
Abstract
Background:
Emerging risk factors highlight the need for an updated understanding of cryptococcosis in the United States.
Objective:
Describe the epidemiological trends and clinical outcomes of cryptococcosis in three patient groups: people with HIV (PWH), non-HIV-infected and non-transplant (NHNT) patients, and patients with a history of solid organ transplantation.
Methods:
We utilized data from the Merative Medicaid Database to identify individuals aged 18 and above with cryptococcosis based on the International Classification of Diseases, Tenth Revision diagnosis codes from January 2017 to December 2019. Patients were stratified into PWH, NHNT patients, and transplant recipients according to Infectious Diseases Society of America guidelines. Baseline characteristics, types of cryptococcosis, hospitalization details, and in-hospital mortality rates were compared across groups.
Results:
Among 703 patients, 59.7% were PWH, 35.6% were NHNT, and 4.7% were transplant recipients. PWH were more likely to be younger, male, identify as Black, and have fewer comorbidities than patients in the NHNT and transplant groups. Notably, 24% of NHNT patients lacked comorbidities. Central nervous system, pulmonary, and disseminated cryptococcosis were most common overall (60%, 14%, and 11%, respectively). The incidence of cryptococcosis fluctuated throughout the study period. PWH accounted for over 50% of cases from June 2017 to June 2019, but this proportion decreased to 47% from July to December 2019. Among the 52% of patients requiring hospitalization, 61% were PWH and 35% were NHNT patients. PWH had longer hospital stays. In-hospital mortality at 90 days was significantly higher in NHNT patients (22%) compared to PWH (7%) and transplant recipients (0%). One-year mortality remained lowest among PWH (8%) compared to NHNT patients (22%) and transplant recipients (13%).
Conclusion:
In this study, most cases of cryptococcosis were PWH. Interestingly, while the incidence remained relatively stable in PWH, it slightly increased in those without HIV by the end of the study period. Mortality was highest in NHNT patients.
Plain language summary
The epidemiology and outcomes of cryptococcosis across the United States have not been recently examined. This study analyzed an insured population from 2017 to 2019 and revealed a relatively stable incidence of cryptococcosis among people with HIV, while concurrently demonstrating a slightly increased incidence among individuals without HIV. Notably, mortality rates were highest among non-HIV-infected and non-transplant patients.
Introduction
The increasing number of cases following solid organ transplantation and in individuals considered phenotypically normal without immunosuppressive risk factors is a growing concern.15,16 Reports have identified a rising trend in NHNT patients, attributed to various factors such as malignancies, autoimmune diseases, hepatic cirrhosis, COVID-19, and the use of immunosuppressive medications.6 –14 Despite the presence of recognized risk factors for cryptococcosis, approximately 30% of cases in the United States occur in individuals who lack any obvious clinical predisposition.9,16
Moreover, there are often delays in diagnosing cryptococcosis, 17 indicating a lack of suspicion, especially in patients with non-traditional risk factors. Notably, individuals without HIV tend to experience a longer duration from initial presentation to diagnosis (ranging from 26 to 68 days versus 22 days), despite exhibiting symptoms for a longer period compared to PWH (44 days versus 19 days). 18 These delays in diagnosis contribute to poorer outcomes.
These findings underscore the need for improved recognition of individuals susceptible to cryptococcosis beyond those with HIV, particularly due to the increasing prevalence of immunosuppressive diseases and the widespread use of immunosuppressive medications. Therefore, this study aimed to refine our understanding of the complex and evolving landscape of cryptococcosis in the United States. The objectives were to describe the epidemiology and clinical outcomes of cryptococcosis across the United States, with a specific focus on the three distinct patient groups defined by the current IDSA guidelines: (1) PWH, (2) NHNT patients, and (3) patients with a history of solid organ transplantation. 1
Methods
Study design and population
We used data from the Merative Medicaid Database (formerly IBM® MarketScan® Medicaid Database) between January 2017 and December 2019 due to database availability in accordance with our institutional use agreement. This database encompasses adjudicated health insurance claims for over 44 million Medicaid enrollees from 8 to 12 unidentified, geographically diverse states. It includes hospital discharge diagnoses, outpatient diagnoses and procedures, outpatient pharmacy claims, and ethnicity information. Medicaid primarily covers publicly insured individuals, including low-income adults, elderly individuals, children, pregnant women, and persons with disabilities. 19 Therefore, Medicaid beneficiaries generally exhibit a higher prevalence of comorbidities and experience greater socioeconomic disadvantage and overall vulnerability compared to commercially insured beneficiaries. 20 The database is fully de-identified and contains none of the data identifiers prohibited by the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. Therefore, the University of Georgia Institutional Review Board determined that review and approval were not required (PROJECT00006726).
We included patients aged 18 years and above diagnosed with cryptococcosis based on the International Classification of Diseases, Tenth Revision (ICD-10-CM) diagnosis codes (Supplemental Table S1). 21 We designated the index date as the first instance in which the diagnosis code was used during the study period. Patients had to have maintained continuous health plan enrollment for 6 months preceding the index date, with no restrictions applied to enrollment after this date. Patients with insurance plans who did not contribute data to the database were excluded. When a patient had multiple encounters coded for cryptococcosis, we considered the earliest coded encounter as the index encounter.
Patients were categorized into one of three groups based on the IDSA clinical guidelines for managing cryptococcal disease, 1 HIV, NHNT, and solid organ transplant, depending on comorbidities recorded prior to or during the index encounter (Supplemental Table S2).
We determined the demographic characteristics based on the index date and included age, sex, race, and type of health insurance plan as recorded in the database (Supplemental Table S3). We assessed underlying comorbidities using ICD-10-CM diagnosis codes for each group, including HIV, solid organ transplantation, systemic connective tissue disorders, immunodeficiencies, type 2 diabetes mellitus (DM), malignancies, hepatic fibrosis and cirrhosis, heart failure, noninfective enteritis and colitis, chronic kidney disease (CKD), and chronic lower respiratory diseases (Supplemental Table S2).
For PWH, receipt of ART was established by the presence of at least one pharmacy claim for antiretroviral medications identified by the national drug code (Supplemental Table S4) within 3 months before the index date.22,23 ART was defined as a single tablet regimen (STR) or using two or more single antiretroviral medications or fixed-dose combination products containing two or more single antiretroviral medications.
We selected the clinical spectrum of cryptococcosis based on ICD-10-CM diagnosis codes, including pulmonary, disseminated, central nervous system (CNS), cutaneous, osseous, other forms, and unspecified cryptococcosis (Supplemental Table S1). We plotted diagnoses and types of cryptococcosis for each 6-month interval over the study period and stratified the proportion of cryptococcosis across the different groups to capture trends over time.
We collected data on the place of service and provider type, stratified by outpatient and inpatient settings (Supplemental Table S5). Outpatient provider type was identified within 30 days of the index date, whereas inpatient provider type was established during hospitalization. Patients receiving inpatient and outpatient services on the same day were classified as inpatient. For patients whose initial diagnosis was outpatient, we determined the rate of subsequent cryptococcosis-related hospitalization.
Among patients with inpatient service records, we evaluated clinical symptoms and findings suggestive of cryptococcosis within 90 days before or 30 days after the index date, including the index date, using ICD-10-CM diagnosis codes (Supplemental Table S6). We also examined hospitalization characteristics related to cryptococcosis, such as the length of stay, patient status at discharge, and infectious diseases (ID) consultation. Receipt of services from critical care providers was used as a proxy to determine whether patients required treatment in an intensive care unit. Procedures conducted within 30 days of the index date were identified using Current Procedural Terminology (CPT) codes, including a composite of diagnostic or therapeutic lumbar puncture (LP) and ventriculostomy or external ventricular drain (VD), per patient across groups (Supplemental Table S7). The Elixhauser Comorbidity Index was calculated for readmissions and in-hospital mortality using ICD-10-CM diagnosis codes for 29 comorbidities present on the index date. 24 In-hospital mortality was determined for inpatient admissions within 90 days and 1 year after the index date.
Outcome measures
The primary outcome of this study was to assess the demographics, underlying comorbidities, and the types of cryptococcosis, among PWH, NHNT patients, and those with a history of transplant. The secondary outcomes included comparing baseline characteristics, clinical symptoms suggestive of cryptococcosis, rates of procedures, provider types, length of hospitalization, and in-hospital mortality among hospitalized patients in the three groups.
Statistical analysis
Descriptive statistics were employed to present the demographic and clinical characteristics of PWH, NHNT patients, and transplant patients. Analysis of variance, chi-squared test, and Fisher’s exact test were utilized to examine the association between group and patients’ demographic and clinical characteristics, such as underlying conditions and comorbidities, clinical symptoms and findings suggestive of cryptococcosis, types of cryptococcosis, rate of procedures, hospitalization, length of hospitalization, and in-hospital mortality. Logistic regression and Firth logistic regression models were built to explore the relationship between in-hospital mortality and each patient group, the type of cryptococcosis, and the interaction between these factors, controlling for covariates such as age and gender. 25 Post hoc multiple comparisons with Tukey–Kramer adjustment were used to assess for differences among PWH, NHNT patients, and transplant patients. 26 The statistical analyses were performed using SAS software, version 9.4 (SAS Institute, Inc., Cary, NC, USA).
This study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist (Supplemental Material). 27
Results
Characteristics of all patients with cryptococcosis
A total of 703 patients with cryptococcosis were included, of which 59.7% (n = 420) were PWH, 35.6% (n = 250) were NHNT, and 4.7% (n = 33) had a history of solid organ transplantation (Supplemental Table S8). PWH were younger [median 44 years (first quartile (Q1)−third quartile (Q3) 34–51.5)] than NHNT patients [53 years (Q1–Q3 41–62)] and those with a history of transplant [57 years (Q1–Q3 51–62)]. There were more male patients in the PWH group (73%) than NHNT and transplant groups (59% and 52%, respectively). The majority of PWH (68%) identified as Black, while a larger proportion of NHNT patients (60%) identified as White. White and Black individuals were equally represented among transplant patients (47%), with few Hispanic patients identified in any group.
PWH had fewer comorbidities [median 0 (Q1–Q3 0–1)] than NHNT and transplant patients [1 (Q1–Q3 1–3) and 2 (Q1–Q3 2–4), respectively]. Chronic lower respiratory disease and malignancy were the most common comorbidities across all groups but were more prevalent in NHNT and transplant patients (Supplemental Table S8). Transplant patients had the highest rates of CKD, heart failure, hepatic fibrosis and cirrhosis, malignancy, DM, as well as autoimmune and inflammatory diseases, while other immunodeficient conditions were more frequent among NHNT patients. Among NHNT patients, risk factors for cryptococcosis included chronic lower respiratory disease (37%), malignancy (24%), DM (24%), systemic connective tissue disorders (10%), hepatic fibrosis and cirrhosis (9%), immunodeficiencies (9%), and noninfective enteritis and colitis (8%). Interestingly, 24% (n = 59/250) of NHNT patients had no identified comorbidities.
Notably, 28% (n = 117/420) of PWH had received ART before the index date. Among these individuals, 80% (n = 94/117) were taking an STR, with bictegravir/emtricitabine/tenofovir alafenamide, dolutegravir/abacavir/lamivudine, and elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide being the most common. The remaining 20% (n = 23/117) received two or more individual antiretroviral medications or fixed-dose combinations, most often including dolutegravir or ritonavir- or cobicistat-boosted darunavir with emtricitabine/tenofovir alafenamide or emtricitabine/tenofovir disoproxil fumarate.
Types and incidence of cryptococcosis among all patients
Over the 3-year study period, 60% (n = 423) of patients had ICD-10-CM diagnosis codes for CNS involvement, 14% (n = 101) had pulmonary cryptococcosis, and 11% (n = 78) had disseminated cryptococcosis. Cutaneous and osseous cryptococcosis were rare, with less than 1% observed for each (n = 6 and n = 2, respectively). An additional 20% (n = 143) and 5% (n = 33) were classified as unspecified or other types, respectively. The overlap of multiple types of cryptococcosis based on ICD-10-CM diagnosis codes was infrequent. Only a small number of patients with CNS cryptococcosis also had pulmonary (7%, n = 28/423) or disseminated (4%, n = 15/423) cryptococcosis, and a negligible portion had both (<1%, n = 3/423).
The majority of cases of CNS (70%) and disseminated (73%) cryptococcosis occurred in PWH (Figure 1). Among PWH, CNS, disseminated, and pulmonary cryptococcosis were the most common types (71%, n = 297/420; 14%, n = 57/420; and 6%, n = 27/420; respectively). NHNT patients accounted for 66% (n = 67/101) of all cases of pulmonary cryptococcosis. In addition, 46% (n = 114/250) of cases in the NHNT group were CNS cryptococcosis. By contrast, few cases of cryptococcosis were diagnosed in transplant recipients. CNS and pulmonary cryptococcosis comprised 36% (n = 12/33) and 21% (n = 7/33) of cases in transplant recipients, respectively, while 39% were categorized as unspecified or other forms of cryptococcosis. The median time from transplantation to the diagnosis of cryptococcosis was 6 months (Q1–Q3 0–9 months; range 0–35 months).
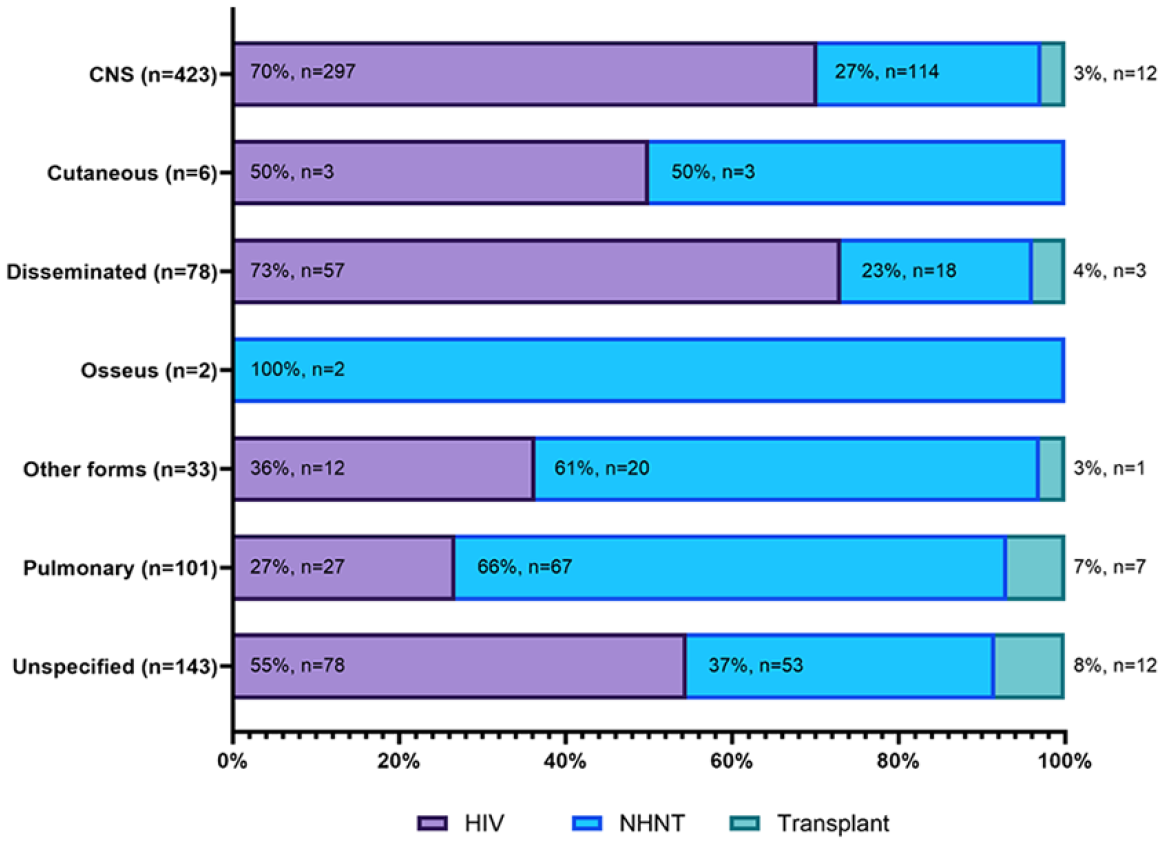
Types of cryptococcosis among people with HIV, NHNT patients, and transplant patients.
The incidence of cryptococcosis varied across groups during the study period (p = 0.03) (Figure 2). While PWH consistently represented a majority of cases, their proportion fluctuated between 52% and 64% from June 2017 to June 2019 before dropping to 47% in the latter half of the study period (July–December 2019). Notably, the incidence of PWH remained relatively stable throughout. Conversely, a slight increase was observed among NHNT and transplant patients during the same timeframe, reaching 45% and 8%, respectively.

Distribution of cryptococcosis among people with HIV, NHNT patients, and transplant patients.
Location of the initial diagnosis among all patients
The index diagnosis was predominantly made in the outpatient setting rather than the inpatient setting (58%, n = 408 versus 42%, n = 295, respectively, p = 0.008). A higher percentage of transplant recipients (79%, n = 26/33) were diagnosed in the outpatient setting compared to PWH (56%, n = 237/420, p = 0.016) and NHNT patients (58%, n = 145/250, p = 0.023).
The overall rate of cryptococcosis-related hospitalization among those initially diagnosed in the outpatient setting was 18%. This rate was highest among transplant patients (31%, n = 8/26), followed by PWH (18%, n = 42/236) and NHNT patients (16%, n = 23/145).
Characteristics of hospitalized patients with cryptococcosis
Among the 369 patients requiring hospitalization, 61% (n = 226) were PWH, 35% (n = 128) were NHNT patients, and 4% (n = 15) had a history of transplant (Table 1). The median age of PWH was significantly lower than that of patients in the NHNT and transplant groups [43 years (Q1–Q3 33–50) versus 52 (38.5–62) versus 57 (46–67), respectively]. Male patients comprised 74% of the PWH and 63% of the NHNT groups but only 47% of those with a history of transplant. In addition, Black individuals represented 65% of the PWH group, while White individuals comprised 58% and 53% of the NHNT and transplant groups, respectively.
Baseline characteristics among hospitalized people with HIV, non-HIV-infected and non-transplant patients, and transplant patients with cryptococcosis.

Data are presented as n (%) unless otherwise noted.
HMO, health maintenance organization; NHNT, non-HIV-infected and non-transplant; Q1, first quartile; Q3, third quartile.
Comorbidities were relatively uncommon among PWH. However, chronic lower respiratory disease (19%), malignancy (16%), and DM (12%) were the most prevalent. Notably, 16% (n = 36/226) of PWH requiring hospitalization had already been receiving ART before the index date. Similarly, among NHNT patients, chronic lower respiratory disease (30%), DM (31%), and malignancy (24%) were the most common comorbidities. In addition, among patients with a history of transplant, 73% had CKD, 60% had DM, and 33% had either malignancy or chronic lower respiratory disease.
Among all hospitalized patients with cryptococcosis over the 3-year study period, 66% (n = 244/369) had ICD-10-CM diagnosis codes for CNS involvement, 16% (n = 60/369) had disseminated cryptococcosis, and 14% (n = 51/369) had pulmonary cryptococcosis. Cutaneous and osseous cryptococcosis were rare, with less than 1% observed for each (n = 3/369 and n = 2/369, respectively). An additional 19% (n = 70/369) and 4% (n = 15/369) were classified as unspecified or other types, respectively. The majority of cases of disseminated (70%) and CNS (67%) cryptococcosis occurred in PWH (Supplemental Figure S1). Among PWH, CNS cryptococcosis was most common (73%, n = 297/420) followed by disseminated (19%, n = 42/226). NHNT patients accounted for 61% (n = 31/51) of all cases of pulmonary cryptococcosis. In addition, 59% (n = 75/128) of cases in the NHNT group were CNS cryptococcosis. By contrast, few cases of cryptococcosis were diagnosed in transplant recipients. CNS and pulmonary cryptococcosis comprised 33% (n = 5/15) and 20% (n = 3/15) of cases in transplant recipients, respectively.
The median duration of hospitalization did not significantly differ between PWH [13 days (Q1–Q3 5–18)], NHNT patients [10 days (Q1–Q3 5–17.5)], and transplant recipients [6 days (Q1–Q3 3–25)] (p = 0.568) (Table 2). In patients with CNS cryptococcosis, PWH had a median duration of hospitalization of 14 days, which was longer but not significantly different than NHNT patients (12 days) and transplant recipients (4.5 days) (p = 0.271). Alternatively, for disseminated cryptococcosis, PWH experienced the shortest hospitalization (12 days) compared to NHNT patients (18 days) and transplant patients (23 days), though no significant difference was observed (p = 0.120). Notably, the median duration of hospitalization for pulmonary cryptococcosis was significantly longer for PWH (15 days) compared to NHNT patients (6 days) and transplant recipients (4 days) (p = 0.002).
Clinical characteristics and outcomes among hospitalized people with HIV, non-HIV-infected and non-transplant patients, and transplant patients with cryptococcosis.

Data are presented as n (%) unless otherwise noted.
Procedures included a composite of diagnostic lumbar punctures, therapeutic lumbar punctures, and ventriculostomy or external VD.
CC, critical care; CNS, central nervous system; ID, infectious diseases; LP, lumbar puncture; NHNT, non-HIV-infected and non-transplant; Q1, first quartile; Q3, third quartile; VD, ventricular drain.
Among all hospitalized patients, 41% (n = 152/369) were assessed by ID providers and 7% (n = 27/369) by critical care providers. PWH (46%, n = 105/226) were more frequently seen by ID providers than NHNT patients (34%, n = 43/128, p = 0.025) and patients with a history of transplant (27%, n = 4/15, p = 0.221).
Clinical manifestations of cryptococcosis in hospitalized patients
Among hospitalized patients with CNS cryptococcosis, altered mental status was documented in 27% of PWH, 40% of NHNT patients, and 40% of patients with a history of transplant, with no significant differences between the groups (p = 0.116) (Table 3). Conversely, cerebral edema was documented more often in NHNT patients (21%) and transplant patients (20%) than in PWH (10%) (p = 0.04). Meningismus, meningoencephalitis, and papilledema were rarely documented, with no differences observed between the groups.
Clinical manifestations among hospitalized people with HIV, non-HIV-infected and non-transplant patients, and transplant patients stratified by the central nervous system, disseminated, and pulmonary cryptococcosis.

Data are presented as n (%) unless otherwise noted.
CNS, central nervous system; NHNT, non-HIV-infected and non-transplant.
Cough and headache were the most frequently documented symptoms across all groups in patients with disseminated cryptococcosis. Fever was documented in 29% of PWH and 20% of NHNT patients but not in individuals with a history of transplant. Notably, altered mental status was more common in NHNT patients (40%) and transplant recipients (67%) compared to PWH (16%). However, there were no statistically significant differences in any of the assessed symptoms between the groups.
Cough was the most frequently documented symptom across all groups in patients with pulmonary cryptococcosis. Chest pain and fever were noted in varying percentages in PWH and NHNT patients but were absent in those with a history of transplant. Likewise, altered mental status and headache were documented in PWH and NHNT patients but not observed in the transplant group. Interestingly, hypoxemia was uncommon, documented in 6% of PWH and 10% of NHNT patients, but in none of the individuals with a history of transplant. Consistent with the findings for CNS and disseminated cryptococcosis, there were no statistically significant differences in any of the assessed symptoms across the groups.
LPs and VDs in hospitalized patients
163 LPs or VDs were documented as performed in 162 hospitalized patients, with 98% (n = 159/163) being diagnostic LPs and 2% (n = 4/163) being therapeutic LPs. A higher proportion of PWH (52%, n = 117/226) underwent LP compared to NHNT patients (32%, n = 41/128, p = 0.0004), and patients with a history of transplant (27%, n = 4/15, p = 0.07) (Table 2). However, the median number was similar for PWH [1 (Q1–Q3 0–1)], NHNT patients [1 (Q1–Q3 0–1)], and transplant recipients [0 (Q1–Q3 0–1)] (p = 0.875).
Of all documented LPs, 78% (n = 127/163) were performed in patients with CNS cryptococcosis. However, only 52% (n = 127/244) of all patients with CNS cryptococcosis underwent LP, which was more common among PWH (58%, n = 95/164) compared to NHNT patients (41%, n = 31/75) and those with a history of transplant (20%, n = 1/5). Notably, no hospitalized patient with CNS cryptococcosis underwent ventriculostomy or external VD placement.
Outcomes among hospitalized patients
The Elixhauser Comorbidity Index indicated a higher risk of 30-day all-cause readmission for PWH compared to NHNT (p = 0.001) (Table 2). However, the risk of 30-day all-cause readmission did not significantly differ between PWH and transplant patients (p = 0.092). Conversely, the Elixhauser Comorbidity Index risk of in-hospital mortality was lowest among PWH indicating a lower likelihood for in-hospital death versus NHNT patients (p < 0.001) and those with a history of transplant (p = 0.018).
The overall in-hospital mortality rate within 90 days and 1-year after the index date was 12% (n = 43/369) and 13% (n = 48/369), respectively. At 90 days, the mortality rate was significantly higher in NHNT patients (22%, n = 28/128) compared to PWH (7%, n = 15/226) and transplant recipients (0%) (p < 0.001) (Table 2 and Supplemental Table S9). One-year in-hospital mortality was lowest among PWH (8%, n = 18/226) compared to NHNT patients (22%, n = 28/128, p = 0.0004) and transplant recipients (13%, n = 2/15, p = 0.359). Mortality rates were similar between PWH who received ART before being diagnosed with cryptococcosis versus those who did not (6%, n = 2/36 versus 8%, n = 16/190, p = 0.745).
The 90-day and 1-year all-cause in-hospital mortality rates were 8% (n = 31/369) and 10% (n = 36/369) for individuals with CNS cryptococcosis, 1.4% (n = 5/369) and 1.6% (n = 6/369) for disseminated cryptococcosis, and less than 1% (n = 3/369 for both) for pulmonary cryptococcosis. LPs performed on patients with CNS cryptococcosis were not associated with decreased 1-year mortality rates overall (12%, n = 15/127 versus 18%, n = 21/117, p = 0.207) or across groups. PWH with CNS cryptococcosis had lower 90-day (6%, n = 13/226) and 1-year (7%, n = 16/226) in-hospital mortality compared to NHNT patients with CNS cryptococcosis (14%, n = 18/128 for both). Nearly all PWH who died within 90 days (87%, n = 13/15) and 1 year (89%, n = 16/18) of hospitalization had CNS cryptococcosis. Similarly, among NHNT patients who died at both 90-day and 1 year, 64% (n = 18/28) had CNS cryptococcosis. The 90-day and 1-year in-hospital mortality rates for disseminated cryptococcosis and pulmonary cryptococcosis among NHNT patients were 3% (n = 4/128) and 2% (n = 3/128), respectively. Evaluation by an ID provider was not associated with a significant difference in mortality rates at either 90 days (p = 0.212) or 1 year (p = 0.126) across patient groups or types of cryptococcosis (Supplemental Table S9).
Logistic regression analysis demonstrated significantly higher odds of 90-day in-hospital mortality among NHNT patients compared to PWH (odds ratio 3.91, 95% confidence interval 2.03–7.52, p < 0.0001) (Supplemental Table S10).
Discussion
Our analysis has uncovered significant trends in the epidemiology and outcomes of cryptococcosis across the United States as new risk factors for this infection continue to be identified. Historically, PWH accounted for the majority of cases, but in recent years, this proportion has significantly decreased due to the expansion of ART and a reduced prevalence of advanced HIV. 2 Alternatively, cases have emerged in people without HIV, driven by higher rates of comorbidities, organ transplants, malignancies, and increased use of immunosuppressive therapies,28 –31 consistent with our findings. A multicenter study conducted in Australia and New Zealand between 2015 and 2019 revealed that 39% of the 475 cases of cryptococcosis lacked an underlying immunodeficiency. 14 However, 56% (n = 35/62) of these patients had at least one underlying comorbidity, such as chronic lung disease, liver disease, kidney disease, or DM, which may have increased their susceptibility to cryptococcosis. Conversely, 24% of NHNT patients in our study did not have any comorbidity associated with immune dysfunction.
While the overall distribution of cases among PWH, NHNT, and transplant patients in our study was similar to other reports from the United States,7,21 we observed several noteworthy differences. Previous studies performed in the United States were often limited to specific regions 21 or single institutions,7,32 and many did not provide details on NHNT and transplant patients. 33 Our cohort, which was more recent and utilized data for Medicaid enrollees from geographically dispersed states across the United States from 2017 to 2019, provided a broader perspective of cryptococcosis.7,21,33 In addition, the Merative Medicaid Database (formerly IBM® MarketScan® Medicaid Database) allowed for analysis of services from both inpatient and outpatient settings, whereby 58% of cases in our study were first diagnosed in the outpatient setting, but 52% of all patients required hospitalization. In the hospitalized cohort, the majority were PWH, followed by NHNT patients and those with a history of transplant, consistent with findings from comparable studies involving hospitalized patients with cryptococcosis.21,33
Demographic characteristics and clinical manifestations of cryptococcosis also varied among groups overall and among hospitalized patients. As observed in other reports,21,32 CNS and disseminated cryptococcosis occurred more frequently in younger Black male PWH compared to individuals without HIV. Less than 30% of PWH were receiving ART within the 3 months prior to the index date, and laboratory data were unavailable to assess virological and immunological control. Conversely, the burden of comorbidities was lower among PWH.
PWH were more likely to be diagnosed with cryptococcosis during hospitalization compared to NHNT and transplant patients. This difference suggests potential shortcomings in cryptococcal antigen screening and early detection methods among PWH. Existing data reveal low screening rates among asymptomatic PWH with poorly controlled HIV. 34 Challenges with engagement in preventive care and appointments among PWH 35 could lead to missed opportunities for early symptom identification, potentially resulting in delayed diagnosis and hospitalization. In addition, the higher frequency of ID evaluation during hospitalization for PWH might also contribute to their higher inpatient diagnosis rate, possibly reflecting heightened clinician vigilance for opportunistic infections in immunocompromised patients.
Despite the importance of LPs for diagnosing and managing CNS cryptococcosis,1,36 only half (52%) of hospitalized patients with CNS cryptococcosis in our study had evidence of undergoing a diagnostic LP based on CPT coding. Procedures to manage intracranial pressure were also uncommonly documented in this group. While previous research based on manual chart review identified deviations from guideline recommendations for managing intracranial pressure, 37 the low rate of LPs in our study may be attributed to factors such as lack of familiarity with the procedure or the perceived complexity of performing serial LPs. However, it is more likely due to issues related to billing and coding procedures, given the number of cases of CNS cryptococcosis without diagnostic LPs. This underutilization of LPs is concerning, potentially impacting diagnosis, treatment, and patient outcomes. Further investigation is needed to confirm the role of billing and coding in this discrepancy.
Recent research from Australia and New Zealand has questioned the necessity of routine LPs in individuals without HIV, suggesting that a combination of a high serum cryptococcal antigen titer and the presence of fungemia may predict the risk of asymptomatic cryptococcal meningoencephalitis, potentially reducing the need for LPs. 14 Further investigations are necessary to validate the use of these biomarkers in LP decision-making. Therefore, there is a need for continued education regarding the importance of managing intracranial pressure in PWH displaying signs and symptoms associated with CNS involvement.
Our study did not identify a significant association between evaluation by an ID provider and reduced mortality at 90 days or 1 year, regardless of patient group or type of cryptococcosis. However, it is important to consider limitations in interpreting this result. First, only 41% of hospitalized patients received an ID consult. This limited sample size might have masked a potential benefit, particularly for specific patient groups. Second, patients with cryptococcosis can present with a wide range of clinical manifestations and complications, and factors such as timeliness of diagnosis, selection of appropriate antifungal medications, management of intracranial pressure, and control of underlying comorbidities significantly influence mortality. Previous research supports a potential role for ID consultation in improving outcomes. A retrospective review reported significantly lower 90-day mortality among 147 individuals without HIV with cryptococcosis who received ID consultation (27% versus 45%, p < 0.001). However, it is important to note that these patients were also more likely to have CNS involvement and a higher fungal burden, 38 both of which are associated with worse outcomes. 39 The improved survival observed in this study is likely attributable to the increased utilization of procedures to manage intracranial pressure and combination antifungal therapy. 39 Furthermore, ID consultation can potentially reduce diagnostic delays. Studies have identified cognitive errors and knowledge deficits as contributing factors to delayed diagnoses in patients with cryptococcosis.34,40 Earlier recognition through ID consultation might lead to greater adherence to guideline-directed management and improved outcomes for patients with cryptococcosis. 37 Our study design may have limited our ability to detect an association between ID evaluation and mortality. Future studies with larger cohorts and a higher proportion of ID consultations are needed to definitively assess the impact of ID involvement on outcomes in patients with cryptococcosis. In addition, investigating the specific interventions implemented by ID providers and their influence on outcomes would provide valuable insights for optimizing patient management.
Most NHNT patients with cryptococcosis identified as White individuals and had a heterogeneous list of comorbidities, consistent with other reports. 8 In our study, NHNT patients had low rates of traditional risk factors for cryptococcosis (e.g. immunodeficiencies, hepatic fibrosis, and cirrhosis), emphasizing the fact that cryptococcosis can affect apparently immunocompetent patients.7,8,17 Chronic lower respiratory diseases were most common among NHNT patients potentially contributing to the high proportion of pulmonary cryptococcosis in these patients, though we did not examine history of glucocorticoid or immunosuppressive therapy. 41 However, cough, chest pain, or hypoxemia was documented in less than one-third of NHNT patients with pulmonary cryptococcosis. This observation underscores the likelihood of asymptomatic pulmonary cryptococcosis and suggests that many of these patients may experience no symptoms. 41 The significantly higher prevalence of cerebral edema documented in NHNT patients compared to PWH and transplant recipients is an intriguing finding. While the underlying mechanism is unclear, it could be related to differences in host inflammatory responses or the presence of a cerebral cryptococcoma. 42 Similar to our findings, signs and symptoms associated with meningoencephalitis were present in only 20% of NHNT patients with cryptococcosis involving the CNS, 43 despite previous reports of high rates of CNS cryptococcosis in individuals without HIV. 8 This highlights the heterogeneity in presentation among NHNT patients with CNS cryptococcosis. The absence of specific symptoms along with fewer comorbidities associated with cryptococcosis leads to delayed diagnosis and worse outcomes in NHNT patients.17,43 Despite the availability of highly accurate diagnostic tests, delays persist, resulting in significantly higher morbidity and mortality. Early recognition is crucial but challenging due to the changing epidemiology of cryptococcosis and the increase in non-traditional patient populations.
As in other reports,21,32 comorbidities were most common in patients with a history of solid organ transplantation, who were older and less likely to be male than PWH or NHNT patients. Cryptococcosis is uncommon following organ transplantation and presents as a late infection, 30 likely contributing to the limited number of cases in our study. The time from transplantation to the diagnosis of cryptococcosis in our study (176 days) was shorter than those observed in previous studies (464 30 and 575 days 44 ). In addition, patients with a history of transplantation accounted for the highest proportion of cases diagnosed in the outpatient setting, the highest rate of subsequent hospitalization, but the fewest signs and symptoms, which might reflect frequent outpatient follow-up or previously missed opportunities to diagnose cryptococcosis in the inpatient setting. 17
In-hospital mortality at 90 days and 1 year were 12% and 13%, respectively, among all patients in our study, comparable to other hospitalized cohorts.33,45 However, these findings differ from the higher mortality rates reported in other studies (16–31%).7,17,21,30,32 These discordant findings may be due to improved management of cryptococcosis in our study timeframe compared to historical cohorts, but most likely represent lower rates of comorbidities associated with poor outcomes, as well as lack of follow-up beyond 1 year for our cohort. 7
Our study adds to the growing body of evidence, highlighting the significantly higher mortality rates associated with NHNTs compared to PWH and transplant recipients.9,18 At both 90 days and 1 year, mortality rates were significantly higher in the NHNT group (22% at both time points) compared to PWH (7% and 8%) and transplant recipients (0% and 13%). The majority of deaths within 90 days and 1 year were attributed to CNS cryptococcosis, particularly in PWH and NHNT patients. The unexpected increase in mortality rates among NHNT patients was likely influenced by diagnostic delays, evidenced by limited reported symptoms and a high proportion diagnosed in the outpatient setting. This underscores the dynamic nature of cryptococcosis outcomes. However, the limited information on mortality rates of cryptococcosis in NHNT patients underscores the need for further investigations to elucidate the unique challenges associated with cryptococcosis in this subgroup.
The Merative Medicaid Database (formerly IBM® MarketScan® Medicaid Database) allowed us to describe the epidemiology and outcomes of cryptococcosis across the United States with a more recent cohort, but our study was retrospective and required continuous health plan enrollment during the 6 months prior to the index date. The study period was also limited due to the institutional user agreement, although it avoided potential confounding with cases occurring in patients with COVID-19. The database includes data for Medicaid enrollees from geographically dispersed states but does not provide geographic variables, which may limit the generalizability of our findings. Comorbidities, signs and symptoms, procedures, and diagnosis of cryptococcosis were identified using administrative codes. These codes can be susceptible to under-coding and misclassification, particularly for less common infections and not adequately capture the nuanced impact of transplantation on comorbidity reporting. Although we incorporated immunosuppressive conditions, the use of immunosuppressive medications was not captured, as the data were unavailable in the inpatient setting, potentially resulting in an underestimation of the prevalence of immunosuppression within our study population. In addition, clinical manifestations suggestive of cryptococcosis were captured, but the specific timing and sequencing could not be determined. Serologic and microbiologic testing results to support the cryptococcosis diagnosis were unavailable. While one study demonstrated promising positive predictive values for using diagnosis codes to identify cryptococcosis, its analysis was limited to just five patients with CNS cryptococcosis. 46 Another study cited unpublished work and reported a positive predictive value of 87% using diagnosis codes from 122 cases of cryptococcosis, but details remain unavailable due to reliance on personal communication. 21 These limited evaluations highlight the need for broader evaluation to assess their effectiveness and potential influence on conclusions drawn from these codes. We assessed subgroups based on types of cryptococcosis due to the greater specificity of ICD-10-CM diagnosis codes compared to previous iterations but were unable to differentiate between Cryptococcus species, which are associated with variable presentations and outcomes. Furthermore, data on antifungal medications administered during hospitalization was unavailable from the database.19,20 This lack of information limited our ability to assess the potential impact of antifungal therapy on patient outcomes. Lastly, outcomes data were only available for hospitalized patients during their admission.
Conclusion
The epidemiology of cryptococcosis in the United States continues to evolve, with decreasing incidence among PWH and increasing incidence among those with inflammatory, autoimmune, and neoplastic comorbidities. The rise in cryptococcosis is associated with aggressive immunosuppressive and biological therapies used to prevent transplant-related rejection and to treat malignancies and inflammatory and autoimmune diseases. Unfortunately, patients without HIV, many of whom lacked traditional risk factors for cryptococcosis, had higher mortality compared to PWH. Therefore, clinicians must be aware of the epidemiologic transition of underlying immunosuppressive conditions predisposing patients to develop cryptococcal infection to improve early detection, recognition, and treatment.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241244967 – Supplemental material for Epidemiological trends and clinical outcomes of cryptococcosis in a medically insured population in the United States: a claims-based analysis from 2017 to 2019
Supplemental material, sj-docx-1-tai-10.1177_20499361241244967 for Epidemiological trends and clinical outcomes of cryptococcosis in a medically insured population in the United States: a claims-based analysis from 2017 to 2019 by Daniel B. Chastain, Qian Zhang, Xianyan Chen, Henry N. Young, Carlos Franco-Paredes, Jose Tuells, George R. Thompson and Andrés F. Henao-Martínez in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-2-tai-10.1177_20499361241244967 – Supplemental material for Epidemiological trends and clinical outcomes of cryptococcosis in a medically insured population in the United States: a claims-based analysis from 2017 to 2019
Supplemental material, sj-docx-2-tai-10.1177_20499361241244967 for Epidemiological trends and clinical outcomes of cryptococcosis in a medically insured population in the United States: a claims-based analysis from 2017 to 2019 by Daniel B. Chastain, Qian Zhang, Xianyan Chen, Henry N. Young, Carlos Franco-Paredes, Jose Tuells, George R. Thompson and Andrés F. Henao-Martínez in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.