidemiologic Studies Short Depression Scale (CES-D-R-10). 49 Participants were expected to respond to how often they experienced depressive symptoms during the past week on a four-point scale ranging from ‘less than 1 day’ to ‘5–7 days’. Questions 5 and 8 that were positive had values 3, 2, 1, and 0 assigned to frequencies from the lowest to highest, that is, assigned 3 to ‘less than 1 day’ and 0 to ‘5–7 days’. For the rest of the questions, the magnitude of the scores assigned was in concordance with the frequencies. The total score was calculated by adding the scores of each question, resulting in a range of scores from 0 to 30. Higher scores indicate higher levels of depressive symptoms. A total score that was equal to or above 10 was considered depressed (Cronbach’s α = 0.884). 50
The seven-item Generalized Anxiety Disorder Scale (GAD-7) was used to assess the anxiety symptoms over the past 2weeks. 50 Each item was rated on a four-point Likert-type scale with 0 representing ‘not at all’ to 3 representing ‘nearly every day’. The responses of each item were summed to create a total score ranging from 0 to 21, with a higher score suggesting a higher level of generalized anxiety disorder. A cutoff of 8 (≥ 8) was recommended to binarize anxiety (Cronbach’s α = 0.921). 51
The 10-item Cohen’s Perceived Stress Scale (PSS) was adopted to measure the levels of stress that participants felt during the last month. 52 A five-point Likert-type scale was used to assess the frequencies of having stressful feelings and thoughts ranging from ‘never’ (0) to ‘very often’ (4). The responses were summed to create a total score ranging from 0 to 40, with a higher score suggesting a higher stress level. The perceived stress was further categorized into three groups: 0–13 referred to low perceived stress; 14–26 referred to moderate perceived stress; and 27–40 referred to high perceived stress (Cronbach’s α = 0.919). 53
Internalized homophobia
Internalized homophobia was assessed by an eight-item scale adapted by.
54
This scale included seven items adapted from two other scales55,56 and created the last item themselves. A four-point Likert-type scale was applied, instead of the original seven-point and five-point scales, to measure the participants’ homophobic beliefs or thoughts due to their sexual identity as MSM. The responses were averaged to create a score ranging from 1 to 4, with a higher score indicating more serious internalized homophobia (Cronbach’s
Discrimination
The experiences of discrimination were measured by a nine-item questionnaire that covered specified situations. 57 Participants were supposed to respond ‘yes’ or ‘no’ to whether they have experienced discrimination in nine certain situations, followed by answering the frequency of occurrence of such experiences if selected ‘yes’. The frequencies measured the total occurrences by assigning values of 0 to ‘never’; 1 to ‘once’; 2.5 to ‘2–3 times’, and 5 to ‘4 or more times’ and summing the values up. The total occurrences ranged from 0 to 45, indicating greater experiences of discrimination (Cronbach’s α = 0.846).
Early trauma
Early trauma experiences were measured using the Early Trauma Inventory–Self Report Short Form (ETISR-SF). 58 The 27-item questionnaire is a short form of the self-report version of clinician-administered ETI (occurred before the age of 18) that includes four domains: general trauma (11 items), physical abuse (5 items), emotional abuse (5 items), and sexual abuse (6 items). In our study, ‘Serious injury of a friend’ within the general trauma domain was excluded, resulting in a total of 26 items. Participants responded by answering whether they have experienced these items (1 = ‘yes’) or not (0 = ‘no’). A total score was summed for each domain, as well as for the entire questionnaire. The scores ranged from 0 to 10, 5, 5, and 6 within the four domains accordingly, and ranged from 0 to 26 in total. Higher scores indicate more severe early trauma. The Cronbach’s α for general trauma, physical, emotional, and sexual abuse were 0.691, 0.815, 0.855, and 0.881, respectively.
Resilience
The four-item Brief Resilient Coping Scale (BRCS) was used to measure participants’ resilience in terms of capturing tendencies to cope with stress in a highly adaptive manner. 59 The scale presented four descriptions of positively reacting to difficulties, asking the likelihood of a participant for each description on a five-point Likert-type scale ranging from ‘Does not describe me at all’ (1) to ‘Describes me well’ (5). The total score that ranged from 4 to 20 was calculated by summing the responses of each item, with higher scores indicating greater resilience. It was further categorized into three groups: 4–13 referred to low resilient copers; 14–16 referred to moderate resilient copers; 17–20 referred to high resilient copers (Cronbach’s α = 0.762). 60
Social support
The 12-item Multidimensional Scale of Perceived Social Support (MSPSS) was used to assess three sources of support of participants, including their family, friends, and significant others. 61 The perceived social support was measured on a seven-point Likert-type scale with 1 representing very strongly disagree to 7 representing very strongly agree. The responses were averaged to create the total score ranging from 1 to 7, with higher scores indicating greater perceived social support. Cutoffs of 3 and 5 were used to categorize the perceived social support into low, moderate, and high groups (Cronbach’s α = 0.916).
CAIDE risk score
CAIDE risk score, developed in the cardiovascular risk factors, aging and dementia study, predicts the risk of late-life dementia for people of middle age based on their midlife risk factors, including age, education, sex, systolic blood pressure, body mass index (BMI), total cholesterol, and physical activity. 10 The dementia risk score ranges from 0 to 15, with higher scores indicating a greater risk of dementia. A cutoff of 6 was suggested to binarize the risk to low- (< 6) and high-risk (≥6) groups. 62 In our study, we combined self-reported high blood pressure history and hypertension history to represent high systolic blood pressure, and used self-reported high cholesterol history to represent high total cholesterol level. BMI was calculated from participants’ heights and weights. Participants who performed moderate or intense physical activities at least twice a week and at least 20–30 min each time were marked as active. CAIDE risk score was then calculated for each participant at the baseline.
Data analysis
Analyses were conducted using R. Multiple imputation was applied to handle missing data for factors that were utilized to predict CAIDE risk score using the R package ‘MICE’.
63
Imputation was performed based on all participants (
Descriptive statistics were used to assess the distribution of the variables. Differences between participants with regard to demographics were described using the Analysis of Variance test (ANOVA). Linear regression was further used to investigate the association between demographics and the variables aforementioned. To examine the association between CAIDE risk and the other variables, linear regression of CAIDE risk score and logistic regression of CAIDE high/low dementia risk adjusted for demographics were applied for each independent variable separately based on variable type (continuous or dichotomous). Linear regressions show incremental change in CAIDE score, whereas logistic models show associations with the highest risk category. The exclusive use of cutoff values may limit the ability to detect more subtle associations. 64 The baseline CAIDE risk variables (continuous or binary with respect to the response variable) were further controlled for analyses at the 6-month follow-up. Among the demographic variables, the 39–64 years category was the reference group for age; white was the reference group for race/ethnicity; gay was the reference group for sexual identity; without at least a Bachelor’s degree was the reference group for education; and less than $20,000 was the reference group for annual household income. In addition, categorized depression, anxiety, perceived stress, total early trauma, resiliency, and social support were considered as the independent variables in separate analyses. Significant independent variables were selected to include in the final models.
Results
Sample characteristics
The characteristics of the demographics at the baseline are summarized in Table 1. The average age was 57.5 years (SD = 8.8), with 77.6% of them at their midlife. 35.2% of these participants were white; 32.7% were black; 21.9% were NHPI or Asian; and 10.2% were Indigenous, Latinx, or multiracial. Among these 196 MSM, 79.1% were gay; the rest were bisexual, heterosexual, or with other sex orientations. 60.7% of them did not complete at least a Bachelor’s degree; 42.3% had annual house incomes less than $20,000. The average CAIDE risk score of the 196 MSM was 7.2 (SD = 2.6), indicating a slightly high risk using a cutoff of 6.
Demographics at the baseline (

CAIDE, CAIDE risk score; NHPI, Native Hawaiian and Pacific Islander.
The characteristics of the other measures at the baseline are presented in Supplemental Table S1. A total of 187 MSM reported the number of days that pain made it hard for their daily activities during the past 30 days; the average number of days was 7 (SD = 9.6). A total of 189 MSM reported the number of days they did not get enough sleep or rest during the past 30 days; the average number of days was 9.7 (SD = 9.6). Among the mental health outcomes, 190, 191, and 187 participants completed their self-reported depression, anxiety, and perceived stress measures. Overall, the average score of depression was 9.2 (SD = 9.1, range: 0–30). The average score was 12.5 (SD = 5.1, range: 0–21) for anxiety and 14.4 (SD = 8.5, range: 0–40) for perceived stress. These numbers indicate that this sample of MSM had a low level of depression, a high level of anxiety, and a moderate level of perceived stress. The average of the mean internalized homophobia scores of 190 MSM was 2.5 (SD = 0.3, range: 1–4). Noticeably, the eight-item scale that measured internalized homophobia for this sample was found to lack internal consistency, as evidenced by a Cronbach’s alpha of 0.271. The average frequency of 185 MSM from the sample experiencing discrimination situations was 8.0 (SD = 9.5, range: 0–45). A total of 193 participants reported their early trauma experience. The average scores of the four domains, including general trauma, physical abuse, emotional abuse, and sexual abuse, were 2.8 (SD = 1.8, range: 0–10), 2.2 (SD = 1.8, range: 0–5), 2.2 (SD = 1.9, range: 0–5), and 1.8 (SD = 1.8, range = 0–6), respectively. At the 6-month follow-up, the average CAIDE risk score of the 135 MSM increased by 0.2 (mean = 7.4, SD = 2.5) (see Supplemental Table S3).
Association between variables and demographics
ANOVA test was used to assess the difference in each variable with respect to demographics. Linear regression models were further applied to measure the effects of demographics on those variables. Associations between variables and demographics at the baseline are presented in Supplemental Table S1a and S1b, and regression coefficients with demographics are presented in Supplemental Table S2a and S2b. Associations and regression coefficients at the 6-month follow-up time point are presented in Supplemental Tables S3a, S3b and S4a, S4b, respectively.
Significant differences between age groups were found in CAIDE risk, pain, and sleep at the baseline. Age was positively associated with the risk of dementia. A higher age would lead to less pain and better sleep. Furthermore, people with higher ages tended to have fewer depressive symptoms and less discrimination experience using the loosened significant level. At the 6-month follow-up, age was found not associated with pain. In addition, higher age was significantly associated with less anxiety, perceived stress, and general childhood trauma experience.
Significant differences among race/ethnicity groups were assessed in CAIDE risk, discrimination, and childhood physical abuse at the baseline. Using white as the reference group, Black identity was associated with an increased risk of developing dementia, while being NHPI & Asian were associated with a decreased risk. Black MSM were noticeably more likely to experience discrimination (β = 7.178) and tended to experience more physical abuse in their childhood (β = 0.767). Additionally, they were more likely to have internalized homophobia (β = 0.126) and were exposed to more sexual abuse in childhood (β = 0.890). NHPI and Asian identity were significantly associated with less pain (β = –3.893), and relatively worse resilience. At the 6-month follow-up, race did not seem to pose an effect on CAIDE risk. Black racial identity was associated with more perceived stress according to the loosened significance level.
Significant differences between sexual identities were found in internalized homophobia, childhood physical abuse, and childhood sexual abuse at the baseline. Compared to being homosexual, other sexual orientations including bisexual, heterosexual, and other orientations were associated with more internalized homophobia and childhood physical and sexual abuse. The findings were consistent at the 6-month follow-up time point.
At the baseline, education was found to have a significant positive effect on resilience and social support and a less significant negative effect on anxiety score, meaning that the higher the education level, the better the resilience and social support, and the less the anxiety. Income showed a significant positive effect on social support and negative effect on pain, indicating that an increase in income could lead to an increase in social support and a decrease in sleep issues.
Regressions
Each variable was fitted separately to linear regression models (using continuous CAIDE risk score as the dependent variable) and logistic regression models (using binary CAIDE risk score by a cutoff of 6) adjusted for all demographics. According to the linear regression model with continuous CAIDE risk score, pain (β = 0.052, p = 0.006) and the categorical perceived stress (moderate: β = 0.783, p = 0.033; high: β = –1.112, p = 0.093) were significant. According to the logistic regression taking the binary CAIDE risk variable, pain (β = 0.034, p = 0.096) and childhood sexual abuse (β = −0.184, p = 0.034) were significant. The full list of these regression results is summarized in Table 2. The baseline CAIDE risk variables were further controlled in these bivariate analyses at the 6-month follow-up. After accounting for the baseline CAIDE status, only sleep positively affected the high risk of dementia (β = 0.086, p = 0.035). The other regression coefficients were presented in Table 3.
Linear regression and logistic regression results for each predictor adjusted for demographics at the baseline.

BRCS, Resilience; CAIDE_IND, CAIDE risk indicator by the cutoff of 6; CAIDE_SUM, CAIDE risk score; CESDR, Depression; EOD, experiences of discrimination; ETI_EA, Early emotional abuse; ETI_GT, Early general trauma; ETI_PA, Early physical abuse; ETI_SA, Early sexual abuse; GAD, General anxiety disorder; IHS, Internalized homophobia; MSPSS, Perceived social support; PAIN, number of days that pain makes it hard for daily activities; PSS, Perceived stress; SLEEP, number of days not having enough rest or sleep.
Linear regression and logistic regression results for each predictor adjusted for demographics and baseline CAIDE risk at the 6-month follow-up time point.

BRCS, Resilience; CAIDE_IND, CAIDE risk indicator by the cutoff of 6; CAIDE_SUM, CAIDE risk score; CESDR, Depression; EOD, Experiences of discrimination; ETI_EA – Early emotional abuse; ETI_GT, Early general trauma; ETI_PA, Early physical abuse; ETI_SA, Early sexual abuse; GAD, General anxiety disorder; IHS, Internalized homophobia; MSPSS, Perceived social support; PAIN, number of days that pain makes it hard for daily activities; PSS, Perceived stress; SLEEP, number of days not having enough rest or sleep.
Significant variables were taken into the final linear/logistic regression models together with the demographics. At the baseline, holding all the other variables fixed, a 1-day increase in feeling pain would result in a 0.039 (
Results of the final linear regression and logistic regression models predicting cognitive risk scores.
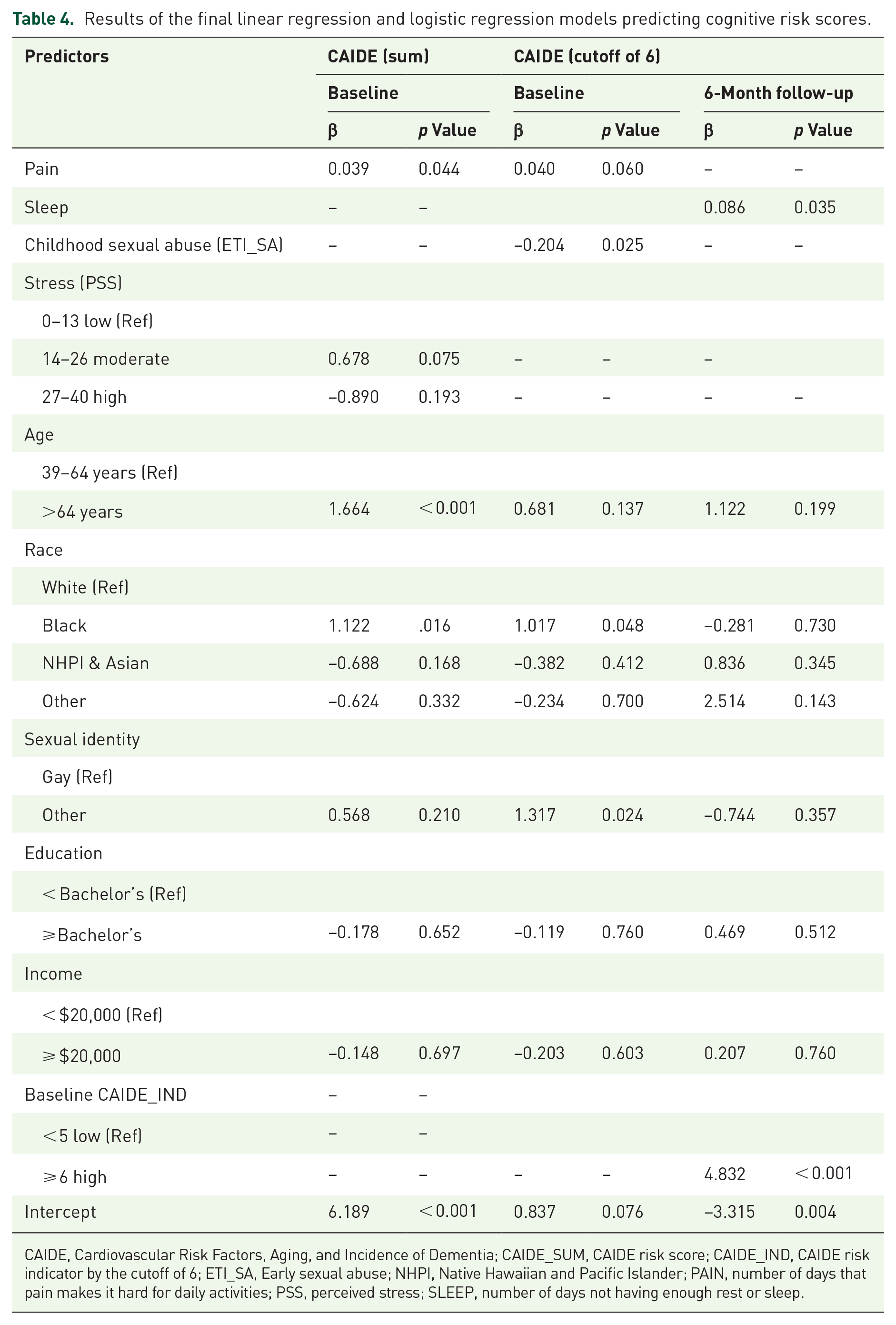
CAIDE, Cardiovascular Risk Factors, Aging, and Incidence of Dementia; CAIDE_SUM, CAIDE risk score; CAIDE_IND, CAIDE risk indicator by the cutoff of 6; ETI_SA, Early sexual abuse; NHPI, Native Hawaiian and Pacific Islander; PAIN, number of days that pain makes it hard for daily activities; PSS, perceived stress; SLEEP, number of days not having enough rest or sleep.
Discussion
This analysis examined a range of biopsychosocial predictors in relation to the risk of cognitive impairment among PLWH as measured by CAIDE scores and identified associations of pain, stress, race, sexual abuse, sexual identity, and age with CAIDE score. It is one of the first studies to examine CAIDE scores in sexual minorities (specifically men who have sex with men) and among few studies to address CAIDE scores in PLWH.
This analysis modeled both incremental change in CAIDE score and the dichotomous high-risk category based on CAIDE score. While risk scores such as CAIDE are traditionally used to identify high-risk categories with a cutoff value, 65 there is also utility in understanding factors that impact more subtle change in CAIDE score. 64 Incremental changes in CAIDE score are associated with both biological and behavioral indicators of cognitive impairment such as hippocampal volume 66 and symptoms of cognitive impairment. 67 Moreover, researchers have suggested that dementia risk scores such as CAIDE are suitable proximal outcomes for interventions targeting risk for dementia emphasizing that exclusive focus on cutoff values limits responsiveness and ability to detect intervention effects in trials. 64 Thus, the present analysis provides insight into factors associated with both incremental change and the highest risk category based on cutoffs.
Importantly, this analysis identified modifiable correlates with CAIDE scores, which included pain and stress. Pain was associated both with an incremental increase in CAIDE score and having an elevated CAIDE score. The relationship between self-reported pain and cognitive impairment appears to be complex and bidirectional; however, much of this literature is examining the relationship between self-reported pain and symptoms of cognitive decline rather than risk for cognitive decline.68–71 If pain is associated with earlier stages of cognitive decline such as CAIDE risk scores, this may indicate an opportunity for early intervention that could disrupt or slow the progression of these conditions. Stress was associated with an incremental increase in CAIDE score, but not with an elevated CAIDE score. Previous research also corroborates that mid-life stress contributes to cognitive decline risk later in life. 47 Given that minority stress and HIV-related stigma can lead to increased stress, it is possible that minority stress processes contribute to accelerated cognitive decline in MSM and other sexual or gender minorities. 72 Thus, interventions that address stigma, minority stress, and/or general stress may contribute to slowing this process. Such interventions may include mindfulness interventions, positive affect interventions, LGB-affirming cognitive behavioral therapy, structural stigma interventions, and others. Of course, most of the indicators for CAIDE are in themselves modifiable through lifestyle interventions, diet, and exercise.
Additionally, this analysis identified nonmodifiable characteristics that may be useful in targeting interventions for cognitive impairment risk reduction among gay and bisexual men living with HIV. These include race, age, and sexual identity. Black racial identity was associated with an incremental increase in CAIDE score and an elevated CAIDE score, while having a sexual identity other than gay was associated with an elevated CAIDE score and older age was associated with an incremental increase in CAIDE score. Interventions should particularly aim to address modifiable risk factors for cognitive impairment among Black MSM, older MSM, and MSM who identify as bisexual or another identity. This suggests the need to improve reach for Black and bisexual men in interventions seeking to reduce cognitive risk. It also may indicate the need for culturally appropriate or culturally adapted intervention strategies such as interventions that center Black and bisexual experiences to maximize the effectiveness of interventions.
Perhaps surprisingly, the analysis indicated a negative association between childhood sexual abuse and lower CAIDE scores. Though, as established earlier in the literature review, the relationship between childhood trauma and cognitive decline later in life is inconsistent,13,31–33 most of the broader health literature links childhood trauma to negative health outcomes including CAIDE-related indicators such as obesity. 73 Pathways between childhood trauma and adult health outcomes include health behaviors, social factors, cognitive patterns, and emotional well-being. 74 Existing literature also suggests that there may be nuance in the relationship between childhood sexual abuse and health including a dose-effect in regard to the severity of abuse, 75 and possible differences by age of occurrence. 76 The measurement used in this study did not discern between these nuances, which may contribute to the observed significant effect. It is also plausible that childhood sexual abuse histories may be associated with a protective factor for example: resilience. Though we did not observe a significant association between childhood abuse and resilience, the association between resilience and childhood sexual abuse among MSM and PLWH is a newer subject of research. There is indication that resilience may moderate or mediate the relationship between childhood sexual abuse and outcomes such as mental health. 77 Findings about the relationship between childhood sexual abuse and resilience are mixed, 77 but some studies have found elevated resilience in people with childhood sexual abuse histories.78,79 Qualitative findings suggest that adverse experiences in childhood may trigger someone to develop resilience as a coping process, 80 which may indicate that resilience developed in coping with one type of adverse experience (sexual abuse) may be transferable to future adversities or challenges. 77 In the present study, we measured resilience as an individual-level coping strategy, though resilience may be conceptualized as multilevel. 77 Though currently limited in their application in the literature addressing HIV, positive frameworks such as resilience, positive variation, or asset-based approaches may lead to insights why some people who experience negative exposures achieve positive health outcomes. 81
Limitations
This analysis should be considered with a few notable limitations. These include that this convenience sample was collected in Honolulu and Philadelphia and may not be generalizable to all populations within the U.S. Although smartphone coverage is high in the U.S. (90% on average), it is lower among the oldest and lowest income groups (roughly 80%), meaning that there may be some selection bias due to the use of CASI.
46
Post-hoc power analyses indicate that the present study was likely underpowered to detect small-effect sizes at the
Conclusion
Cognitive impairment among MSM living with HIV is a critical HIV-related comorbidity. The present analysis identified modifiable correlates of cognitive risk and relevant subpopulations that may be emphasized in interventions to reduce cognitive risk. Future projects should seek to address pain, stress, and cognitive impairment risk, particularly among older, Black, nongay MSM living with HIV.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241249657 – Supplemental material for Examining biopsychosocial predictors of risk for cognitive impairment among a racially diverse sample of men who have sex with men living with HIV
Supplemental material, sj-docx-1-tai-10.1177_20499361241249657 for Examining biopsychosocial predictors of risk for cognitive impairment among a racially diverse sample of men who have sex with men living with HIV by Casey D. Xavier Hall, Beth Okantey, Zhuo Meng, Crim Sabuncu, Brittany Lane, Eugenia Millender, Artur Queiroz, Jung Hyo Kim, Lorie Okada, Avrum Gillespie, Gina Simoncini, John ‘Jack’ P. Barile, Grace X. Ma and Frank ‘Frankie’ Y. Wong in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.