
Abstract
Background:
Data are controversial regarding nephrotoxicity risk with vancomycin plus piperacillin–tazobactam (VPT) compared to vancomycin alone or in combination with other beta-lactams (BLs) in acute care use. Furthermore, data are lacking on the incidence of acute kidney injury (AKI) with long-term use of VPT including outpatient parenteral antimicrobial therapy (OPAT).
Methods:
This retrospective study included 826 adult patients on an intravenous vancomycin plus BL for ⩾2 weeks, including cefepime, piperacillin/tazobactam, ertapenem, or meropenem, from August 2017 to January 2022. The primary outcome was incidence of AKI. Univariate and multivariable Cox proportional hazard regression analyses were conducted to adjust for confounding variables. A secondary analysis based on the propensity score (PS)-matched cohort was performed.
Results:
AKI occurred in 14.4% of patients in the VPT group (n = 15/104) compared to 5.5% in the other BL group (n = 40/722) (p < 0.001). Average time to AKI from start of combination therapy was 9.4 (1.7–12.0) days in the VPT group and 10.9 (5–22.7) days in the other BL group (p = 0.20). The median duration of vancomycin and BL in the overall cohort was approximately 1 month. Beyond BL selection, patient characteristics were not associated with AKI other than the receipt of concomitant acyclovir [hazard ratio (HR) 2.48 (95% confidence interval (CI): 1.33–4.65), p = 0.004]. In the PS-matched cohort, AKI occurred in 14.4% of patients in the VPT group (n = 15/104) and 5.3% in the other BL group (n = 11/208) (p = 0.006). Receipt of VPT [HR: 2.55 (1.36–4.78), p = 0.004] and acyclovir [HR: 2.38 (1.19–4.74), p = 0.014) remained significantly associated with AKI in the multivariable model.
Conclusion:
Clinicians should exercise caution when using VPT for >2 weeks, including in the OPAT setting, even when no renal dysfunction is observed during the initial week of combination therapy.
Introduction
Outpatient parenteral antimicrobial therapy (OPAT) provides many benefits to patients including shorter hospital length of stay, decreased cost, and increased patient satisfaction.1–3 Routine laboratory monitoring is recommended for OPAT patients and has been shown to reduce the rate of hospital readmission. 4 The use of nephrotoxic agents such as vancomycin in the OPAT setting poses additional safety concerns owing to variability in hydration status and less frequent laboratory monitoring compared to the inpatient setting.
Nephrotoxicity is a known adverse drug reaction associated with vancomycin use. 5 Risk factors include total daily dose of vancomycin exceeding 4 g daily, duration of therapy greater than 7 days, trough levels >15 μ/mL or area under the curve (AUC) >600, concomitant administration with other nephrotoxic agents, obesity, preexisting renal dysfunction, diabetes, and hypertension. Patients with multiple risk factors experience increased risk of vancomycin nephrotoxicity, with the onset typically occurring between 5 and 7 days.5,6
Concomitant use of piperacillin/tazobactam (PTZ) has also been implicated as a risk factor for vancomycin-induced nephrotoxicity.7–17 Vancomycin plus piperacillin/tazobactam (VPT) has been associated with an increased risk of acute kidney injury (AKI) compared to vancomycin plus an alternative antipseudomonal beta-lactam (BL) such as cefepime or meropenem.12–20 AKI has been shown to occur faster with VPT compared to vancomycin alone or vancomycin plus cefepime or meropenem.12,16,21 In contrast, other studies have not found an increased rate of AKI with VPT compared to vancomycin plus cefepime or meropenem in critically ill populations after adjustment for relevant confounders.22,23
While most data focus on short-term use (i.e. <7 days), data are lacking on the AKI incidence of vancomycin with BLs including PTZ in long-term use (i.e. ⩾2 weeks) including OPAT. Previous studies have evaluated the onset of AKI with various combinations of vancomycin and BLs, but it remains unclear whether patients can tolerate these combinations longer term if no AKI is observed in the first week of therapy, or if there is a time-dependent cumulative renal risk.
Renal injury has been linked to increased morbidity including chronic kidney disease (CKD), cardiovascular events, and decrease in 5- to 10-year survival. 24 Therefore, it is important to evaluate for incidence and risks for AKI in the setting of long-term use of combination of vancomycin and BLs. The purpose of this study is to determine the relative renal risk of combination of BLs with vancomycin in the setting of longer durations of therapy, including patients receiving OPAT.
Methods
Study design and population
This was a retrospective cohort study evaluating the safety of intravenous (IV) BL with IV vancomycin combinations in long-term use across the Mayo Clinic Enterprise including sites in Arizona, Florida, Minnesota, and Wisconsin. Hospitals ranged in size from critical access hospitals (approximately 10–20 beds) with transitional care units and generally no formal OPAT team to a large academic medical center (>1000 beds) with multidisciplinary dedicated OPAT teams. The institution-wide guidance for antimicrobial laboratory monitoring recommends once weekly serum creatinine (SCr) monitoring for cephalosporins, penicillin, and carbapenems. Vancomycin monitoring recommendation is SCr and vancomycin trough once weekly with a target trough of 10–15 µ/mL unless the treatment indication was methicillin-resistant Staphylococcus aureus (MRSA) pneumonia, central nervous system infection (15–20 µ/mL), or MRSA bloodstream infection (10–20 µ/mL). Twice weekly, SCr and vancomycin trough monitoring is advised for select high-risk patients (trough goal 15–20 µ/mL, >4 g/day of vancomycin, unstable renal function, etc.). Ultimately, the laboratory monitoring plan was at the discretion of the treating clinician(s). Eligible patients were ⩾18 years of age and received IV cefepime, PTZ, ertapenem, or meropenem plus IV vancomycin for ⩾2 weeks from 25 August 2017 to 13 January 2022. Cefepime, ertapenem, and meropenem were chosen as the comparator BLs of interest due to their similar spectrums of activity to PTZ and frequency of use for long-term IV antibiotic therapy at our institution. To be assigned to a BL group, the patient needed to receive >50% of their total treatment duration with that BL. Patients who were incarcerated, pregnant, or Minnesota residents who declined Minnesota research authorization were excluded. Additional exclusion criteria included AKI within 7 days of BL or vancomycin use, ⩾6 BL switches throughout the course of BL therapy, receipt of renal replacement therapy, and chronic renal dysfunction (⩾Stage 3 CKD per past medical history or any creatinine clearance <30 mL/min based on Cockcroft–Gault). The Mayo Clinic Institutional Review Board deemed this study to be exempt.
Outcomes and definitions
The primary outcome was incidence of AKI, defined as an increase in SCr ⩾ 2 times higher than the baseline value, which was similarly defined in a retrospective cohort study conducted by Moenster et al. 25 Baseline SCr was calculated as the average of SCr in the 6 months preceding the index date. Time to AKI was evaluated as a secondary outcome. Concomitant nephrotoxins included any documented receipt of oral or IV computed tomography (CT) contrast, nonsteroidal anti-inflammatory drugs (NSAIDs) (ibuprofen >600 mg/24 h, naproxen >440 mg/24 h, ⩾1 dose of ketorolac), acyclovir, amphotericin B, IV aminoglycosides, and any non-chronic diuretic use.
Statistical analysis
Comparisons of patient characteristics between groups were made using t-tests or Wilcoxon rank-sum tests for continuous variables and either chi-square or Fisher’s exact test for categorial variables. The primary outcome was compared between groups with chi-square test. We additionally utilized univariate and multivariable Cox proportional hazard regression analyses to assess risk factors for AKI including vancomycin dose exceeding 4 g daily, obesity, and concomitant nephrotoxins. Among patients with observed AKI, time to AKI was compared using a Wilcoxon rank-sum test. For the time-dependent covariate analysis, there is a lag of 48 h, which assumes that the effect of the BL starts at 48 h after the first dose and continues for 48 h after stopping.
To account for potential differences between treatment groups, we also ran a secondary analysis based on a propensity score (PS)-matched cohort. PS was defined as the probability that a patient would receive VPT and was estimated using a multivariable logistic regression model with the characteristics in Table 1 as the covariates. Patients with VPT were then matched 1:2 to those with another BL based on the logit of the PS (±0.2 standard deviation of the logit of the PS). Covariate imbalance between groups was evaluated using standardized differences, where a standardized difference <0.10 represents negligible imbalance between groups.
Baseline characteristics.

Available in 102 piperacillin–tazobactam patients and 702 other beta-lactam patients who received some treatment inpatient.
Available in 58 piperacillin–tazobactam patients and 492 other beta-lactam patients who receive some treatment outpatient.
IQR, interquartile range; mg, milligrams; SCr, serum creatinine; SD, standard deviation.
All tests were two-sided, and p values less than or equal to 0.05 were considered statistically significant. All analyses were performed using SAS version 9.4 software (SAS Institute, Inc., Cary, NC, USA).
Results
A total of 826 met inclusion criteria for analysis, of whom 104 patients were categorized in the VPT group and 722 patients were categorized in the other BL group (Figure 1). The mean age of patients was 60.9 years with a total of 471 patients being male (57.0%) and total of 721 patients being Caucasian (87.3%) (Table 1). Over half of the patients received antimicrobials in the outpatient setting for at least one dose, with a minority receiving antimicrobials exclusively as outpatients. Concomitant nephrotoxins were common, including CT contrast (42.5%), NSAIDs (44.8%), and receipt of at least one IV aminoglycoside dose (21.8%).
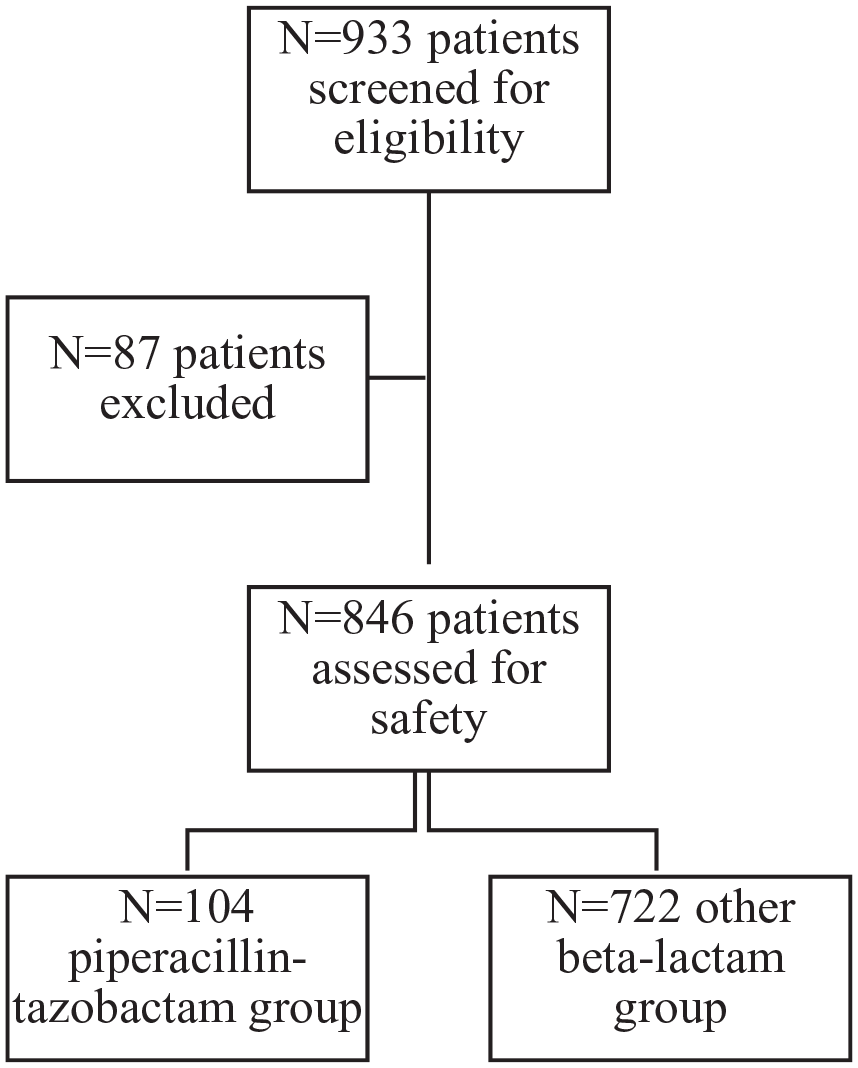
Total patients included for analysis in VPT group and other-BL group.
Patients in the VPT group were younger on average (57.5 years versus 61.4 years, p = 0.008) and had a lower median weight (78.6 versus 84.8 kg, p = 0.028) compared to the other BL group. Receipt of CT contrast was more common in the VPT group (57.7%) versus the other BL group (40.3%) (p < 0.001). The median vancomycin duration was 29.9 days in the total cohort (25.5 days VPT versus 31.2 days other BL, p = 0.098) and the median duration of BLs was 31 days overall (23.1 days PTZ versus 32.9 days other BL, p = 0.014). The total daily dose of vancomycin on average was 1729 mg (1722 mg VPT versus 1729 other BL, p = 0.66). A BL duration of 2 to <3 weeks was more common in the VPT group (n = 47/104, 45.2%) compared to the other BL group (n = 203/722, 28.1%).
AKI was observed in 6.7% of total patients (n = 55/826), occurring in 14.4% of patients in the VPT group (n = 15/104) as compared to 5.5% in the other BL group (n = 40/722) (p < 0.001) (Table 2). There was no significant association seen between AKI and body mass index, Charlson Comorbidity Index, baseline SCr, and nephrotoxin exposure, with the exception of acyclovir. In patients who received concomitant acyclovir, 14.5% developed AKI (n = 10/69), while 5.9% (n = 45/757) of those without exposure to acyclovir developed AKI [HR: 2.88 (95% confidence interval (CI): 1.41–5.57), p = 0.003]. Receipt of VPT [HR: 2.55 (1.36–4.78), p = 0.004] and acyclovir [HR 2.38 (1.19–4.74), p = 0.014] remained significantly associated with AKI in the multivariable model. Among those with AKI, the average time to AKI was 9.4 (IQR 1.7–12.0) days in the VPT group and 10.9 (IQR 5–22.7) days in the other BL group (p = 0.20) from the combination therapy start. The majority of renal injury (n = 47/55) occurred while inpatient.
Univariate associations between patient and clinical characteristics and AKI.
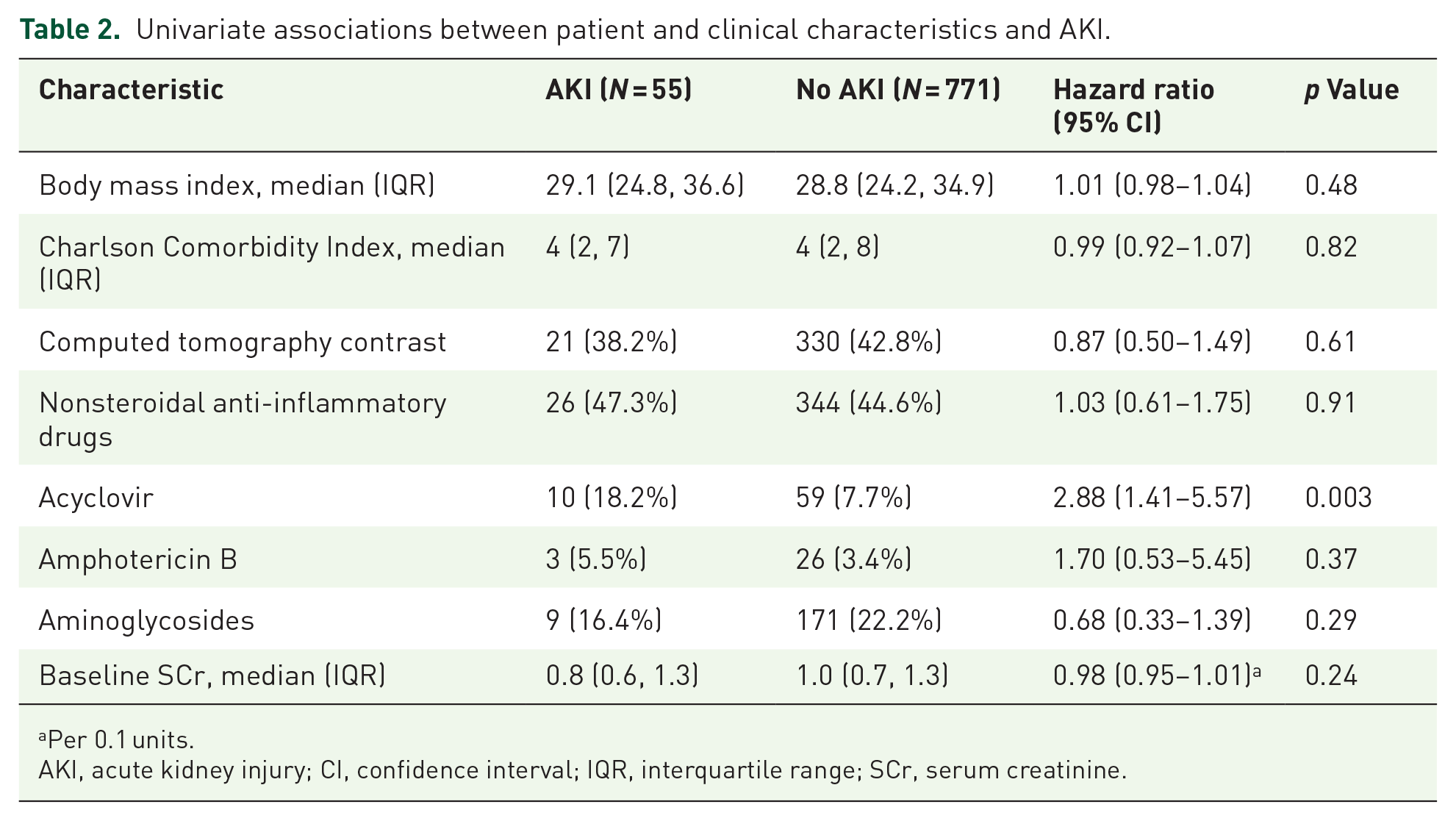
Per 0.1 units.
AKI, acute kidney injury; CI, confidence interval; IQR, interquartile range; SCr, serum creatinine.
In the PS-matched cohort, there were 104 patients in the VPT arm matched to 208 in the other BL arm. These groups were well balanced in terms of baseline characteristics (Table 3). AKI occurred in 14.4% of patients in the VPT group (n = 15/104) and 5.3% in the other BL group (n = 11/208) (p = 0.006). When treating PTZ as a time-dependent covariate where the potential nephrotoxicity of VPT did not take effect until 48 h after PTZ start, and the effect remained up to 48 h after stopping PTZ, we found those receiving VPT were still more likely to have AKI [HR: 3.17 (1.27–7.96), p = 0.014] (Table 4).
Propensity score-matched baseline characteristics.

A standardized difference <0.10 represents negligible imbalance between groups.
IQR, interquartile range; SD, standard deviation; SCr, serum creatinine.
Univariate associations between patient and clinical characteristics and AKI in the propensity score-matched cohort.

Per 10 units.
Per 0.1 units.
For the time-dependent covariates, there is a lag of 48 h, which assumes that the effect of the beta-lactam does not ‘kick in’ until 48 h after starting, and continues for 48 h after stopping.
AKI, acute kidney injury; CI, confidence interval; IQR, interquartile range; SCr, serum creatinine; SD, standard deviation.
Discussion
To our knowledge, this is the first study to assess the safety of long-term use of vancomycin plus BLs, including patients receiving antimicrobials in the OPAT setting. We observed a statistically higher rate of AKI occurrence with VPT compared to other BLs used in combination with vancomycin for >2 weeks. Concomitant use of PTZ and acyclovir with vancomycin was both significantly associated with AKI. Our findings are consistent with previous studies demonstrating higher rates of AKI with VPT as compared to vancomycin alone or vancomycin plus other BLs with short-term use.7–20
The mechanism by which VPT increases AKI risk has not been clearly defined. Increased rates of nephrotoxicity have been seen with anti-staphylococcal penicillin compared to cefazolin when combined with vancomycin for MRSA bacteremia. 26 In addition, an increased rate of AKI has been noted with VPT compared to vancomycin plus ceftolozane/tazobactam. 27 These findings implicate the piperacillin rather than the tazobactam component. Piperacillin has high affinity for organic anion transporter-3, leading to intracellular accumulation in the proximal renal tubule. 28 This may further exacerbate oxidative stress caused by vancomycin in renal tubular epithelial cells. 29
We defined AKI as an increase in SCr ⩾ 2 times higher than the baseline value. Increases in SCr may be due to competitive inhibition of renal tubular secretion of creatinine and transporter suppression rather than representative of true renal injury. 30 A recent study by Miano et al. 30 found that VPT was associated with a higher incidence creatinine-defined AKI as compared to vancomycin plus cefepime but did not result in significant changes in cystatin C, a biomarker unaffected by tubular secretion. Pending emerging evidence continues to support these findings, OPAT programs may consider cystatin C monitoring (either routinely or case by case at the time of SCr increase) for VPT. Based on our findings, cystatin C monitoring in OPAT does not seem strongly indicated for other BL combinations.
Our study has several additional limitations, including its retrospective study design. We were unable to evaluate urine output because many subjects were partially managed in the outpatient setting. Serum trough monitoring was used for vancomycin dosing in our cohort with a target trough of 10–15 for most indications; however, this has not been shown to significantly impact the risk of AKI compared to area under the concentration–time curve vancomycin dosing in the setting of VPT therapy. 31 We did not evaluate all potential adverse effects associated with these antimicrobial regimens, which may have led to changing antimicrobial therapy independent of AKI. Actual use of concomitant nephrotoxins may have varied from what was documented in the electronic medical record, particularly for outpatients. Patient with observed AKI may have been more likely to have concomitant nephrotoxin use documented as a consequence of clinical evaluation and management of their AKI. For the time-dependent covariates analysis, we attributed AKI to a specific BL combination if it occurred after 48 h of the first dose of BL and within 48 h of the last BL dose, this window was based on BL pharmacokinetics and expert opinion. In addition, 87% of the patients in this cohort are Caucasian; therefore, the external validity of this study to other races is not clear.
Over half of the study cohort received BL and vancomycin combination for part or the entire course as an outpatient, with a majority crossing both settings. This study findings are particularly salient for OPAT practitioners given the potential implications of AKI for hospital readmissions and resource-intensive changes in OPAT regimen, in addition to general patient safety concerns. Importantly, the majority of AKI occurred in the inpatient setting; however, 14.5% of AKI occurred during OPAT. Renal risk mitigation for OPAT programs to these findings could take a number of forms including the following: (1) Choice of a PTZ alternative when vancomycin is also indicated, where possible; (2) Use of daptomycin, linezolid, or other broad gram-positive agent in place of vancomycin when PTZ is also indicated, where possible; (3) Pre-emptive increased intensity of renal monitoring for those receiving VPT (i.e. monitoring SCr twice weekly instead of once weekly, monitoring cystatin C when available, avoiding other nephrotoxic medications); and (4) Limiting VPT to 2 weeks with a planned IV to oral switch therapy to oral agents also termed ‘IVOST’. 32 We also found it important that AKI appeared at an average of around 10 days; thus, our evidence suggests that renal risk with BL combinations is not cumulative with time, as may be a common misconception.
Other areas needing future exploration which may have influence on renal outcomes include the use of continuous infusions of vancomycin and/or PTZ, vancomycin AUC monitoring in the outpatient setting, and as previously mentioned, routine cystatin C monitoring with long-term use of combination vancomycin with PTZ.
Conclusion
Even when no renal dysfunction is observed during the initial week of combination therapy, clinicians should proceed with caution and consider increased laboratory monitoring frequency when using longer courses of VPT.