
Abstract
The resurgence of diphtheria in Nigeria, culminating in an outbreak surpassing previous records, has spotlighted the critical imperative for robust immunization policies amidst a milieu of vaccine hesitancy. This commentary delineates the multifaceted dimensions of the current diphtheria outbreak, which started in May 2022, juxtaposed against historical outbreaks, with a focal examination of the pervasive vaccine hesitancy and its underpinning sociocultural and systemic determinants. The discourse extends to a meticulous evaluation of Nigeria’s public health response, underlined by the synergy with international organizations, reflecting a global collaborative ethos in combating the diphtheria menace. A critical appraisal of the prevailing immunization policies unveils a necessity for strategic amendments to invigorate vaccination uptake, essential for curbing the diphtheria outbreak and enhancing public health resilience. The reflections herein advocate for a comprehensive, culturally resonant, and sustainable public health paradigm, encompassing a synergistic approach of policy fortification, community engagement, and international collaboration to navigate the challenges posed by vaccine-preventable diseases epitomized by the ongoing diphtheria outbreak. Through a synthesis of historical lessons, contemporary challenges, and global solidarity, this piece contributes to the broader discourse on enhancing immunization coverage and infectious disease control in Nigeria.
Plain language summary
Recently, Nigeria has faced its worst diphtheria outbreak in years, showing how important it is to get people vaccinated. This article looks closely at the current outbreak, compares it to past ones, and explores why some people are hesitant to get vaccinated. We discuss the reasons behind this hesitation, including cultural and social factors. We also review how Nigeria is responding to the outbreak with help from international groups. We point out that Nigeria’s vaccination policies need to be updated to encourage more people to get vaccinated, which is crucial to stop the outbreak and strengthen overall health defenses. The article calls for a well-rounded and lasting approach to public health that includes better policies, working closely with communities, and international cooperation.
Introduction
The discourse surrounding infectious disease control has undergone a seminal shift with the emergence and widespread dissemination of vaccines, heralding a transformative epoch in global public health landscapes. 1 However, the potency of vaccines in curtailing the incidence of preventable diseases such as diphtheria has been ostensibly attenuated by the phenomenon of vaccine hesitancy.2,3 The term ‘vaccine hesitancy’ encapsulates a spectrum of attitudes toward vaccination, ranging from slight reluctance to absolute refusal, despite the availability of vaccination services.2,3 This phenomenon is not peculiar to Nigeria but has shown to have grave implications in the face of burgeoning infectious disease outbreaks. The World Health Organization (WHO) flagged vaccine hesitancy as one of the top 10 threats to global health, 4 emphasizing its potential to reverse the progress made in combating vaccine-preventable diseases.
In Nigeria, the episodic resurgence of diphtheria, reaching a zenith in the ongoing outbreak, accentuates a pressing necessity to confront the enduring impediment of vaccine hesitancy. 5 Diphtheria, an infectious bacterial ailment, presents as a grave respiratory malady, harboring potential life-threatening ramifications, especially among the pediatric demographic.5,6 The current outbreak, which started in May 2022, characterized as the most severe in several decades, unveils a gaping chasm in immunization coverage, a scenario further aggravated by entrenched vaccine hesitancy within the populace. 5
The historical backdrop of diphtheria control in Nigeria traces a trajectory of intermittent outbreaks, with a notable reduction in incidence following the introduction of diphtheria–tetanus–pertussis vaccine in the national immunization schedule. 7 However, the recent resurge underlines a pivotal concern on the sufficiency and efficacy of the immunization programs. The 1989 outbreak, hitherto the most severe with 5039 cases, was a testament to the potential devastation of diphtheria; yet, the ongoing outbreak surpasses it, signaling a profound public health crisis. As per the data reported by the Nigeria Centre for Disease Control and Prevention (NCDC) on 19 October 2023, there have been 9478 confirmed cases of diphtheria in Nigeria. 8 The recurrent confrontation with diphtheria not only unveils the critical lacunae in immunization uptake 7 but also highlights the imperative for robust public health strategies to ameliorate vaccine hesitancy and fortify immunization frameworks, thereby mitigating the burden of vaccine-preventable diseases in Nigeria.
The sociocultural fabric of Nigeria, a nation with over 250 ethnic groups, engenders a complex milieu that influences health-seeking behaviors, including vaccine acceptance. A melange of factors, including religious beliefs, misinformation, distrust in the healthcare system, and inadequate awareness about the importance of vaccines, brew a potent concoction fueling vaccine hesitancy.5,7 The ramifications of these are stark, as evidenced by the escalating number of diphtheria cases and associated mortalities, primarily among unvaccinated individuals. According to NCDC, up to 80% of the confirmed cases are unvaccinated. 9 The response strategies have encompassed mass vaccination campaigns, community engagement, and public education endeavors to debunk myths surrounding vaccination. 9 Yet, the tenacity of vaccine hesitancy poses a significant hurdle to achieving optimal immunization coverage and curtailing the outbreak.
This piece endeavors to dissect the nexus between vaccine hesitancy and the exacerbation of the diphtheria outbreak in Nigeria. Through a meticulous examination of the sociocultural determinants of vaccine hesitancy, juxtaposed with the epidemiological dynamics of the outbreak, a comprehensive understanding of the multifaceted challenge at hand is sought. In addition, it aims to proffer insights into plausible strategies to ameliorate vaccine hesitancy, enhance immunization coverage, and fortify the public health infrastructure to avert future outbreaks. The narrative here underscores a compelling call for a concerted effort from the global health community, national governments, and local communities to bridge the immunization gap and foster a culture of vaccine acceptance, which is quintessential for the control of diphtheria and other vaccine-preventable diseases in Nigeria and beyond.
Methodology
This perspective review systematically explores the complex landscape of vaccine hesitancy and its impact on diphtheria outbreaks in Nigeria, adopting a comprehensive approach to synthesize insights from a diverse range of sources. Our methodology was grounded in a meticulous literature search aimed at capturing the multifaceted aspects of vaccine hesitancy, including sociocultural, economic, and systemic determinants, as well as public health responses to diphtheria outbreaks.
Literature search and selection criteria
We conducted a thorough search of databases such as PubMed, Scopus, and Web of Science, as well as reports from the WHO, NCDC, and other relevant public health bodies. Keywords used in the search included ‘vaccine hesitancy’, ‘diphtheria outbreaks’, ‘immunization policies’, and ‘Nigeria’, supplemented by additional terms relevant to public health responses and vaccine uptake in Nigeria. The inclusion criteria focused on articles published in English from 1985 to 2023 to encompass the historical and current perspectives on diphtheria management and vaccine uptake challenges in Nigeria. Exclusion criteria were non-empirical studies, articles not focusing on Nigeria or unrelated to vaccine hesitancy and diphtheria, and duplicative reports. The selected articles and reports were critically reviewed to extract relevant information on the dynamics of vaccine hesitancy, patterns of diphtheria outbreaks, and the effectiveness of intervention strategies within the Nigerian context.
The evolving landscape of diphtheria outbreaks in Nigeria (1985–2023)
The resurgence of diphtheria in 2022 has evoked a historical reflection, harking back to the 1989 outbreak. The juxtaposition of these critical junctures furnishes a fertile milieu for assessing the trajectory of public health endeavors, particularly shedding light on vaccination uptakes and public responsiveness. This extensive spread and alarming increase in confirmed cases are graphically represented in Figure 1, which elucidates the flow of diphtheria cases from 1989 to 2023, spotlighting the significant resurgence in 2023 after a period of relative decline.
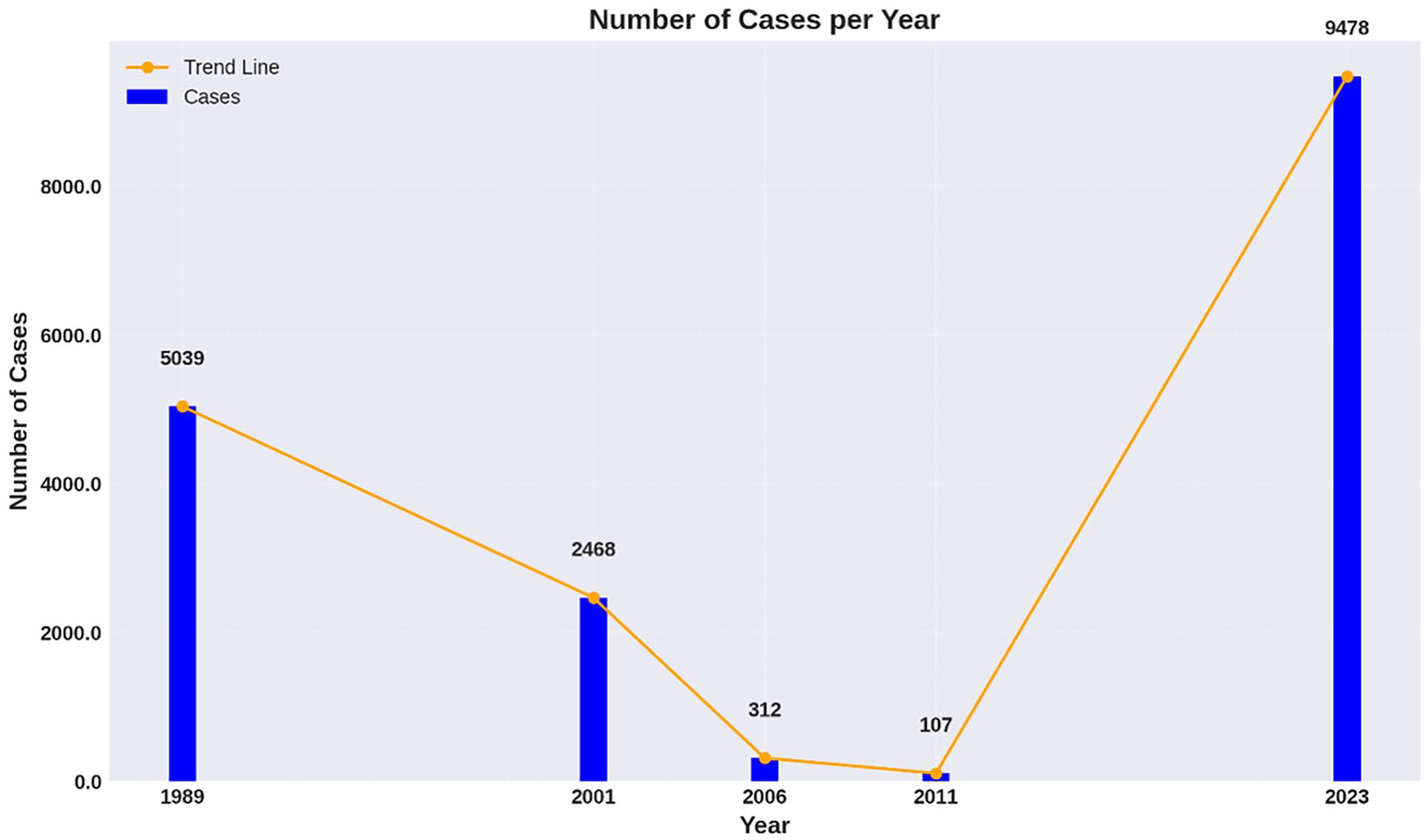
Graphical representation of major diphtheria outbreaks in Nigeria (1989–2023).
According to the archival data from the WHO, a discernible diminution of reported diphtheria cases was observed, dwindling from 5039 in 1989 to 2468 in 2001 and further to 312 in 2006.7,10 The data void post-2006 likely mirrors the inadequacies in the reporting infrastructure and suboptimal disease surveillance within Nigeria. It is noteworthy that a semblance of this downtrend was mirrored in developed nations prior to subsequent diphtheria upsurges.11,12 Subsequently, sporadic reports of probable diphtheria from three distinct geographical realms in Nigeria hinted at a possible resurgence of the malady, with diverse case counts emanating from Lagos, Benin, and Katsina between 2007 and 2010.7,13 This period also witnessed inconsistent immunization coverage, variably oscillating from low to moderate for DPT 3, with the contemporary DPT 3 coverage languishing at 34.9%. 7 The more recent reminiscence in 2011 saw an epidemic unfurling in Borno state, necessitating intervention from Medecin Sans Frontiere to delineate the epidemic contours. 7 A total of 107 probable diphtheria cases were unearthed, culminating in 24 fatalities and a case-fatality ratio of 22.4%. A significant majority of the affected were aged below 10 years, and a staggering 98% had never been privy to any form of childhood immunization. The scenario was further exacerbated by delayed medical intervention and the dearth of antitoxin alongside adequate antibiotic therapy. 7
Fast-forward to the recent alarm on 1 December 2022, where the NCDC in Nigeria was alerted to suspected diphtheria outbreaks in Kano and Lagos states.14,15 As the narrative unfolded into the third week of 2023, a tally of 253 suspected cases of diphtheria emerged across various Nigerian states, including Kano, Yobe, Lagos, and Osun, with 111 confirmed either via laboratory assays or clinical evaluations. 15 To visually capture the extent of the outbreak’s geographical spread and emphasize the regions most affected, Figure 2 presents the distribution of confirmed diphtheria cases in Nigeria by state as of 19 October 2023.

Distribution of confirmed diphtheria cases in Nigeria by state as of 19 October 2023.
The majority of confirmed cases were identified in children aged 2–14 years, with a mere 10.8% having received full vaccination with a diphtheria toxin-containing vaccine. 15 As of 19 October 2023, the NCDC unveiled a staggering figure of 9478 confirmed cases, predominantly affecting children between the ages of 1–14, encapsulating 71.5% of the confirmed cases. 8 The geographical spread of the disease was elucidated by the Director General of NCDC, Dr. Ifedayo Adetiba, during a media briefing, revealing an extensive spread across 137 Local Government Areas in 20 states, including the Federal Capital Territory. The breakdown divulged a significant concentration of cases in Kano, followed by Yobe, Bauchi, and other states. 8 As of 12 October 2023, the diphtheria outbreak has taken a tragic toll, with over 600 deaths reported, primarily among children. 16 This situation further evolved, as WHO Africa reported on 14 January 2024 that there were 22,417 suspected cases, 13,477 confirmed with 593 confirmed deaths (Case Fatality Rate 2.6%). 17 The discrepancy in reported figures over time paints a concerning picture, highlighting the challenges in outbreak monitoring and data accuracy.
Among these reports, a common denominator was the youthful age of the affected, predominantly under 15 years, coupled with a remarkable case fatality rate across the regions and a conspicuous absence of definitive management, notably diphtheria antitoxin (DAT).
Public health intervention to contain the ongoing outbreak
Amidst the escalating diphtheria outbreak, a swift, unified response has been mobilized under the aegis of the Honourable Coordinating Minister of the Federal Ministry of Health and Social Welfare (FMOH&SW), Professor Muhammad Ali Pate. 9 A National Emergency Task Team, co-chaired by the helm of the National Primary Healthcare Development Agency (NPHCDA) and the NCDC, has been assembled, fostering a collaborative front among critical health stakeholders, and global health allies such as WHO, UNICEF, USCDC, and GAVI. The response framework embarks with the formation of the Diphtheria Emergency Task Team, converging with the National Diphtheria Emergency Operations Centre at NCDC, thus laying the groundwork for coordinated, multi-faceted initiatives to tackle the outbreak. This is further amplified by the deployment of National Rapid Response Teams (NRRT) to afflicted states and the drafting of National Diphtheria Surveillance and Response guidelines, ensuring adept surveillance and diagnostic proceedings. 9
The provision of critical therapeutics like DAT and intravenous erythromycin marks a significant stride in case management, facilitated by the FMOH&SW through NCDC with indispensable support from WHO. Concurrently, the establishment of Diphtheria Treatment Centres/Wards alongside the State Ministry of Health delineates a structured clinical response. 9 The immunization ambit witnesses a surge in routine diphtheria immunization activities and reactive vaccination campaigns orchestrated by the NPHCDA, targeting the significant vaccination lacuna, especially among the 5–14-year-olds. Risk Communication and Community Engagement are propelled through an array of strategies, including public health advisories dissemination, media engagements, and community sensitization campaigns, aiming for a community-centric approach to diphtheria containment. 9 This response framework, underpinned by a collaborative ethos and public engagement, aspires not only for a robust containment of the diphtheria outbreak but also fortifying Nigeria’s public health infrastructure against impending infectious disease threats.
Vaccine hesitancy in Nigeria
The complex sociocultural tapestry of Nigeria significantly underpins the phenomenon of vaccine hesitancy, with myriad factors intertwining to influence public perception and acceptance of vaccination.18–20 Traditionally, a diverse array of beliefs and practices across the country’s over 250 ethnic groups has molded health-seeking behaviors, often transcending scientific evidence. Religious beliefs, in particular, have been noted to play a pivotal role, with certain factions disseminating anti-vaccine narratives based on doctrinal interpretations. 20 Moreover, the political landscape and historical episodes of distrust toward governmental health initiatives further exacerbate vaccine hesitancy. Systemic factors, including the accessibility and quality of healthcare services, also play a crucial role. 19 The sporadic availability of vaccines, coupled with inadequately equipped healthcare facilities and personnel, often deters individuals from seeking vaccination, perpetuating a cycle of hesitancy.18,20
Vaccine hesitancy fueling the present outbreak
The unfolding diphtheria epidemic in Nigeria starkly illuminates the perilous ramifications of vaccine hesitancy within the public health panorama. Noteworthy is the glaring fact that over 80% of confirmed cases are among the unvaccinated populace,9,21 a statistic that accentuates the chasm wrought by vaccine hesitancy, thus leaving vast swathes of the community vulnerable to diphtheria and sparking a pervasive transmission trajectory across societal bounds. The individuals devoid of vaccination not only bear a heightened susceptibility to diphtheria but also morph into vectors for the bacterium’s dissemination, thereby thwarting the aspirations of attaining herd immunity and containing the outbreak. Moreover, the hesitancy quagmire has cast a pall over response strategies, manifesting as a diminished turnout in vaccination drives and consequently protracting the timeline requisite for outbreak containment.3,20
Amidst the ongoing diphtheria outbreak in Nigeria, the call for extensive vaccination drives resonates with a stark urgency. As of now, a staggering figure of 14 million children require vaccination to curb the menacing spread of diphtheria. 22 In response, the initial two phases of the UNICEF-led immunization campaigns have yielded commendable coverage, administering vaccines to 7,504,981 children. However, the path to achieving comprehensive immunization is fraught with financial constraints. A report from UNICEF delineates a funding shortfall of US$3.85 million, which is requisite for an efficacious outbreak response across seven states, as discerned on 12 October.
The narrative of Kano exemplifies the challenges in meeting vaccination targets. Here, a modest number of 68,109 children have been vaccinated under the Penta regimen, which starkly represents only 14% of the target population encompassing children aged between 6 weeks to 4 years, with the target figure standing at 475,153. 22 To further understand vaccine hesitancy in Nigeria, especially in the context of such figures, it is imperative to examine the sociocultural dynamics, particularly in Northern Nigeria. High birth rates and specific beliefs significantly influence vaccine acceptance in this region.23,24 Some communities hold a pervasive perception that vaccines are part of an agenda to reduce birth rates, a belief fueled by misinformation and distrust in external interventions. 23 Similarly, in the case of the diphtheria outbreak, recent incidents have further complicated efforts to combat vaccine hesitancy. Reports of two mothers claiming their children developed kidney complications after receiving diphtheria vaccines in Kano have revived old vaccine safety fears in the region. 25 These claims, aired by a local radio station and widely shared online, have contributed to increased skepticism toward the diphtheria vaccine. 25 Such challenges are not new to the region. Historical vaccine safety scandals, including the adverse events following an experimental meningitis vaccine trial in 1996, have left a lasting impression on the community’s trust in vaccination campaigns. 25 These past and present concerns highlight the complexity of addressing vaccine hesitancy in Nigeria, necessitating a multifaceted approach that includes accurate information dissemination, engagement with community leaders, and sensitivity to local beliefs and historical contexts.
The tapestry of vaccine hesitancy, intricately interwoven with the current diphtheria outbreak, unfurls a broader dialog on the public health preparedness and community engagement ethos within Nigeria. The imperative to confront and mollify vaccine hesitancy surpasses the immediacy of outbreak containment; it embodies a longitudinal endeavor to engender a culture imbued with trust, acceptance, and adherence to vaccination paradigms, a cornerstone for thwarting and managing vaccine-preventable maladies.
Fortifying vaccination uptake as a pathway to diphtheria containment
The burgeoning diphtheria outbreak in Nigeria underscores the imperative of vaccination as a linchpin of effective public health response. 15 However, the endeavor to bolster immunization uptake is oftentimes at loggerheads with ingrained cultural and religious sentiments that act as deterrents to vaccination. 20 As such, navigating this intricate socio-religious milieu necessitates a nuanced, culturally sensitive, and multifaceted strategy. These include:
Develop tailored public health messaging that aligns with cultural and religious values, using vernacular languages for broader reach and transparently communicating the benefits and risks of vaccination.
Engage with religious and community leaders to endorse vaccination, leveraging their influence to shift community perceptions and foster acceptance.
Conduct culturally attuned education and awareness campaigns through local media channels to dispel myths and address fears about vaccination.
Provide accessible and respectful vaccination services that are non-discriminatory and sensitive to cultural and religious norms.
Train healthcare workers in cultural competence to ensure they communicate effectively and respectfully with diverse populations.
Promote community-centric vaccination initiatives that encourage community ownership and align with local customs and practices.
Establish and utilize feedback mechanisms to gather community input on vaccination services, facilitating ongoing improvement of service delivery.
Advocate for policies that support culturally sensitive vaccination programs and include culturally relevant indicators in monitoring and evaluation efforts to assess and enhance vaccine acceptance.
Policy advocacy should aim at engendering governmental and organizational backing for culturally sensitive vaccination programs, ensuring that immunization policies are inclusive and respectful of cultural and religious diversity. Moreover, the integration of culturally sensitive indicators within the monitoring and evaluation framework will be instrumental in gauging the efficacy of interventions aimed at ameliorating vaccine acceptance and uptake amidst a backdrop of cultural and religious diversity.26,27 A prime example of the impact of such tailored approaches is the successful eradication of polio in Nigeria. The country’s triumph over polio, declared polio-free by the WHO in August 2020, 28 aggrandizes the potential of dedicated vaccination campaigns that respect and address the nuanced challenges posed by Nigeria’s diverse cultural and religious landscape. This success story not only illustrates the critical importance of community engagement and the adaptation of strategies to local contexts but also serves as an inspiring model for tackling other infectious diseases through vaccination.
Following this example, a holistic, inclusive blueprint that incorporates lessons learned from the polio eradication effort not only offers a robust response to the current diphtheria menace but also augments the immunization infrastructure against prospective outbreaks of vaccine-preventable diseases within a culturally and religiously diverse demographic. This integrated approach, exemplified by the polio campaign’s success, highlights the importance of sustained, culturally sensitive public health initiatives in achieving widespread vaccine coverage and disease eradication.
Limitations of the review
In our comprehensive exploration of the sociocultural and systemic determinants shaping vaccine hesitancy, this review unveils critical insights yet encounters inherent constraints in delineating the precise impact of these factors on vaccination rates and the dynamics of the diphtheria outbreak in Nigeria. Despite recognizing the substantial role of vaccine hesitancy in undermining immunization efforts, the review grapples with a scarcity of region-specific studies and comprehensive datasets, limiting our capacity to quantitatively anchor this relationship within the wider public health discourse. References to reports from the NCDC and other published sources underline the prevalence of diphtheria among unvaccinated individuals; however, the absence of nuanced, directly correlational data leaves a gap in our understanding. Moreover, our position as external researchers, distanced from the immediate response mechanisms but deeply engaged in infectious disease epidemiology, inherently restricts our perspective to the publicly available information. This limitation, while reflective of the broad challenges confronting academic inquiry into public health crises, underlines the critical need for more granular, accessible data to inform and refine our understanding of vaccine hesitancy’s impact on outbreak management and immunization strategies.
Conclusion
The narrative of Nigeria’s struggle against the worst diphtheria outbreak in decades unravels a complex tapestry of challenges and opportunities in public health. It beckons a critical examination of the existing immunization policies, unraveling the nuanced interplay of vaccine hesitancy, sociocultural dynamics, and systemic impediments. The discourse transcends the immediate exigency of controlling the outbreak, extending to a broader spectrum of immunization and infectious disease control. The pivotal role of international collaboration, underscored by the contributions of global health entities, amplifies the essence of a unified front against vaccine-preventable diseases. This piece has elucidated the multifaceted dimensions of the diphtheria outbreak in Nigeria, from the lens of vaccine hesitancy to the policy implications, providing a foundational premise for envisaging robust, culturally resonant, and sustainable public health strategies. The reflections herein are not merely an academic exercise but a clarion call for a concerted effort toward bolstering immunization uptake, nurturing a culture of vaccine acceptance, and fortifying the public health infrastructure. The journey toward a diphtheria-free Nigeria and enhanced public health resilience is a collective endeavor, necessitating the synergy of policy-makers, healthcare professionals, communities, and the global health community. Through a meticulous synthesis of lessons from history, contemporary challenges, and global best practices, the roadmap toward achieving these objectives can be envisioned and actualized.