
Abstract
Objective
To analyse the clinicopathological features of isolated pulmonary cryptococcosis in human immunodeficiency virus (HIV)-negative patients.
Methods
This retrospective study analysed the following data from HIV-negative patients diagnosed with pulmonary cryptococcosis: demographics, underlying diseases, clinical manifestations on admission, laboratory tests, imaging data, results of histopathology, treatment options and outcomes. Sputum samples from all patients were collected and assessed for the presence of yeast or fungi. Cryptococcal antigen testing was performed for some patients. Histopathological analysis was also undertaken for some samples of lung tissue.
Results
The study analysed 37 patients (22 males). Thirteen (35.14%) patients were asymptomatic, 24 (64.86%) were symptomatic and 17 (45.95%) patients had no underlying disease. Out of 25 tested patients, 23 (92.00%) tested positive on the serum cryptococcal capsular polysaccharide antigen test. During 6 to 24 months of follow-up, all 37 patients that were either treated with or without antifungal therapy alone or combined with surgical resection showed complete recovery. One patient made a full recovery without any treatment.
Conclusion
Early identification of pulmonary cryptococcosis in HIV-negative patients and timely detection of cryptococcal antigens in serum or respiratory specimens may help to improve diagnosis, prognosis and treatment of the disease.
Keywords
Introduction
Cryptococcus is a ubiquitous pathogen widely distributed throughout the world, especially in soil and bird habitats. There are more than 70 species. In China, Cryptococcus ranks third after Aspergillus and Candida in all invasive fungal diseases. 1 It has high affinity for the central nervous system and thus easily causes cryptococcal meningoencephalitis. Approximately 1 million people worldwide suffer from cryptococcal meningitis each year and more than 60% of these patients die from the disease. 2 The majority of cryptococcosis cases are caused by Cryptococcus neoformans or Cryptococcus gattii. 3 The former has a worldwide distribution infecting both immunocompetent and immunosuppressed hosts, while the latter is more prevalent in tropical and subtropical regions infecting mostly immunocompetent hosts.4,5 Cryptococcus can also infect individuals without any underlying disease. A good example is pulmonary cryptococcosis (PC) that is often caused by inhalation of cryptococcal spores from the air. It is localized in the lungs and has nonspecific symptoms such as cough, dyspnoea, chest pain and fever. It may be totally asymptomatic or may present as acute respiratory distress syndrome (ARDS). 6
In recent years, the incidence of PC has risen rapidly. 7 Of note, its incidence has increased by more than six-times between year 1999 and 2006 reaching 38 cases in every million people. 7 Most of these increased cases were in human immunodeficiency virus (HIV)-negative patients. 7 To date, PC in HIV-negative patients is not as well understood as in HIV-positive patients. There are also existing controversies regarding the optimal treatment for PC in immunocompetent hosts with mild symptoms. 8 Moreover, because of its nonspecific symptoms, the misdiagnosis rate is high in China and hence it is not treated promptly resulting in increased mortality. 9 In order to improve the understanding of PC in HIV-negative patients, this current study retrospectively analysed the clinical data from patients diagnosed with PC between 2014 and 2018. This study also reviewed the relevant literature to improve the management of the disease.
Patients and methods
Patient population
This retrospective study analysed the clinical data from consecutive HIV-negative patients diagnosed with PC at Dongyang Hospital Affiliated to Wenzhou Medical University, Dongyang, Zhejiang Province, China between May 2014 and May 2018 using a computer-assisted search of the hospital’s electronic medical records. Patients were classified as having proven PC based on the following criteria: histopathological, cytopathological or direct microscopic examination of a specimen obtained by a needle aspiration or biopsy from a normally sterile site (other than mucous membranes) showing encapsulated budding yeasts; or probable PC if each of the three elements of host factor, clinical features and mycological evidence were present. 10 Those patients with HIV infection, disseminated cryptococcosis or PC with possible diagnosis were excluded from this study.
Informed consent was waived because this was a retrospective study and there was no modification in the patient management. All personal information was encrypted in the database and patient data were anonymized. There was no breach of privacy. This retrospective study was approved by the Ethics Committee of Dongyang Hospital Affiliated to Wenzhou Medical University (no. 2019-YX-067).
Clinical data collection
The following data were recorded for all patients: demographic, underlying diseases, clinical manifestations on admission, laboratory tests, imaging data, results of histopathology, treatment options, treatment and outcomes. Sputum samples from all patients were collected and cultured in appropriate media for yeast and fungal growth. The cultures were later visualized under an electronic microscope to assess whether there were any yeast or fungi present. In those patients that underwent cryptococcal capsular polysaccharide antigen (CrAg) lateral flow assay (LFA) testing (IMMY Inc. Norman, OK, USA), the results were also recorded. Lung tissue samples obtained from patients were stained with haematoxylin and eosin (H&E). Histochemical staining was performed with periodate Schiff, mucus cardin and Grocott’s dimethylamine silver. All patients underwent a chest computed tomography (CT) scan and the findings were interpreted by two experienced radiologists. The follow-up of patients was undertaken during regular clinic visits and by telephone contact.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. All values are expressed as mean ± SD or n of patients (%). No statistical comparisons were undertaken.
Results
A total of 37 HIV-negative patients with proven or probable PC were enrolled in the study. Of these, 22 patients were males and 15 were females. The flowchart for the selection of the study population is shown in Figure 1. The demographic and clinical characteristics of the study cohort are presented in Table 1. The mean ± SD age was 51.95 ± 11.65 years (range, 27–83 years).

Flowchart of the study population with pulmonary cryptococcosis (PC) and data from positive and negative cases for different diagnostic methods. CrAg, cryptococcal capsular polysaccharide antigen; BALF, bronchoalveolar lavage fluid.
Demographic and clinical characteristics of human immunodeficiency virus-negative patients with pulmonary cryptococcosis (n =37).

Data presented as mean ± SD or n of patients (%).
Of the 37 patients, seven were in formal employment, 14 were farmers, 13 were housewives, one was a clinician and two were businessmen. Of the 37 patients, 17 had no underlying disease. Twenty patients had a variety of underlying diseases, with some having two or more of the following underlying diseases: eight had hypertension, five had diabetes mellitus and seven had hepatitis B. Two patients had undergone surgery for malignant tumours, five patients had connective tissue disease and one had leukocytopenia. All 37 patients tested negative for HIV and had normal CD4+ T cell counts. Those with underlying diseases had not been treated with immunosuppressive therapy. In terms of environmental exposure, six patients had been exposed to pigeons and four patients had a history of keeping cats, dogs or poultry.
Thirteen patients (35.14%) were asymptomatic and detection was only made by screening. The other 24 patients (64.86%) were symptomatic exhibiting varying clinical manifestations. The most common clinical manifestations were coughing, expectoration, chest pains and fever (Table 2).
Clinical features of pulmonary cryptococcosis in human immunodeficiency virus-negative patients (n =37).

Data presented as mean ± SD or n of patients (%).
CRP, C-reactive protein; PCT, procalcitonin; CrAg, cryptococcal capsular polysaccharide antigen.
Sputum samples from all 37 patients were negative when cultured and visualized under an electronic microscope to assess whether there were any yeast or fungi present. A total of 25 patients underwent CrAg LFA for the semiquantitative detection of CrAg in serum; and 23 out of the 25 tested positive. Four patients underwent bronchoscopy to identify positive CrAg LFA in bronchoalveolar lavage (BAL). Two of the BAL direct smears were positive for Cryptococcus (Table 2).
To clarify the nature of the lung lesions, 14 patients underwent thoracoscopic surgery while 12 patients were diagnosed by CT-guided lung biopsy. Two patients were diagnosed according to a positive result from the BAL direct smears for Cryptococcus and the remaining nine patients were clinically diagnosed with pulmonary cryptococcosis. All lung tissues obtained from 26 patients were stained with haematoxylin and eosin and the histopathology showed cryptococcal granuloma in 25 patients.
All patients underwent chest CT scans. The radiological appearance of pulmonary cryptococcosis mimicked that of other clinical conditions such as tuberculosis, malignancy, bacterial pneumonia and infarction (Figure 2). Nodules or masses located in the lower lobe and peripheral area of the lung were observed in most patients. The radiological manifestations of all patients are shown in Table 3.

Representative chest computed tomography (CT) images of pulmonary cryptococcosis mimicking lung cancer. (a) A 69-year-old Asian woman with a history of rheumatoid arthritis was admitted to hospital with complaints of cough and sputum for 3 months and fever for 4 days. The chest CT scan revealed diffuse nodules in both lungs. (b) After 4 months of 400 mg fluconazole orally once daily treatment, a re-examination of the chest CT showed that multiple nodules were clearly absorbed.
Radiography findings of pulmonary cryptococcosis in human immunodeficiency virus-negative patients (n =37).
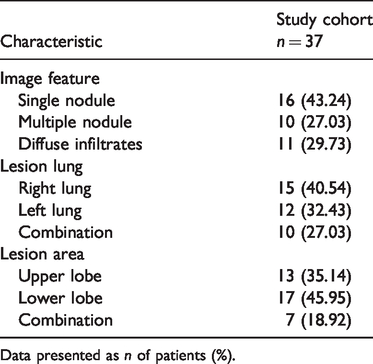
Data presented as n of patients (%).
A total of 28 patients were directly diagnosed and confirmed to have pulmonary cryptococcosis: 26 were confirmed by histopathology while confirmation of the other two was done by direct microscopy of BAL (Table 4). The diagnosis of the remaining nine patients was indirect and could not be confirmed prior to some preliminary tests. They underwent antifungal treatment first, after which the symptoms showed more prominently in the radiological imaging results. This confirmed the presence of pulmonary cryptococcosis. The time from presentation to final diagnosis of pulmonary cryptococcosis ranged from 5 to 17 days. On admission to hospital, 35 patients (94.59%) had initially been misdiagnosed: 16 patients (43.24%) were thought to have pneumonia, two patients (5.41%) were thought to have tuberculosis and 17 patients (45.95%) were thought to have lung cancer. Only two patients (5.41%) had been correctly diagnosed as having pulmonary cryptococcosis.
Diagnosis and treatment of pulmonary cryptococcosis in human immunodeficiency virus-negative patients (n =37).

Data presented as n of patients (%).
PCNB, computed tomography-guided percutaneous cutting needle biopsy; CrAg, cryptococcal capsular polysaccharide antigen; BAL, bronchoalveolar lavage.
Several treatment options were undertaken (Table 4). One patient experienced spontaneous recovery within 6 months of follow-up without any antifungal treatment or surgery (Figure 3); 22 patients received antifungal therapy and 14 patients underwent surgical resection. Among the 14 patients that underwent surgical resection, 13 were treated with postoperative antifungal medication while one patient only underwent surgical resection without postoperative antifungal medication. Antifungal therapy was undertaken using 400 mg fluconazole orally once a day as recommended by guidelines. 11 During 6 to 24 months follow-up, all 37 patients had good outcomes after treatment. However, one patient had a relapse of the lesions 8 months after antifungal therapy with 400 mg fluconazole orally once a day for 9 months. The patient underwent another regime of antifungal treatment with 200 mg voriconazole orally twice a day for 12 months after which the lesions were completely absorbed. There was also no recurrence after follow-up at 12 months.

Representative chest computed tomography (CT) images of a case of pulmonary cryptococcosis that did not require antifungal therapy. (a) A 55-year-old Asian male with concomitant diabetes mellitus. He was admitted to hospital with complaints of cough and sputum for 2 weeks. A chest CT scan revealed consolidation of the right lower lobe. (b) The chest CT scan showed complete absorption without any antifungal treatment after 6 months of follow-up.
Discussion
Over the last several decades modern medical interventions such as the use of immunosuppressive drugs have raised concerns over the rise in invasive fungal infections caused by Cryptococcus. 12 Cryptococcosis is the third most common invasive fungal infection, 1 and PC mostly manifests itself in immunocompetent patients, 13 with 35% of these cases occurring in HIV-negative patients. 14 Birds play an important role in the epidemiology and spread of PC. 5 According to research, cryptococcal spores can survive in the stomach of pigeons for 86 days. 5 The woody environments that birds live in are conducive to the growth of Cryptococcus because of enabling factors such as the presence of tree holes, flowering plants and bird droppings.15–17 In this current retrospective study, six patients were working or living in environments potentially contaminated by fungal spores. As such, it is evident that identification of infested areas, proper control of birds and disinfection of contaminated environments is essential for the epidemiological control of cryptococcosis.
In this current retrospective study, males were prone to infection than females. These current results were consistent with previously published findings.18,19 Approximately one-third of immunocompetent patients diagnosed with PC in the current study were asymptomatic. In contrast, more than half of the remaining two-thirds of symptomatic patients had only cough or chest pain as their symptoms. Nodules located in the peripheral area of the lung were the most common imaging finding on chest X-rays and chest CT scans of immunocompetent patients diagnosed with PC. 20 Further to this, lesions are usually located in a unilateral lung lobe, especially on the right side. 21 Because of these atypical symptoms and imaging findings that are not specific to PC, misdiagnosis and missed diagnosis are often common. In this current study, only two patients were correctly diagnosed at hospital admission.
The correct diagnosis of PC requires histopathology tests or the culture of respiratory specimens to obtain positive results. Direct microscopic examination can also detect Cryptococcus in some cases. However, these methods are limited; histopathology is an invasive procedure while culturing and direct microscopy are time-consuming and laborious. 22 The CrAg LFA test has therefore been widely used to detect cryptococcal antigens because of its high sensitivity and specificity. 3 However, it has not been standardized for respiratory specimens such as BAL, pleural fluid and sputum. For example, a previous study in 23 HIV-negative patients with pulmonary cryptococcosis showed that the positive rate of CrAg in BAL was 82.6% while that of serum CrAg was 73.9%. 23 In this current study, four patients had positive cryptococcal antigens in BAL. Based on these results, detection of cryptococcal antigen in BAL can be used as a supplementary diagnostic tool. However, further research is needed with large sample sizes.
Although PC can occur in people without underlying diseases, those with underlying diseases or a defective immune system are more predisposed to the disease. For example, well-known predisposing factors are: HIV infection, solid organ transplantation, long-term corticosteroid or immunosuppressive therapy, malignancy, severe diabetes mellitus leading to organ damage and cirrhosis. 13 In China, hepatitis B affects many people, most of whom develop cirrhosis. 24 Because of their impaired cellular and humoral immunity, patients with cirrhosis cannot quickly remove cryptococcal spores once they have inhaled them and thus they are easily infected. 25 As such, cirrhosis was reported as a risk factor for cryptococcosis. 26 In HIV-negative patients, 21–36% of Cryptococcus infections occur in patients with cirrhosis. 27 In addition, cryptococcocaemia occurs in 50–70% of patients with cirrhosis-related cryptococcosis. 27 The mortality rate of cirrhotic patients caused by cryptococcocaemia ranges from 51–100% thus making cirrhosis the most significant predictor of 30-day mortality in patients with cryptococcocemia. 27 In this current study, seven patients had hepatitis B in addition to cryptococcal infection. Based on these observations, in our opinion, clinicians need to be alert to cirrhosis-related cryptococcal disease in their daily work. They should also aim to detect cryptococcal antigens as early as possible in patients with end-stage liver disease and unexplained sepsis.
In this current study, 13 patients were asymptomatic and the treatment of asymptomatic pulmonary cryptococcosis remains controversial. For example, a previous study concluded that immunocompetent hosts with isolated pulmonary cryptococcosis do not require antifungal therapy as most of them can recover without any treatment. 28 Since then, there have been reports of immunocompetent patients with positive sputum culture findings that have done well clinically without any treatment.29,30 In contrast, there are studies that present the contrary view. For example, a study in HIV-negative patients reported that without treatment a small number of immunocompetent hosts with isolated PC progress to cryptococcal meningitis. 31 Fluconazole is the drug of choice for immunocompetent patients diagnosed with PC because it does not affect the central nervous system. 32 A systematic review of the prevalence of fluconazole resistance in Cryptococcus clinical isolates in 29 studies demonstrated that the mean fluconazole resistance was 10.6% for the incident isolates (n = 4747) from HIV-positive patients. 33 The rate of fluconazole resistance has increased over time thus causing considerable challenges in the management of Cryptococcus infections.34,35 In this current study, one immunocompetent patient experienced spontaneous recovery without any antifungal treatment within 6 months of follow-up. Based on this observation, it is our opinion that immunocompetent patients with pulmonary cryptococcosis with minimal symptoms limited to the lungs can be observed without therapy because of the toxicity, cost and risk of drug resistance of antifungal drugs. However, there was no conclusive optimal treatment plan for patients whose lesions had been surgically removed. A previous study reported that patients with normal immune function whose lesions were surgically removed had no recurrence within 1 year of follow-up despite antifungal treatment not being used. 18 These results were consistent with those of this current study in which one immunocompetent patient did not undergo antifungal therapy after surgical resection and no recurrence occurred. However, to prevent intraoperative infection, intraoperative compression should be avoided.
This current study had several limitations. First, it was retrospective in nature and had a small study population. Secondly, not all of the patients were confirmed as having PC using histopathology. Thirdly, the CrAg LFA test was not widely used in our hospital in 2014–2015, so not all patients underwent this test. The collection of patients with PC continues at this institution and a prospective study of isolated PC is ongoing, which may provide answers to some questions in the future.
Pulmonary cryptococcosis commonly appears as clustered nodules in the peripheral area of the lung. Because of its atypical clinical manifestations and radiological appearance, clinicians may fail to make an early diagnosis. Detection of cryptococcal antigens in BAL can be used as an adjunct diagnostic method although further research is needed to ascertain its use. As a country with a high incidence of hepatitis B, clinicians in China need to be alert to the high incidence of cirrhosis patients with PC. Early identification of PC in HIV-negative patients and timely detection of cryptococcal antigens in serum or respiratory specimens may help to improve diagnosis, prognosis and treatment of the disease.
Footnotes
Acknowledgement
We would like to thank the staff at the Records System and Medical Imaging Division of the Dongyang Hospital Affiliated to Wenzhou Medical University for their assistance in collecting data and figures in this study.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.