
Abstract
Background and objective:
Fungal empyema is a rare entity which is associated with high mortality. It is mostly seen in immune-compromised hosts. However, there is limited data available on fungal empyema from developing countries regarding risk factors, treatment, and outcome. This study was conducted to determine the risk factors, clinical features, treatment, and outcome of fungal empyema.
Methods:
A retrospective observational study was performed on proven fungal empyema cases, admitted at Aga Khan University Hospital, Karachi, Pakistan during January 2018 to May 2021. We excluded all those patients with polymicrobial bacterial and fungal empyema or with negative pleural fluid cultures. A preformed questionnaire was filled out for each case.
Results:
A total of 26 patients were diagnosed with fungal empyema with a mean age of 43.6 ± 20.3 years. Of these, 16 (61.5%) patients were male. Diabetes mellitus was the most frequent comorbidity (n = 11, 42.3%), followed by hypertension (n = 9, 34.6%), malignancy (n = 6, 23.1%), and asthma (n = 1, 3.8%). Ten (38.5%) patients had multiple comorbidities. Candida spp. was isolated in 21 (80.8%) patients and Aspergillus spp. in 7 (26.9%) patients. Fusarium spp. was isolated from one (3.9%) patient. Video-assisted thoracoscopy surgery was done in 14 (53.8%) patients and 12 (46.1%) patients were managed with tube thoracostomy. Twenty-one (80.8%) patients received antifungal agents. Overall, in-hospital mortality was 38.5% (n = 10) and all patients developed respiratory failure. Clinical improvement was seen in 16 (61.5%) patients.
Conclusion:
Our data suggest that fungal empyema has a poor outcome as almost one-third of our patients died. Early diagnosis and intervention can improve outcome.
Plain language summary
• This study was carried out as there are limited data available globally on fungal empyema.
• We conducted a retrospective case study of 26 patients and our findings suggest that the fungal empyema has a poor outcome.
• One third of our patients died during hospital stay.
• Early diagnosis and treatment are important in fungal empyema.
• Diabetes mellitus was found as a possible risk factor for fungal empyema, which should be evaluated further in future studies.
Introduction
The accumulation of pus between the lungs and pleural cavity is known as empyema. Empyema could be due to bacterial or fungal agents. Community-acquired empyema is commonly seen with aerobic Staphylococcus and Streptococcus species and gram-negative bacteria like Escherichia coli, Haemophilus influenzae, and Klebsiella pneumoniae while hospital-acquired empyema is commonly caused by methicillin-resistant Staphylococcus aureus and gram-negative organisms including Pseudomonas.1,2
Fungal empyema is a rare etiology but associated with a much higher mortality, as high as 70%, and is usually caused by Candida species.1,2 Commonly, fungal empyema is acquired in intensive care units (ICU) due to abdominal pathology followed by bronchopulmonary infection and chest surgery. 2 A recently published study reported Candida albicans (65%), followed by Candida glabrata (26%), Candida parapsilosis (11%), and Candida tropicalis (4%) as the most common organisms in fungal empyema. 3
Compared to bacterial empyema, fungal empyema has been reported to be associated with longer hospital and ICU stay, worse surgical outcome, and higher 30-day mortality. 1 A significantly increased risk of death has been seen in patients with advanced age, immune-compromised, respiratory failure, 2 and high Charlson Comorbidity Index. 1 Prompt diagnosis, systemic antifungal, drainage, and decortication can affect the survival of the patient. However, data is lacking on optimal duration of antifungals. Besides, the data are limited globally on fungal empyema, and mostly reported data are in the form of case reports. Therefore, we aimed to conduct a retrospective case series study to determine the etiology, clinical characteristics, treatment, and outcome of fungal empyema in our patient population.
Materials and methods
Study design and setting
This was a retrospective, observational study conducted on proven fungal empyema cases admitted at Aga Khan University Hospital (AKUH) Karachi, Pakistan from January 2018 to May 2021. Records of 26 patients with a diagnosis of fungal empyema were retrieved using the International Classification of Diseases 9 system from Health Information Management System of AKUH.
Inclusion and exclusion criteria
Patients with proven fungal empyema based on positive cultures of pleural fluid, pleural tissue, and/or histopathology were included regardless of underlying conditions; polymicrobial bacterial and fungal empyema was excluded.4,5 We excluded all those patients with polymicrobial bacterial and fungal empyema or with negative pleural fluid cultures.
Study questionnaire
A preformed questionnaire was filled out for each case. The questionnaire looked at the following factors: age, gender, smoking status, comorbid diseases, high-resolution computed tomography (HRCT) findings along with pleural effusion, clinical features, complications, microbiology, treatment options, and outcome.
Informed consent
Informed consent was waived due to this being a retrospective study with no human or animal experimentation. The study was approved by the ethical review committee at AKUH.
Fungal culture
During the study period, if pleural fluid and/or pleural tissue were sent for bacterial culture Sabouraud’s dextrose agar plate was inoculated and incubated aerobically in addition to the routine bacterial media. The plates were read daily for 72 h before finalization. Pleural fluid and/or pleural tissue specifically requested for fungal culture were inoculated on sheep blood agar, two plates of Sabouraud’s dextrose agar incubated at 37°C and 25°C, potato dextrose agar, and Mycosel agar. The plates were read daily for first week, then twice weekly for the next 3–4 weeks. Any fungal growth observed on the culture plates was identified using phenotypic methods. Candida species were identified by morphology on BiGGY, ChromAgar Candida, and Cornmeal Tween80 agar and analytical profile index-API 20AUX (BioMerieux). Molds were identified phenotypically by colony morphology and microscopic features as visualized on lactophenol cotton blue smears.
Antifungal susceptibility testing
Antifungal susceptibilities to fluconazole and voriconazole were performed for C. albicans, C. tropicalis, and C. parapsilosis and fluconazole for C. glabrata and voriconazole for Candida krusei by disc diffusion method according to Clinical Laboratory Standards Institute (CLSI) guidelines M44 3rd edition. Minimum inhibitory concentrations for fluconazole resistant strains were determined using Sensititre YeastONE YO10 and interpretation was done according to CLSI M60 1st edition and European Committee on Antimicrobial Susceptibility Testing 2020. C. parapsilosis ATCC 22019 and C. krusei ATCC 6258 were used as quality control strains.
Data management and statistical analysis
Data entry and management was conducted using Excel for Microsoft 365, while descriptive statistical analysis was performed using the Statistical Package for Social Sciences for Windows, version 19.0 (IBM Corp., Armonk, NY, USA). Demographic and clinical characteristics of the patients with fungal empyema were presented as mean and standard deviation (SD) for continuous variables and frequency and percentage for categorical variables. Descriptive characteristics of individual patients, which also included presenting complaints, HRCT features, video-assisted thoracoscopic surgery (VATS), anti-fungal treatment, fungal species, specific fungal organisms, respiratory failure outcome, and survival outcome, were also reported.
Results
Sociodemographic and clinical characteristics
The present case series comprised 26 patients with fungal empyema. The sociodemographic and clinical characteristics of the patients are shown in Table 1. Mean age of the patients was 43.6 ± 20.3 years. Male gender was predominant (n = 16, 61.5%). Diabetes mellitus (DM) was the most frequent comorbidity (n = 11, 42.3%), followed by hypertension (n = 9, 34.6%), malignancy (n = 6, 23.1%), and asthma (n = 1, 3.8%). Of the 26 patients, 10 (38.5%) had multiple comorbidities. The types of malignancy were esophageal cancer (three patients), followed by breast cancer (two patients) and lung cancer (one patient). Most commonly exhibited respiratory symptoms were shortness of breath (n = 17, 65.4%), cough (n = 13, 50.0%), and fever (n = 11, 42.3%). On HRCT examination, along with pleural effusion, cavitation (n = 8, 30.8%), consolidation (n = 8, 30.8%), and loculated effusion (n = 5, 19.2%) were the most frequent features.
Demographic and clinical characteristics of patients admitted with fungal empyema.

HRCT, high-resolution computed tomography; SD, standard deviation.
Fungal isolates and antifungal treatment
Candida spp. was the predominant isolated fungal pathogen (n = 21, 80.8%), followed by Aspergillus spp. (n = 7, 26.9%). Fusarium spp. was isolated from one (3.9%) patient. The details of isolated fungal pathogens are presented in Table 2. Twenty-one (80.8%) patients received anti-fungal therapy. Amphotericin B (n = 10, 47.6%) was the most frequently received anti-fungal treatment, followed by voriconazole (n = 6, 28.6%) and fluconazole (n = 6, 28.6%). Fourteen (53.8%) patients had VATS and tube thoracostomy was performed on 46.2% (n = 12) of the patients.
Fungal isolates from empyema.
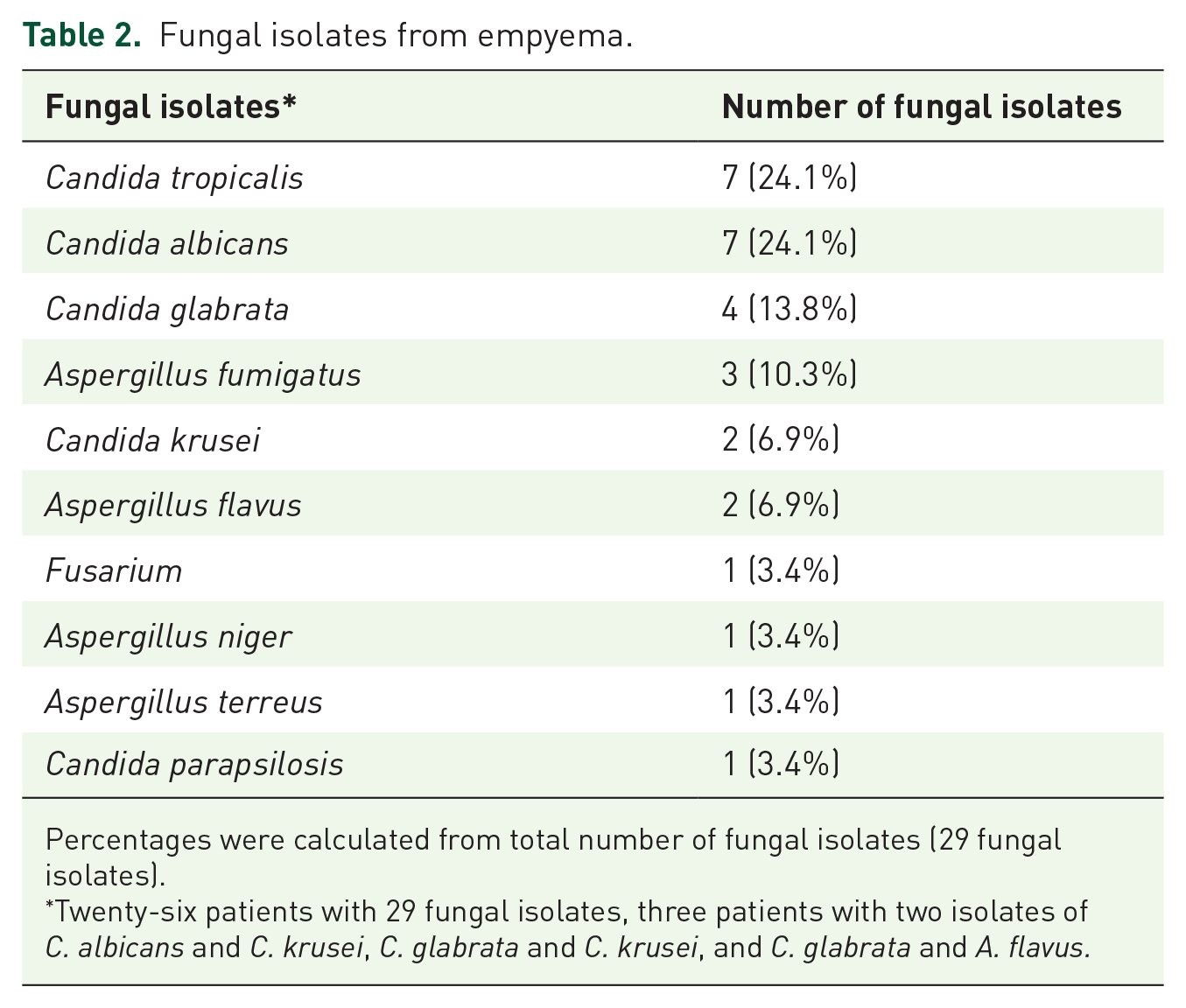
Percentages were calculated from total number of fungal isolates (29 fungal isolates).
Twenty-six patients with 29 fungal isolates, three patients with two isolates of C. albicans and C. krusei, C. glabrata and C. krusei, and C. glabrata and A. flavus.
Antifungal susceptibility
Antifungal susceptibilities were determined for 15 cases. All except one C. albicans, C. tropicalis, and C. parapsilosis strains were susceptible to fluconazole and voriconazole. One C. parapsilosis strain was resistant to fluconazole and voriconazole but was sensitive to amphotericin and caspofungin. C. krusei strains were susceptible to voriconazole, amphotericin, and caspofungin. C. glabrata strains were susceptible to fluconazole, amphotericin, and caspofungin.
Mortality
Overall, in-hospital mortality was 38.5% (n = 10), and all patients developed respiratory failure. Of the 21 patients who received antifungal treatment, 9 (42.9%) expired. Those patients who died, regardless of the treatment, had cultures positive for C. tropicalis (n = 1, 0.1%), C. albicans (n = 5, 0.5%), C. krusei (n = 2, 0.2%), C. glabrata (n = 4, 0.4%), and A. flavus (n = 1, 0.1%). Characteristics of individual patients diagnosed with fungal empyema are shown in Table 3.
Characteristics of individual patients diagnosed with fungal empyema.

DM, diabetes mellitus; HbA1C, hemoglobin A1C; HRCT, high-resolution computed tomography; HTN, hypertension; NA, not available; SOB, shortness of breath; VATS, video-assisted thoracoscopic surgery.
Discussion
This is the first case series from Pakistan that presents the etiology, clinical features, and outcome of fungal empyema. We have reported 26 proven fungal empyema cases with Candida spp. as the most frequent organism, followed by Aspergillus spp. We found that fungal empyema was seen in mainly male, diabetic, hypertensive patients. Among malignancies, gastrointestinal (esophageal cancer) and breast cancer were more common. All patients in our study, regardless of their treatment, died due to respiratory failure.
These results are consistent with a study published from Taiwan, where fungal empyema was predominant in males and Candida spp. was the commonest organism (47 isolates, 64%), with increased relative risk of death (73%) with respiratory failure and immunocompromised state. 2 Candida spp. is a normal flora of the gut and urinary tract. Case reports have shown the risk of Candida spp. empyema increases in gastrointestinal malignancy such as esophageal cancer, esophageal fistula, and perforation.6–8 We found cancer in 23.1% of patients, not only gastrointestinal esophageal malignancy but also breast cancer. Candida spp. was the commonest pathogen in our patients (73.1%) and also reported previously as a common pathogen of fungal empyema 89% and 64%, respectively.1,2
DM is an important risk factor for fungal infections of various organs, from colonization to invasive infection. 9 DM incidence is currently rising globally, but rampantly affecting low- and middle-income countries like Pakistan. 10 In total, we found that 38.5% of our patients had DMs, which is higher than previously reported data from the United States 3 (22%) and Taiwan (25.4%). 11 We found DM was a possible risk factor for fungal empyema, which must be investigated further in larger cohorts or case control studies. Overall, fungal infections are underdiagnosed in Pakistan due to poor or lack of diagnostic facilities, but the reported incidence of invasive candidemia and mucormycosis are currently rising. 12
Mortality was seen in 38.5% of patients, which included C. albicans 55.5% and C. glabrata 33.3%. This is comparable to previously reported data at 52% with C. albicans and 30% with C. glabrata from the United States. 3 C. albicans (n = 4) was also found to be a common cause of fungal empyema in a case series of eight patients from Taiwan and overall in hospital mortality reported was 62.5%. 13 In another study from Taiwan, the mortality rate was 61.9% with C. albicans being the commonest pathogen (76.5%). 11 We found a decreased mortality rate compared to these studies, which might be due to intervention such as VATS decortication performed in 53.8% and antifungal use in 80.8% of patients.
Most of our patients received amphotericin B followed by fluconazole and voriconazole compared to those of Cheng et al. 1 where fluconazole and voriconazole were frequently prescribed and those of Lin et al. 11 where fluconazole was used in majority of patients. Data suggest that in fungal empyema, surgical intervention is associated with worse outcome compared to bacterial empyema. 1 Intrapleural fibrinolytics therapy in bacterial empyema has been investigated in various studies. However, the results are variable and a Cochrane database review concluded no mortality benefit with intrapleural fibrinolytics. 14 Overall, prompt diagnosis, systemic antifungal, drainage, and decortication can affect the survival of the patient. However, data is lacking on the optimal duration of antifungals and overall fungal empyema management.
This study has some limitations. For example it is a single center study with a small sample size. We do not have molecular diagnostic facilities and therefore we did not confirm the results on a molecular level. However, we did perform fungal cultures in every patient using special fungal culture media. A lack of diagnostic facilities can delay diagnosis and impact the overall outcome of the patient. Further studies with better diagnostic capabilities, larger sample sizes, and multicenter involvement will help to understand fungal empyema in more detail.
Conclusion
Our data suggest fungal empyema is not uncommon and necessitates a high index of suspicion, to prevent a delay in diagnosis, treatment, and improve outcome. We found DM as a possible risk factor for fungal empyema, which must be investigated in larger cohorts or case control studies. We found that the most common species were Candida followed by Aspergillus and the mortality rate was high with respiratory failure.
Supplemental Material
sj-doc-1-tai-10.1177_20499361231223887 – Supplemental material for Fungal empyema thoracis, a rare but an emerging entity: a retrospective case series from Pakistan
Supplemental material, sj-doc-1-tai-10.1177_20499361231223887 for Fungal empyema thoracis, a rare but an emerging entity: a retrospective case series from Pakistan by Nousheen Iqbal, Akbar Shoukat Ali, Aqusa Zahid, Kausar Jabeen and Muhammad Irfan in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-pdf-1-tai-10.1177_20499361231223887 – Supplemental material for Fungal empyema thoracis, a rare but an emerging entity: a retrospective case series from Pakistan
Supplemental material, sj-pdf-1-tai-10.1177_20499361231223887 for Fungal empyema thoracis, a rare but an emerging entity: a retrospective case series from Pakistan by Nousheen Iqbal, Akbar Shoukat Ali, Aqusa Zahid, Kausar Jabeen and Muhammad Irfan in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.