
Abstract
Introduction:
Brucellosis is a common global zoonotic disease with a wide range of complex and nonspecific clinical manifestations that may lead to misdiagnosis and delayed treatment. Osteoarticular involvement is the most common complaint in brucellosis.
Objective:
This present study aims to describe the clinical and laboratory characteristics and treatment of brucellosis patients with arthritis and sacroiliitis.
Methods:
This retrospective descriptive study was performed on patients presenting to a teaching hospital in Kermanshah, Iran with a diagnosis of brucellosis from 2011 to 2019. The demographic and clinical characteristics, complications, laboratory findings, and treatment were recorded during the study period. Then, the difference in the collected data was investigated between brucellosis patients with and without arthritis or sacroiliitis.
Results:
Of 425 patients studied, 130 (30.58%) had osteoarticular involvement. Among them, 41 (9.64%) and 58 (13.6%) patients were diagnosed with arthritis and sacroiliitis, respectively. There were no significant demographic differences between patients with and without brucellar arthritis or sacroiliitis (p > 0.05). The patients with Brucella arthritis had a significantly higher frequency of arthralgia and radiculopathy (p ⩽ 0.05). Sacroiliitis was significantly more common in patients with arthralgia, neck pain, and low back pain, positive flexion-abduction-external rotation (FABER) test, radiculopathy, and vertebral tenderness compared to patients without sacroiliitis (p ⩽ 0.05), while fever and headache were significantly more common in patients without sacroiliitis (p ⩽ 0.05). The median Wright and 2-Mercapto Ethanol titers were higher in brucellosis patients with arthritis or sacroiliitis versus patients without arthritis or sacroiliitis, but the difference was not significant (p > 0.05). Synovial fluid had been analyzed in 20 cases. The mean white blood cell count, glucose, and protein level were 3461 ± 2.70 cells/mm3, 58.54 ± 31.43 mg/dL, and 8.6 ± 11.85 g/dL, respectively. In 80% of the subjects, neutrophil cells were predominant. There were no significant laboratory differences between patients with and without brucellar arthritis or sacroiliitis, except for a higher median platelet count in patients with arthritis and higher median levels of aspartate aminotransferase (AST) and alkaline phosphatase (ALP) in patients with sacroiliitis. Most cases of arthritis and sacroiliitis were diagnosed with ultrasound (31.8%) and FABER test (79.3%), respectively.
Conclusion:
Arthritis and sacroiliitis were the two most important and common manifestations of brucellar osteoarthritis with a frequency of 9.64% and 13.6%, respectively. Any complaints of low back pain and radiculopathy as well as the presence of spondylitis in patients should raise suspicion of sacroiliitis. High levels of AST and ALP and a high platelet count may be associated with brucellar sacroiliitis and arthritis, respectively. The use of imaging methods such as MRI and bone scan seems necessary for the diagnosis of sacroiliitis.
Introduction
Brucellosis, also known as undulant fever, Malta fever, and Mediterranean fever, is one of the most common zoonoses worldwide. It is caused by the genus Brucella, an intracellular Gram-negative bacterium. The genus Brucella consists of 12 species, of which four are the main causes of the disease in humans, including B. melitensis, B. abortus, B. suis, and B. canis.1,2 Annually, at least 500,000 new human cases of brucellosis are identified worldwide, and it is estimated that there are four unidentified cases beside each identified case. 3 Approximately 29% of dairy products in the Middle East are contaminated with Brucella, and raw cow’s milk seems to be the most contaminated dairy product in the region. 4
Reticuloendothelial system involvement throughout the body causes a wide range of clinical symptoms. Brucellosis manifestations mimic the clinical picture of many other infectious and non-infectious diseases. Osteoarticular problems alongside fever and fatigue are the most common findings in brucellosis. The rate of osteoarticular involvement varies from 10% to 85% in various studies. The type of osteoarticular involvement depends on many factors such as the patient’s age so monoarthritis, sacroiliitis, and spondylitis are more common in children, adults, and the elderly, respectively. 5
Brucellar peripheral arthritis has been reported in both reactive and septic forms. Knee mono arthritis is the most common type of peripheral joint involvement in most studies. 6 Failure in diagnosis may lead to permanent injuries and disabilities due to osteomyelitis, bone destruction, joint effusion, and abscess. It is not difficult to diagnose knee joint arthritis, which is also common. However, it is challenging to diagnose arthritis of other joints such as the hip in which a delayed diagnosis leads to necrosis of the femoral head and dislocation. 7
Brucellar sacroiliitis can lead to severe motor disabilities. Its prevalence has been reported up to 80% in patients with focal complications (5). It is one-sided in 80% of the cases. Sacroiliitis causes severe back pain that radiates to the lower extremities and mimics the features of a lumbar disc herniation in most cases. However, about 24% of brucellar sacroiliitis cases are asymptomatic and detected by imaging. The flexion-abduction-external rotation (FABER) test and radiography are very helpful in confirming sacroiliac joint involvement, although they are not specific. In addition, CT scans, MRIs, and bone scans are also helpful. 8
Iran as a developing country has a traditional livestock industry with a brucellosis rate of 238.6 per 100,000 making it an endemic area. It should be noted that the incidence of the disease is not the same in all parts of the country and the main foci are located in the western and northwestern provinces such as Kurdistan, Lorestan, Hamedan, Kermanshah, South Khorasan, and northern provinces. 9 According to a recent systematic review and meta-analysis study conducted in Iran, the annual incidence of Brucella is estimated at 276.42 in 100,000 in Kermanshah Province, which is the highest among the provinces of Iran. 10 Brucellosis can irreversibly hurt the economy of the country by involving the youth in the workforce. Although it is rarely fatal, diagnostic challenges such as nonspecific clinical signs and slow growth in culture specimens, which result in a delayed diagnosis, lead to severe disabilities. 11 Therefore, the objective of this study was to establish the frequency, clinical manifestations, and para-clinical characteristics of brucellar arthritis and sacroiliitis in patients presenting to a referral hospital in the west of Iran.
Material and methods
The medical records of all patients admitted to Imam Reza Referral University Hospital in Kermanshah Province, Western Iran, were retrospectively searched to find patients suspicious of brucellosis at the time of hospital admission during an 8-year period between 2011 and 2019. The inclusion criterion was hospitalization with a diagnosis of brucellosis during the study period. Patients with incomplete medical records, duplicate records based on name, ID number, and gender were excluded. Data including demographic and epidemiological characteristics, clinical manifestations, imaging data, treatment regimens used, and length of hospital stay were collected from the medical records of brucellosis patients. Furthermore, the medical records of the patients with arthritis or sacroiliitis were selected for further evaluation.
Case definition
Brucellosis was diagnosed as per the national guidelines (Iranian Center for Disease Control, ICDC, 2012) including isolation of Brucella species from the blood or other fluids or bone marrow culture, a compatible clinical picture with brucellosis (arthralgia, fever, perspiration, malaise, liver and spleen enlargement, and signs of sacroiliac or peripheral joint involvement) with standard tube agglutination titer (SAT) ⩾1/80, and a titer of ⩾1/40 for 2-mercaptoethanol (2ME) Brucella agglutination test. Sacroiliitis was defined as inflammation of the sacroiliac joint diagnosed by a positive FABER test in clinical examination or the presence of suggestive changes in a radionuclide bone scan or MRI. Peripheral arthritis was diagnosed with peripheral joint effusion with any sign of inflammation on clinical examination, ultrasound or MRI, or leukocytosis in synovial fluid analysis. The patients were categorized into acute (<3 months) and chronic (>3 months) brucellosis based on the duration of the disease before hospital admission. Relapse was considered as a history of brucellosis with improvement within 3 months, and reinfection was defined as a history of brucellosis more than 3 months.
Statistical analysis
The SPSS software version 16 was used for statistical analysis (SPSS Inc., Chicago, IL, USA). The Shapiro–Wilk test was used to evaluate the normal distribution of the data in each group. Continuous variables with a normal distribution are presented as mean ± standard deviation (SD), and data without a normal distribution are presented as median (IQR). Categorical variables are described as frequency and percentage. To compare brucellosis patients with arthritis or sacroiliitis with those without arthritis or sacroiliitis, t-test, chi-square, and Fisher’s exact tests were used for variables with normal distribution, and Mann–Whitney and rank sum tests were applied to variables with an abnormal distribution. p Values < 0.05 were considered statistically significant.
Results
From 21 March 2011 to 20 March 2019, 740 medical records with a diagnosis of brucellosis were screened for enrolment. Of 740 screened medical records, 425 were eligible for inclusion in the study.
Demographic and clinical characteristics of patients with brucellosis
Of 425 patients, 180 were female and 245 were male with a mean age of 43.2 ± 17.5 years (range: 12–83 years). 74.8% of the patients were involved acutely, 18.3% were involved chronic and the duration of involvement in 6.8% of the patients was unknown. Recurrence and relapses were found in 18.93% and 11.66% of patients, respectively. Of 425 patients studied, 130 (30.58%) had osteoarticular involvement. Sacroiliitis (13.6%) was the most common type of osteoarticular complication followed by spondylitis (12.9%) and peripheral arthritis (9.6%). The demographic, epidemiological, and clinical characteristics and laboratory findings of brucellosis patients are shown in Table 1.
Clinical and demographic characteristics and laboratory findings of brucellosis patients in Imam Reza Hospital, Kermanshah, Iran, during an 8-year period between 2011 and 2019.

FABER, flexion-abduction-external rotation.
Demographic and clinical manifestations and laboratory findings of Brucella arthritis patients
During the study period, 41 patients (9.6%) with brucellar arthritis were diagnosed. In all, 33 cases (80.48%) had acute and five cases had chronic brucellosis. The chronicity status was unknown in three cases. A previous history of brucellosis was recorded in the records of 28 patients. Relapses and re-infection were found in 2.43% and 7.31% of patients, respectively. The knee (58.53%), hip (17.07%), and ankle (9.75%) were the most common joints involved. One patient (2.43%) had elbow involvement and one (2.43%) had sternoclavicular involvement. The most common type of peripheral arthritis was monoarticular arthritis (95.4%).
Only four patients with peripheral arthritis had oligoarticular patterns (two cases had bilateral hip involvement, one had bilateral knee and hip involvement, and one had knee and hip involvement). Five cases (12.19%) had discopathy and three cases (7.31%) had rheumatoid arthritis. The demographic and clinical characteristics of brucellosis patients with and without arthritis or sacroiliitis are shown in Table 2.
Clinical and demographic characteristics of brucellosis patients with and without arthritis or sacroiliitis.

FABER, flexion-abduction-external rotation.
Most cases of arthritis were diagnosed by ultrasound (13 cases, 31.8%) and arthrocentesis (11 cases, 26.8%). MRI was used in only three cases (7.3%). The diagnosis of arthritis was clinical in only three patients and different diagnostic methods were used in 11 (26.8%) patients.
Synovial fluid was analyzed in 20 cases. The mean white blood cell (WBC) count, glucose, and protein levels were 3461 ± 2.70 cells/mm3, 58.54 ± 31.43 mg/dL, and 8.6 ± 11.85 g/dL, respectively. WBC differentiation of synovial fluid was done for 19 patients. In 80% of the subjects, neutrophil cells were predominant (Table 3). The Wright test was positive with titers of 1.20 and 1.160 in the synovial fluid of two patients.
Laboratory findings of synovial fluid.

A triple regimen containing an aminoglycoside, doxycycline, and rifampin (58.5%) was the most common regimen prescribed by doctors for patients with Brucella arthritis. Furthermore, seven patients (17.1%) received double therapy with doxycycline and rifampin. Other patients (24.4%) received different regimens with two to four drugs including the above drugs plus Co-trimoxazole, ciprofloxacin, and ceftriaxone. Three patients (7.31%) with knee involvement eventually required arthroscopy/arthrotomy.
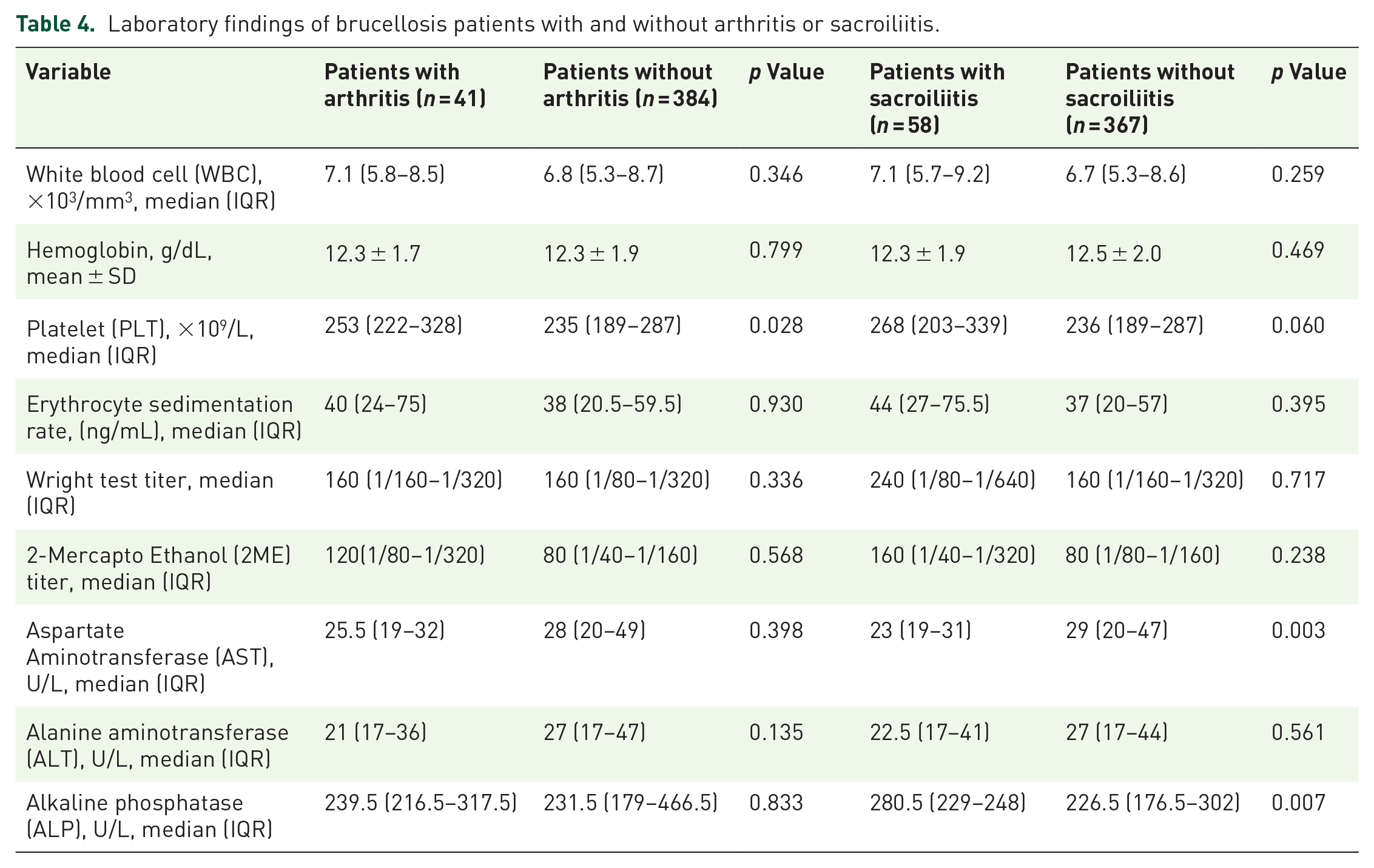
No differences were observed in the demographic characteristics between patients with and without arthritis. The patients with arthritis had a significantly higher frequency of arthralgia and radiculopathy (p ⩽ 0.05). The median Wright and 2ME titers were higher in patients with arthritis compared to patients without arthritis, but the difference was not statistically significant (p > 0.05). There were no significant laboratory differences between the patients with and without brucellar arthritis, except for a higher median platelet count in patients with arthritis (Table 4).
Laboratory findings of brucellosis patients with and without arthritis or sacroiliitis.
Demographic and clinical manifestations and laboratory findings of Brucella sacroiliitis patients
Among 425 brucellosis patients, 58 (13.6%) had sacroiliitis. The majority of the patients were in the acute stages of brucellosis (72.41%), 13 (22.41%) had chronic brucellosis, and 3 cases were unknown. Relapse and re-infection were found in 5.1% (three cases) and 12.06% (seven cases) of the patients, respectively.
Most cases of sacroiliitis were diagnosed with a positive FABER test on physical examination (46 cases, 79.3%). MRI and bone scan were used for 7 (12.06%) and 5 (8.62%) patients. Sacroiliitis was unilateral in the majority of the patients (51 cases = 87.93%). Sacroiliitis was bilateral in only seven patients (12.06%), and 6.89% of the patients showed concomitant sacroiliitis with discopathy.
In all, 38 patients (65.5%) received triple combination therapy with doxycycline, rifampin, and aminoglycoside, and six patients (10.4%) received double combination therapy with doxycycline and rifampin. Other patients (24.1%) received different regimens of 2–4 drugs including the above drugs with Co-trimoxazole, ciprofloxacin, and ceftriaxone.
Sacroiliitis was significantly more frequent in patients with arthralgia, neck pain, and back pain versus patients without sacroiliitis (p ⩽ 0.05), while fever and headache were significantly more common in patients without sacroiliitis (p ⩽ 0.05). Although the median Wright and 2ME titers were higher in patients with sacroiliitis compared to patients without sacroiliitis, the difference was not statistically significant (p > 0.05). A significant difference was found in alkaline phosphatase (ALP) and aspartate transaminase (AST) values between patients with and without sacroiliitis (p ⩽ 0.05). Laboratory and serologic findings of the patients with and without sacroiliitis are shown in Table 4.
Discussion
Brucellosis is one of the most common zoonotic diseases in Iran. The latest national cohort study conducted to estimate the incidence of brucellosis in Iran showed that the incidence rate is 21.78 per 100,000. 12 The present study investigated the frequency, clinical manifestations, laboratory findings, diagnosis, and treatment of brucellosis patients with arthritis or sacroiliitis admitted to a university hospital in the west of Iran. The frequency of osteoarticular complications in our study was 30.58% which is similar to a prospective cohort study performed in India (34%). 13 A systematic review and meta-analysis estimated the prevalence of osteoarticular brucellosis at 27% and 36% in low-risk and high-risk regions, respectively. 6 A study done in Iran reported that spondylitis (51.6%) was more common than peripheral arthritis (25.8%) and sacroiliitis (22.5%), 14 while a study conducted in China found that peripheral arthritis (57%) was more frequent than spondylitis (20%) and sacroiliitis (2%). 15 We found that the most common manifestation was sacroiliitis (13.6%) followed by spondylitis (12.9%) and peripheral arthritis (9.6%). These contradictory results could be due to differences in the sample size, Brucella species, study population, environmental factors, age, disease duration, and diagnostic methods.
The frequency of peripheral arthritis was 9.6% in the present study. No difference was observed in gender between brucellosis patients with and without arthritis. The most common type of arthritis was monoarticular in our patients, which mainly occurred in lower limbs such as the knee and hip, as reported in most studies.16–18 In addition, the frequency of sacroiliitis was 13.6% in the present study. The frequency of sacroiliitis has been reported up to 75% in some studies. 5 It is noteworthy that in the study area, diagnosis of sacroiliitis is mainly made based on clinical examination without a bone scan or MRI; therefore, it may be underestimated due to the similarity of the disease symptoms with discopathy and low back pain, which is a common complaint in patients with brucellosis. Sacroiliitis was mostly unilateral in previous studies, which is similar to the present study.19–22 El Desuki used bone scans in patients diagnosed with unilateral sacroiliitis and reported that about 65% of the patients had bilateral involvement in the sacroiliac joints. 23 The author proposed that the frequency of bilateral involvement might be higher than previously thought. Considering the infrequent use of imaging techniques for diagnosing Brucella sacroiliitis in this study, this finding needs further investigation.
Arthralgia and radiculopathy were the most common complaints in arthritis patients and were reported more frequently than fever and chills. Other symptoms and signs were not significantly different in patients with arthritis. Back pain, neck pain, sweating, and arthralgia are significantly more reported in patients with sacroiliitis. Our results showed that in sacroiliitis patients, the frequency of positive FABER test, radiculopathy, and vertebral tenderness was significantly higher than in other patients. In most studies, fever and chills, arthralgia, and back pain were the most common complaints of brucellosis.24–27 The higher proportions of some variables such as radiculopathy, vertebral tenderness, low back pain, and neck pain in sacroiliitis patients in this study could reflect the coincidence of spondylitis with sacroiliitis in some patients. So about 25% of sacroiliitis patients had concomitant spondylitis (data not shown). Sacroiliitis mimics the symptoms of a lumbar spine hernia, which causes back pain, a common complaint in these patients. It should be noted that discopathy has been reported as a confounding factor (comorbidity) in 89.6% of sacroiliitis patients8,21 On the other hand, the lower proportions of general symptoms such as fever and headache in patients with sacroiliitis compared to patients without sacroiliitis may be due to temporary amnesia caused by severe pain of the sacroiliac joint.
There were no significant hematologic and biochemical changes between patients with and without arthritis. Nonetheless, the patients with arthritis had a significantly higher platelet count compared to patients without arthritis (p = 0.028). A previous study showed that high platelet counts within the normal range were significantly associated with knee and hip osteoarthritis. 28 Platelet count disorders in brucellosis occur both in thrombocytopenia and thrombocytosis.29,30 Platelets have been extensively described as a source of prothrombotic agents associated with inflammatory markers and play a role in the initiation and progression of vascular and inflammatory diseases. It has been suggested that platelets play a key role in the development of various autoimmune diseases, such as rheumatoid arthritis and systemic sclerosis through the production of IFN-α by dendritic cells activated by immune complexes. 31 It has also been suggested that platelet distribution width, an indicator of platelet function and activation, can be useful in the initial evaluation of patients in the challenging diagnosis of infection-related diseases that can affect platelet counts. 32 In the present study, alkaline phosphatase had significantly higher values in patients with sacroiliitis compared to others (p = 0.007). High ALP levels have been reported in various types of sacroiliitis such as spondyloarthropathy, postpartum sacroiliitis, and a case of sacroiliitis with a spinal cord injury.33,34 In addition, it has been reported that increased serum ALP levels may be associated with disease severity in spondyloarthropathy.30–32
The most common method for diagnosing brucellar arthritis in the patients was ultrasound (31.8%). Ultrasound is extensively used in our province since it is affordable, and is not time-consuming. This method is less invasive than synovial fluid tests and the patients are more cooperative. Various studies have been performed on the advantages of ultrasound in the early detection of arthritis. However, the recommended method is MRI for accurate diagnosis of the severity of the disease and follow-up of the response to treatment as well as diagnosis in deeper joints. Ultrasound is more suitable for outpatients compared to hospitalized patients.35,36 Most cases of brucellar sacroiliitis in our study were diagnosed with clinical examination without using para-clinical methods. It can explain the lower frequency of sacroiliitis in the area under study. 14
Sacroiliitis is a diagnostic challenge since it imitates other diseases. Bone scans can help diagnose unknown cases. The helpful role of fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) has been shown in recent studies. 37 However, CT scans and MRIs are needed to accurately determine the process, severity, and complications of the disease.23,38 The radiologist’s report may even miss sacroiliitis, as previously reported in the diagnosis of sacroiliitis, there may be moderate intra-observer agreement in the interpretation of plain radiographs and MRI. Therefore, in cases of suspected brucellosis, it is important that the interpretation of plain radiography and sacroiliac MRI be evaluated by a panel of several physicians to ensure that the diagnosis is not missed.39,40
In the present study, synovial fluid analysis was requested for 21 patients to diagnose Brucella arthritis, and its results were recorded. Synovial fluid analysis showed a decrease in glucose level and an increase in protein level and WBC count (neutrophil predominance) similar to some previous findings. 41 In contrast to our findings, some studies reported the predominance of lymphocytes in the synovial fluid.42,43 It should be noted that the sample size of all the studies mentioned was smaller than our study. In general, even in the presence of a negative culture for Brucella organism, septic involvement cannot be definitively ruled out; therefore, synovial biopsy is an invasive procedure that is mostly unnecessary. 44 If a cutoff of 50,000 cells/mm3 is accepted for septic arthritis, our samples indicated reactive involvement. It should be noted that the synovial fluid Wright test titer was positive in two cases, which confirms a reactive involvement although this cutoff was questioned recently. McGillicuddy found that a synovial fluid WBC cutoff of 50,000/mm3 lacked the sensitivity required to be clinically useful in ruling out infectious arthritis. 45
In the present study, the most frequent treatment regimen in both groups of brucellosis patients with arthritis and sacroiliitis was triple therapy with rifampin + aminoglycosides + doxycycline similar to a study by Al Nokhata et al. 24 However, they reported a 10% recurrence of brucellosis. Generally, the relapse rate is reported 5–30% in various previous studies with similar diets. 46 Due to the retrospective nature of our study, it was not possible to follow up with the patients to report the recurrence rate of the patients considering the treatment received. Another common regimen was the doxycycline + rifampin regimen. However, this regimen is recommended for individuals without complications and regional involvement.47,48 In general, the choice of treatment regimen depends on the experience and opinion of the physician and the characteristics of brucellosis in the area and the affected person.
This study had some limitations. The first limitation was the retrospective nature of the study, which did not allow completion of missing data and follow-up of the patients. Second, synovial fluid analysis was performed for a small number of patients and lacked culture in bacteriological media, which made it impossible to accurately determine whether the arthritis was septic or reactive. Third, because of the low sample size, the interpretation of the results might not represent the larger population. Fourth, most patients with Brucella sacroiliitis were diagnosed based on clinical manifestations (positive FABER test) without corroborating imaging exams. Therefore, it is better to consider these people as patients with axial musculoskeletal symptoms suspected of sacroiliitis. Consequently, the results should be interpreted with caution due to this unavoidable limitation. Despite these limitations, the present study provides important perspectives on the clinical and laboratory characteristics of brucellosis patients with arthritis and sacroiliitis in Kermanshah.
Conclusion
In summary, sacroiliitis and arthritis are common complications of brucellosis that should be diagnosed as soon as possible to prevent their irreversible consequences. Any complaints of low back pain and radiculopathy as well as the presence of spondylitis in patients should raise suspicion of sacroiliitis. The use of imaging methods such as MRI and bone scan seems necessary for the diagnosis of sacroiliitis. High levels of AST and ALP and a high platelet count may be associated with brucellar sacroiliitis and arthritis, respectively. Due to the endemicity of brucellosis in Kermanshah Province, it is recommended to set up a disease registry system to improve the registration of the patient’s medical records and their follow-up to facilitate data collection on recurrence and drug compliance for proper diagnosis and treatment.
Footnotes
Acknowledgements
The authors want to thank their colleagues at Imam Reza Therapeutic Educational Hospital of Kermanshah, Iran for their contribution to the patient’s diagnosis. We also extend our thanks to the clinical research development center of Imam Reza Hospital affiliated to Kermanshah University of Medical Sciences for their kind support.