
Abstract
Objective:
This scoping review aimed to describe studies that evaluate the management of cryptococcal meningitis (CM) using cerebrospinal fluid (CSF) shunts, types of shunts used, and clinically relevant patient outcomes.
Methods:
We searched in the following databases: PubMed, Web of Science/Core collection, Embase, the Cochrane Library, and clinicaltrials.gov on 1 April 2022. We included two-arm and one-arm cohort studies that evaluated clinically relevant patient outcomes. Case reports were used to describe the type of CSF shunts used and the rationale behind its selection. The selection and extraction processes were independently performed by two authors.
Results:
This study included 20 cohort studies and 26 case reports. Only seven cohort studies compared two groups. Ventriculoperitoneal shunt was the most commonly used type of shunt (82.1%). The main indications for placing a shunt were persistently high opening pressure (57.1%) and persisting neurological symptoms or deterioration (54.3%). Cohort studies suggest that patients with shunt showed improvement in some outcomes such as neurological symptoms and hospital stay length. The most common shunt complications were post-operative fever (1–35.6%) and shunt obstruction (7–16%).
Conclusion:
CSF shunts may improve some clinically relevant outcomes in patients with CM, but the evidence is very uncertain.
Introduction
Cryptococcosis is a systemic fungal disease caused by species of the Cryptococcus genus, namely Cryptococcus neoformans and C. gatti. 1 The prevalence of cryptococcosis is 5–10% in immunocompromised patients. 2 It is unusual in immunocompetent patients, but they may account for up to one-third of all cases.3,4 Cryptococcosis results in up to 280,000 cases and 130,000 deaths yearly, with an estimated 152,000 cases and 112,000 deaths in patients with acquired immunodeficiency syndrome. 5 Both C. neoformans and C. gatti have marked neurotropism, therefore cryptococcal meningitis (CM) is the most common clinical presentation. 6 Cryptococcal cells and shed polysaccharide capsule cause inflammation of the meninges and underlying brain tissue, leading to plugging and fibrosis of arachnoid villi, resulting in insufficient cerebrospinal fluid (CSF) drainage and increased intracranial pressure (ICP) due to communicating hydrocephalus. Failure to control ICP in the context of CM has been associated with worse clinical outcomes, including hearing loss.7,8 Antifungal therapy is the hallmark of treatment, and current guidelines recommend basal measurements of ICP and management of increased ICP using lumbar puncture. 9 When lumbar puncture fails to control ICP, it is recommended to place CSF shunts, with various types of shunts used in different settings and varying degrees of success. 10 The most common devices are the ventriculoperitoneal shunt (VPS), lumboperitoneal shunt (LPS), and auriculoventricular shunt (AVS). Although there is no global estimate on the frequency of CSF shunting in CM, a Thai study reported an 19% prevalence, reaching as high as 55% in those with hydrocephalus. 11
Historically, the benefits of shunt placement have been outweighed by the risk of infection, shunt obstruction, and peritoneal fungal seeding.12,13 However, recent studies suggest the opposite. Some studies suggest that VPS placement in severely immunosuppressed human immunodeficiency virus (HIV)-infected patients with persistently elevated ICP due to CM have good outcomes.10,14,15 Moreover, they have addressed that its benefits such as long-term symptom control due to ICP lowering and reducing the risk of infection resulting from external lumbar drain placement may outweigh the risk of potential infection.10,16 Regarding the type of CSF shunting, several studies have shown a higher therapeutic failure in LPS placement in comparison to VPS placement.16,17 Furthermore, similar rates of distal-end complications have been described in AVS and VPS. 18 Thus, the evidence on the use of shunts for CM remains unclear.
Summarizing the results and describing studies evaluating CSF shunts in the management of CM is important for evidence-based clinical decision-making. However, high-evidence level research is lacking on this topic. We undertook this study to describe the clinically relevant outcomes in patients with CM, types of shunts used, when to use them, the indications, and associated complications.
Methods
We conducted a scoping review in accordance with the Preferred Reporting Items for Systematic and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) guidelines of 2018. 19 Our study protocol was registered on the Figshare platform, under the title ‘Shunting in Cryptococcal meningitis: a scoping review’. The full checklist is available in Supplemental Material 1.
Eligibility criteria
This scoping review aimed to examine studies of patients diagnosed with CM who have undergone CSF shunting. Both immunocompetent and immunocompromised patients were included in the study. To evaluate important patient outcomes, we included two-arm cohort studies (comparing patients with and without shunts) and one-arm cohort studies (including only patients with shunts). The important outcomes evaluated were mortality, quality of life, relapse, neurological status, and any complications related to the surgery, such as surgical site infection, shunt obstruction, and bleeding. Additionally, we also analyzed cohort and case report studies that mentioned the type of CSF shunting procedure used and the rationale behind its selection.
Literature search
We conducted a comprehensive search of multiple databases, including PubMed, Web of Science/Core collection, Embase, the Cochrane Library, and clinicaltrials.gov. The search was conducted on 1 April 2022, without any limitations on language or publication date. The search terms were organized into two categories: ‘Meningitis, Cryptococcal’ and ‘Cerebrospinal Shunt’, with the full search strategy detailed in Supplemental Material 2.
Study selection
Manual duplicate removal and study selection was done using Rayyan software (Rayyan QCRI, Qatar Computing Research Institute).19,20 Two authors (XC and ASS) independently reviewed the titles and abstracts of the results to identify potentially relevant studies for inclusion. These studies were then evaluated in full-text by the authors (GC-V and XC) independently. Any discrepancies in study selection were discussed and resolved through consensus with another author (DRS-M).
Data extraction
A standardized data extraction sheet was created using Microsoft Excel, and the data of interest were independently extracted by the authors (GC-V, XC, and ASS). Any discrepancies were resolved through discussion with two different authors (DRS-M and JA). The following variables were extracted from each study: author, year of publication, study design, sample size, population details (age, sex, immunological status, clinical presentation, prior treatment before CSF shunting), intervention details (type of CSF shunt, indication for placing the shunt), outcomes in patients with and without shunt, and complications related to shunt.
Synthesis
The information extracted from the articles is presented in the form of tables and figures displaying relative frequencies, providing a descriptive overview of the data.
Results
Selection
The database search yielded 255 records after deduplication. These records were screened by title-abstract where 102 were retained for assessment at the full-text. Finally, 46 studies met the eligibility criteria and were included in the review (Figure 1). Reasons for exclusion of studies in full-text selection can be found in Supplemental Material 3.

Flow diagram summarizing the process of literature search and selection.
Characteristics of the studies
Of the 46 studies included, 20 were cohorts4,10,14–18,21–33 and 26 were case reports/series.12,34–58 The cohort studies were divided in 7 two-arm (groups with and without shunt) and 13 one-arm (group with shunt) studies, and their characteristics are summarized in Table 1.
Characteristics of included cohort studies (n = 20).

AmB, amphotericin B, AmBd, amphotericin B deoxycholate; AMS, altered mental status; CS, corticosteroids; DB, diabetes; EVD, external ventricular drainage; 5-FC, 5-flucytosine; HBV, hepatitis B; HIV, human immunodeficiency virus; ICP, intracranial pressure; LFAmB, lipid formulations of amphotericin B; LP, lumbar punctures; NR, not reported; N/V/D, nausea/vomiting/dizziness; TBC, tuberculosis; VA, ventriculoatrial; VP, ventriculoperitoneal.
Of the seven two-arm studies included, four were conducted in China, two in the USA, and one in Uruguay. All of them were retrospective cohorts. The sample size ranged between 10 and 257 patients. Most studies included patients with ages between the third and fifth decade of life. Six of seven studies had patients with HIV infection as the primary cause. Headache and altered mental status were the most common clinical presentation in the majority of studies. Most studies reported treatment with amphotericin B, fluconazole, and 5-flucytosine combinations. The non-pharmacological approach included serial lumbar punctures (three studies) and ventriculostomy (one study).
Regarding the 13 one-arm studies, seven were conducted in China, two in the USA, two in Taiwan, and one study in each Brazil and Australia. All of them were retrospective cohorts. The sample size varied between 9 and 128. Nine studies included patients with immunosuppression, in three studies the immune status was not reported and in one study patients were immunocompetent. In three studies clinical presentation was not reported. The majority of the studies used pharmacological treatment with different combinations of amphotericin B, fluconazole, voriconazole, or 5-flucytosine. Five studies used non-pharmacological treatments, four were lumbar punctures, and one an external ventricular drainage and craniotomy. Three studies did not report the treatment. The characteristics of case reports/series are presented in Supplemental Material 4.
Most studies did not report dosage and timing of antifungal therapy. Only nine studies (45%) did specify dosage and timing.4,16,21,22,24,28,29,31,32
Type of shunts used
The type of shunt used was reported for 397 patients. VPS was the most frequent one (82.1%), followed by LPS (10.3%) and AVS (7.6%) (Figure 2).
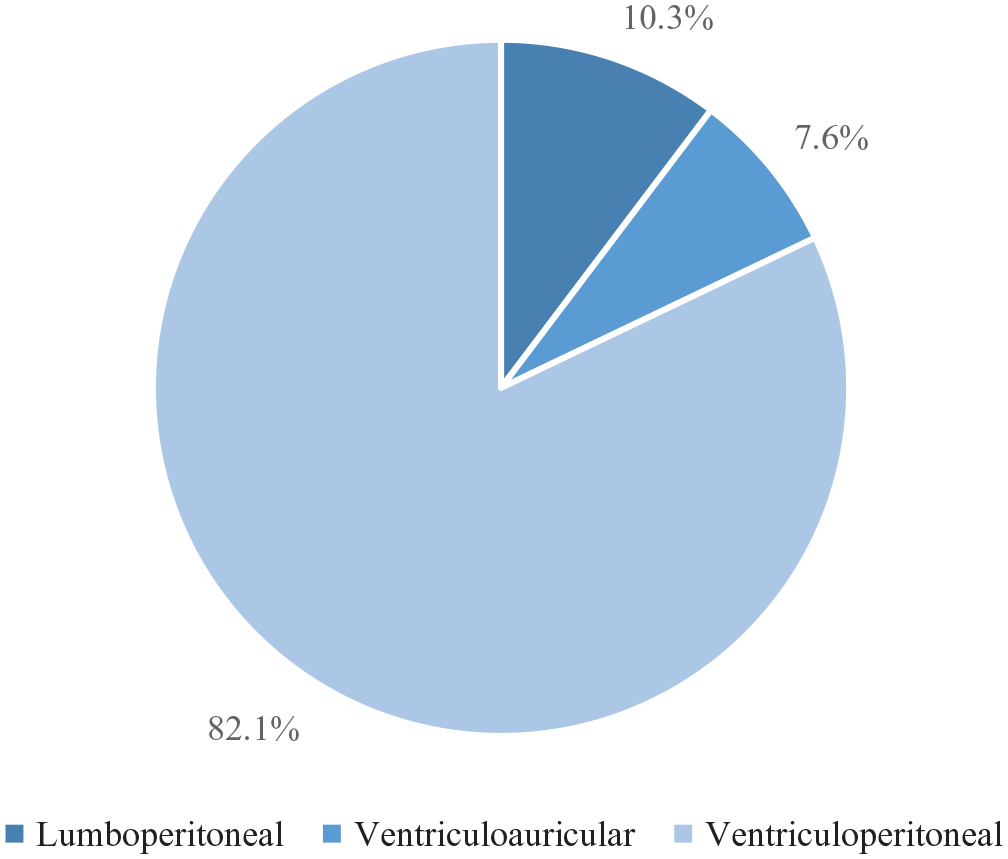
Types of cerebrospinal fluid shunts used for cryptococcal meningitis (n = 397).
Shunt placement indications
When evaluating CSF shunt placing indications, we found information in 35 studies including case reports and cohort studies. The main indications were persistent high opening pressure (57.1%) and persisting neurological symptoms and/or deterioration (54.3%). Persistent headache was reported in 31.4% of the studies. Other indications were hydrocephalus or ventriculomegaly (25.7%) and patients not tolerating further lumbar punctures (17.1%) (Figure 3).
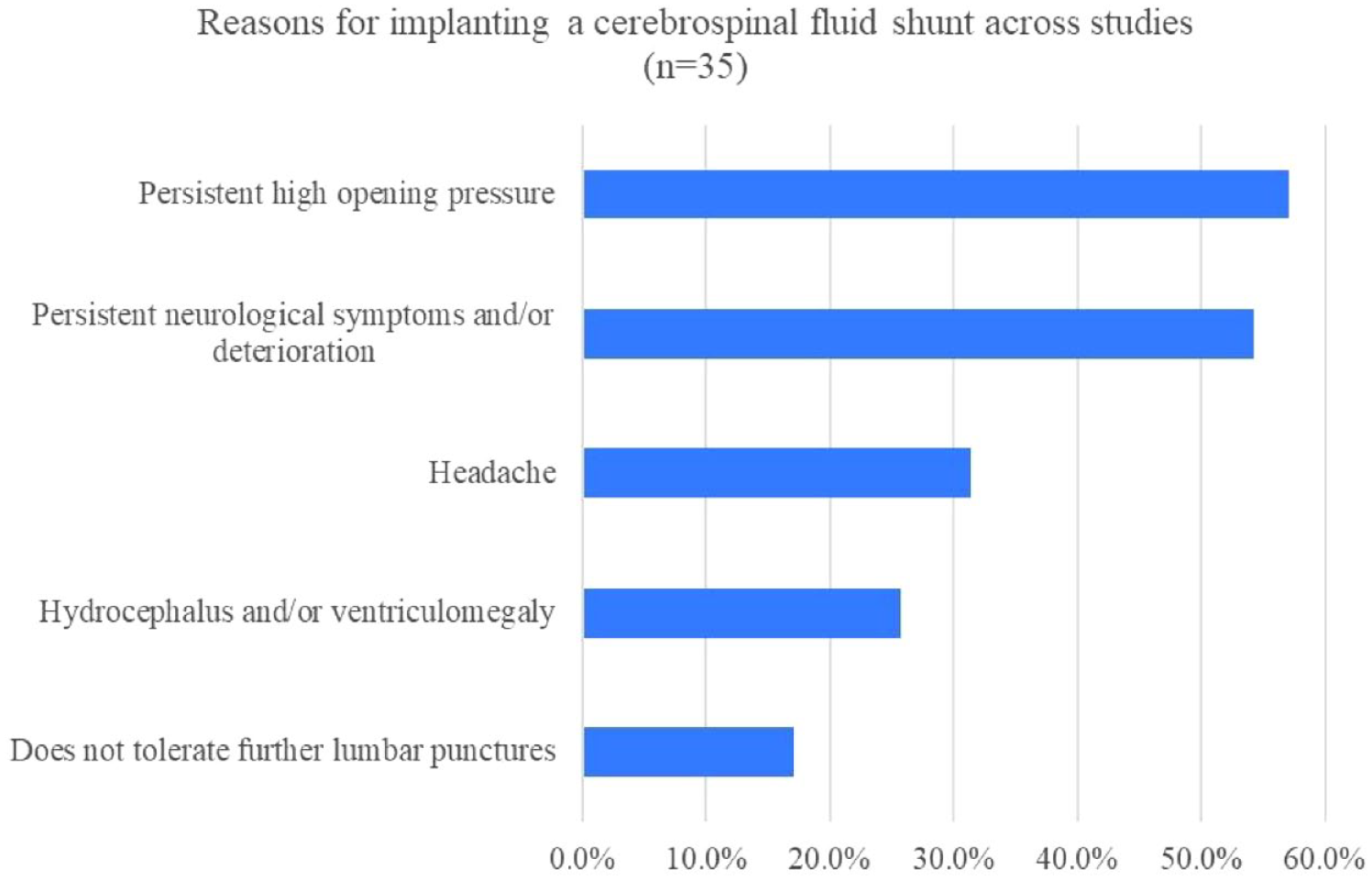
Indications for placing a cerebrospinal fluid shunt across studies (n = 35).
Outcomes
In the group of two-arm studies, six of them reported mortality. Mortality in patients with shunts was between 4% and 54% [median: 8.5, interquartile range (IQR): 25] and in patients without shunt mortality was between 0% and 75% (median: 35.5, IQR: 36). In the group of patients with shunt, three studies showed that more than 80% of patients had improvement of symptoms. In two studies, length of hospital stay (LOS) was reported, Liu et al. 15 reported that the mean LOS was 62.8 days in patients with shunt and 73.5 days in patients without it. Li et al. 21 reported a median of 25 days of LOS in the group with shunt and a median of 77 days in the group of patients without shunt. In the one-arm studies, mortality was assessed in four studies, ranging between 4% and 22% in patients with shunt. In five studies, more than 50% patients with shunt presented improvement in neurological status. Two studies did not report outcomes (Table 2).
Shunt characteristics and outcomes in cohort studies (n = 20).

LPS, lumboperitoneal shunt; NR, not reported; POF, post operative fever; VAS, ventriculoauricular shunt; VPS, ventriculoperitoneal shunt.
Complications related to shunt
Of the seven two-arm studies, five of them described complications related to shunts. Postoperative fever was frequently reported (1–36%). Shunt obstruction (7–16%) and shunt-related infection (1–4%) were the most common complications. Only one study reported shunt revision as a complication (15%). In the group of one-arm studies, six studies did not report complications related to shunt. Of the seven studies that described complications related to shunt, these included shunt replacement (10–31%), shunt obstruction (1–11%), shunt revisions (20–29%), and shunt-related infection (1–14%). Other complications are shown in Table 2.
Discussion
This study is the first scoping review evaluating the use of CSF shunts in patients with CM. The majority of studies did not compare the outcomes of patients with shunt to those without shunt. The most used type of shunt was the VPS. Shunts were primarily placed due to elevated opening pressures, persistent neurological symptoms, or deterioration. Taking all the results together, shunts could lead to an improvement in clinically relevant outcomes such as resolution of neurological symptoms and LOS. Furthermore, postoperative fever and shunt obstruction were the most common complications. However, evidence regarding these findings is limited by the quality of available studies.
Randomized clinical trials are considered the optimal method for evaluating the efficacy of an intervention. However, for CSF shunts in CM, this may not be feasible. In this scoping review we found 20 cohort studies and 26 case reports, suggesting a shortage of evidence. Although cohort studies could provide valuable information by comparing patients with and without shunts and evaluating important outcomes, only 2 of the 20 included cohort studies in this review had the main objective of evaluating the effect of shunts compared to no shunts.21,22 These studies found improvements in survival and hospital stay length.21,22 Regarding the characteristics of the included studies, we found clinical heterogeneity in the immune status of patients and pre-shunting treatment. The immune status of patients varied from immunocompetent to HIV, and other types of immunosuppression; and pre-shunting treatment included antifungal therapy, ICP lowering medication, serial lumbar punctures, etc. Therefore, these findings could not be generalized to all populations and further studies in different patient groups are needed to clarify the role of CSF shunts in the management of CM.
Likewise, we describe the type of shunts and the criteria for placing these devices. Similarly, both the Infectious Disease Society of America (IDSA) and the World Health Organization (WHO) recommend permanent shunt placement only after appropriate antifungal therapy has been administered and conservative measures, such as lumbar punctures, percutaneous lumbar drains, or ventriculostomy, have failed to control increased ICP.9,59 IDSA recommends only VPS while WHO also recommends LPS.9,59 The predominance of VPS usage in this review may be attributed to these recommendations. Only a few studies described the indications for choosing a specific type of shunt. For instance, Guang et al. 39 mentioned choosing an AVS due to its lower risk of abdominal adhesions, and smaller operatory field. Park et al. 18 described the choice as surgeons’ preference. It appears that the type of shunt employed is mainly influenced by both surgeon preference and expertise. Shunt indications mirrored those published in IDSA and WHO guidelines.9,59 The study by Zhao et al. 24 is noteworthy because it used the largest number of AVS in any study we reviewed. However, the indication for the preference over VPS or LPS was not mentioned. We suggest that future studies should stablish objective criteria for selecting one type of shunt over others.
Regarding clinically important outcomes, we found varying mortality rates among patients with and without CSF shunting procedures: five studies showed lower mortality in patients who underwent CSF shunting procedures than in those who did not, whereas two studies showed higher mortality in patients who underwent CSF shunting procedures than in those who did not.10,21 However, we cannot rule-out a bias toward shunting the more severely ill patients, thus resulting in worse prognosis and higher mortality in this subgroup of patients. This may lead to the benefit of CSF shunting being underestimated. Nonetheless, the opposite could be true and very ill patients may not be shunted due to a higher true or perceived surgical risk. This bias may also arise from the lack of consistent criteria for placing the shunt. In order to bridge this knowledge gap, we believe prospective cohort studies adjusted by cofounding variables such as illness severity, immune status, and age, would minimize this bias.
In addition, most studies reported clinical improvement in more than half of the patients. However, these studies used nonspecific terminology such as ‘improvement of neurological symptoms’ or ‘restoration of premorbid mental status,’ which may not be as informative when considering clinical decision-making for long-term morbidity and sequelae. A single study reported improvement on an individual symptom basis, revealing similar improvement in visual and auditory symptoms in both the shunting and non-shunting group. 22 On the other hand, two studies reported LOS, with a trend toward shorter stays in the shunt group.15,21 We encourage future studies to include this important, yet underreported outcome.
Previously, studies have suggested that complications of CSF shunting may outweigh its benefits.10,16 However, our review found a rather low prevalence of severe complications. The most clinically relevant outcomes were shunt malfunction and infection. Nonetheless, no studies defined criteria for shunt malfunction, as previously described.10,17,30,60 Only one case of abdominal seeding of cryptococcal infection was reported, 21 despite this being considered a major complication in previous literature.12,13,27,61 A single study compared outcomes among shunt types: mortality was higher in the VPS group than in the AVS group. 24 However, small sample sizes limit the utility of this finding. AVS is usually a second-line option for CSF shunting, used when the peritoneum is not suitable due to adhesions or infection. Despite the limitations in the quality of available data, we believe that shunts are a beneficial intervention in the management of ICP in CM in selected patients.
The studies included in this review had several limitations. First, only 7 out of 46 studies were two-arm, meaning that they included a population with and without shunt, and there were no randomized clinical trials. All longitudinal studies were retrospective. This limits the ability to draw solid conclusions about the efficacy of CSF shunting as a treatment for CM. Furthermore, the sample sizes of the studies were relatively small, ranging from 10 to 257 patients, which may not be representative of the larger population. Furthermore, most of the studies were conducted in China, with only a small number of studies from other countries. No studies were from sub-Saharan Africa, which is where the highest burden of disease is. We believe this may be due to unavailability of materials and expertise. Additionally, the studies had a heterogeneous immune status and pre-shunting treatment. Finally, there are important variables which we aimed to describe in this scoping review, such as the time from diagnosis to shunt placement or the indications for placing one type of shunt over others. Unfortunately, lack of available data rendered this impossible.
Based on the findings of the present scoping review, it appears that CSF shunting could be a beneficial intervention in clinically relevant outcomes for patients diagnosed with CM who despite proper CSF drainage by lumbar puncture persist with increased ICP, and with low severe complication rates. However, it is important to note that while the current article provides insight into the most common indications for using a shunt in patients with CM, the criteria for determining when to use a shunt remain uncertain. IDSA guidelines recommend shunt placement be reserved for failure of antifungal therapy and conservative measures (serial LPs, lumbar drainages), albeit based on evidence from opinions of respected authorities. 9 Ultimately, the decision to utilize a shunt is primarily based on clinical judgment, and further research is needed to establish clear guidelines and objective criteria for determining when a shunt is the appropriate intervention. These results should be further validated through larger, prospective two-arm studies. Ideally, studies should evaluate statically significant differences using effect measures or p values. 22 Additionally, future research should aim to investigate a wider range of outcomes, including quality of life, relapse rates, shunt revision rates and indications for this, LOS, and more-detailed description of neurological impairments, including visual loss and hearing loss evaluated through validated scales (e.g. extended disability status scale). 62 In addition, studies should provide more detailed information on the indications behind the selection of specific types of shunts and the rationale behind their use.
The methodology of this scoping review has several limitations. First, the study did not include any unpublished literature, which may have led to the exclusion of relevant studies. Also, the data on the indications for shunt placement were obtained considering the number of studies and not the number of patients as the denominator, due to the limited availability of data. On the other hand, this review follows the PRISMA-ScR guidelines, which provides a structured and transparent approach to conducting a scoping review. The literature search was conducted on multiple databases, which increases the chances of finding relevant studies. Finally, we believe this scoping review will serve to guide future research in this topic.
This review evaluated observational studies on the use of CSF shunting in patients with CM. The most used shunt was the VPS. Shunts were placed mainly due to elevated opening pressure and symptoms or neurological deterioration, with low complication rates. Our results suggest that in patients with shunt, there is an improvement in clinically relevant outcomes such as neurological symptoms and LOS. Future studies should be prospective, and compare clinically relevant outcomes in patients with shunt to those without shunt, identifying optimal timing for shunt placement, and describing in detail the most important complications.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241228666 – Supplemental material for Cerebrospinal fluid shunting for the management of cryptococcal meningitis: a scoping review
Supplemental material, sj-docx-1-tai-10.1177_20499361241228666 for Cerebrospinal fluid shunting for the management of cryptococcal meningitis: a scoping review by Gonzalo Cornejo-Venegas, Xosse Carreras, Andrea S. Salcedo, David R. Soriano-Moreno, Jorge L. Salinas and Jorge Alave in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-2-tai-10.1177_20499361241228666 – Supplemental material for Cerebrospinal fluid shunting for the management of cryptococcal meningitis: a scoping review
Supplemental material, sj-docx-2-tai-10.1177_20499361241228666 for Cerebrospinal fluid shunting for the management of cryptococcal meningitis: a scoping review by Gonzalo Cornejo-Venegas, Xosse Carreras, Andrea S. Salcedo, David R. Soriano-Moreno, Jorge L. Salinas and Jorge Alave in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
The authors would like to thank Carolina Mendez-Guerra for her support in the review protocol.
Authors’ note
Our study protocol was registered on the Figshare platform, under the title ‘Shunting in Cryptococcal meningitis: a scoping review’.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.