
Abstract
Purpose:
To determine the frequency at which fluoroquinolones and aminoglycosides demonstrate in vitro activity against non-urinary, non-skin/skin structure Pseudomonas aeruginosa isolates exhibiting decreased susceptibilities to one or more β-lactam agents.
Methods:
β-lactam-non-susceptible P. aeruginosa isolates recovered from blood, bone, lower respiratory tract, pleural fluid, cerebrospinal fluid, or peritoneal fluid cultures between October 2010 and October 2014 were reviewed from four community hospitals within a single health-system. Only the first isolate per patient was included for analysis. The likelihood that each isolate was susceptible to a non-β-lactam antimicrobial was then determined and summarized within a combination antibiogram.
Results:
In total, 179 P. aeruginosa isolates with decreased susceptibilities to one or more β-lactam agents were assessed. Because no appreciable differences in antimicrobial susceptibility profile were observed between hospitals, the isolates were evaluated in aggregate. Susceptibility rates for β-lactam monotherapy ranged from 34% to 75%. Aminoglycosides possessed increased antibacterial activity compared to fluoroquinolones. Tobramycin was the non-β-lactam most likely to expand antimicrobial coverage against β-lactam-non-susceptible P. aeruginosa with activity against 64%, 66%, and 65% of cefepime-, piperacillin-tazobactam-, and meropenem-non-susceptible isolates, respectively (p < 0.001 for all).
Conclusions:
The results of this study support the use of aminoglycosides over fluoroquinolones for achieving optimal, empiric antimicrobial combination therapy for P. aeruginosa when dual antimicrobial therapy is clinically necessary. Future efforts aimed at optimizing combination therapy for P. aeruginosa should focus on systemic interventions that limit the selection of fluoroquinolones in combination with β-lactams to expand coverage based on local susceptibility rates.
Introduction
Pseudomonas aeruginosa is an aerobic, Gram-negative bacillus commonly implicated in severe infections. Patients who acquire infections due to multi-drug resistant (MDR) P. aeruginosa are at an increased risk of treatment failure and mortality.1,2 Prescribers often select antimicrobial combination therapies to increase bactericidal activity through synergy, decrease the emergence of bacterial resistance, and ensure appropriate empiric coverage.3–5 However, of these proposed benefits, combination therapy was only shown to increase the likelihood of appropriate empiric coverage in clinical practice.6,7 Therefore, the benefits of combination therapy must be weighed against the consequences of increased antimicrobial consumption such as increased adverse events, medication costs, Clostridium difficile diarrhea, and emergence of resistance.8–11
Despite controversy surrounding its routine use, the reported percentage of patients receiving combination therapy for suspected P. aeruginosa infections and/or critical illness remains high.6,12,13 Combination therapy typically includes a β-lactam with activity against P. aeruginosa and a fluoroquinolone or an aminoglycoside with activity against P. aeruginosa (anti-pseudomonal). Prescribers wishing to avoid the risk of nephrotoxicity and need for therapeutic drug monitoring may elect to use an anti-pseudomonal fluoroquinolone, rather than an aminoglycoside, in combination with an anti-pseudomonal β-lactam. Local antimicrobial susceptibility data, often in the form of an antibiogram, have been utilized to select combination regimens; commonly by selecting two antimicrobials showing the greatest individual in vitro activity against P. aeruginosa. 14 Yet, traditional antibiograms are unable to account for overlapping antimicrobial resistance mechanisms. Due to this limitation, combination antibiograms quantifying the likelihood that at least one antimicrobial is active may be utilized to inform empiric prescribing at a local level.
Available literature on P. aeruginosa combination antibiograms suggests the additional coverage conferred by a fluoroquinolone is less than that of an aminoglycoside.14–17 However, the majority of previous evaluations were conducted in the context of single-center large urban teaching hospitals, and all but one included isolates from all body sites, including urine. This is notable as the bacterial ecology at smaller hospitals may differ from large tertiary referral centers due to lack of specialized clinical service lines and/or potentially different antimicrobial prescribing practices. In 2013, 37.2% of US hospital discharges were from urban, non-teaching hospitals. 18 Additionally, treatment of P. aeruginosa in the urinary tract is less pharmacokinetically challenging and urinary isolates may possess different susceptibility patterns than non-urinary isolates. Furthermore, skin/skin structure isolates may reflect colonization rather than true infection while also possessing different susceptibility patterns than isolates from non-skin/skin structure sites. The objective of this study was to determine the frequency at which fluoroquinolones and aminoglycosides demonstrate in vitro activity against non-urinary, non-skin/skin structure P. aeruginosa isolates exhibiting decreased susceptibility patterns to one or more β-lactam agents from a non-referral health-system.
Methods
Data were collected for inpatients aged ⩾18 years from one of four community hospitals (licensed for 100–385 beds) within Wheaton Franciscan Healthcare of Southeast Wisconsin from 1 October 2010 through 31 October 2014. A line listing of all P. aeruginosa isolates recovered from blood, bone, lower respiratory tract, pleural fluid, cerebrospinal fluid, or peritoneal fluid cultures was procured by a laboratory information system. Organism identifications were generated by automated VITEK® 2-based Gram-negative identification (GN) cards (bioMérieux, Incorporated, Hazelwood, MO) or, when appropriate, by rapid identification schema outlined in CLSI M35-A2. 19 Performance and interpretation of routine ceftazidime, cefepime, aztreonam, piperacillin-tazobactam, meropenem, imipenem-cilastatin, ciprofloxacin, levofloxacin, gentamicin, and tobramycin disk diffusion susceptibility testing followed guidelines in the CLSI M100 series. 20 Upon clinician request, amikacin disk diffusion susceptibility testing was also procured. Isolates from patients aged <18 years and those from the urinary tract or skin/skin structure were excluded.
P. aeruginosa isolates with decreased susceptibility (intermediate or resistant) to at least one anti-pseudomonal β-lactam (piperacillin-tazobactam, cefepime, ceftazidime, meropenem, imipenem-cilastatin, doripenem, and/or aztreonam) were subsequently compiled. Data from all four hospitals were analyzed in aggregate as substantial homogeneity with respect to antimicrobial susceptibility profiles was observed between sites (data not shown). Data were then audited for the anti-pseudomonal agents ciprofloxacin, levofloxacin, gentamicin, tobramycin, and amikacin. A limited number of isolates tested against amikacin precluded inclusion in the combination antibiogram.
The proportion of isolates susceptible to each β-lactam/non-β-lactam combination was compared to β-lactam monotherapy using Pearson’s chi-squared test for independence. A p-value of ⩽0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 20.0 (IBM Corp., Armonk, NY, USA). Per Wheaton Franciscan Healthcare Institutional Review Board policy, Institutional Review Board review was not required.
Results
A total of 179 P. aeruginosa isolates showing decreased susceptibility to at least one anti-pseudomonal β-lactam and meeting inclusion criteria were reviewed during the study period. Combined data showed 44 (25%), 81 (45%), 119 (66%), 57 (32%), 61 (34%), and 47 (26%) isolates with decreased susceptibility to ceftazidime, cefepime, aztreonam, piperacillin-tazobactam, meropenem, and imipenem-cilastatin; respectively.
A combination antibiogram displaying the coverage of commonly utilized β-lactams with aminoglycosides and fluoroquinolones revealed that aminoglycosides provided the highest additional in vitro activity, with tobramycin conferring greater additional coverage than gentamicin (Table 1). Tobramycin expanded the overall empiric coverage by 19–51% (p ⩽ 0.039 for all), and tobramycin-containing regimens were active against ⩾84% of isolates. Addition of a fluoroquinolone to a β-lactam conferred less empiric coverage as compared to aminoglycosides (Table 1), with ciprofloxacin providing marginally higher coverage than levofloxacin against all but the imipenem-non-susceptible (NS) isolates (p ⩾ 0.196 for all). All non-β-lactam agents in combination with aztreonam led to a substantial increase in antimicrobial coverage (p < 0.001 for all). Amikacin was active against the following percentages of β-lactam-NS P. aeruginosa isolates: 100% of ceftazidime-NS (n = 7), 67% of cefepime-NS (n = 12), 71% of aztreonam-NS (n = 14), 73% of piperacillin-tazobactam-NS (n = 11), 64% of meropenem-NS (n = 11), and 100% of imipenem-cilastatin-NS (n = 3).
Percentage of P. aeruginosa isolates with decreased susceptibility to one or more β-lactam agents (n = 179) exhibiting susceptibility to β-lactam monotherapy, as compared to combination therapy with non-β-lactam agents. a
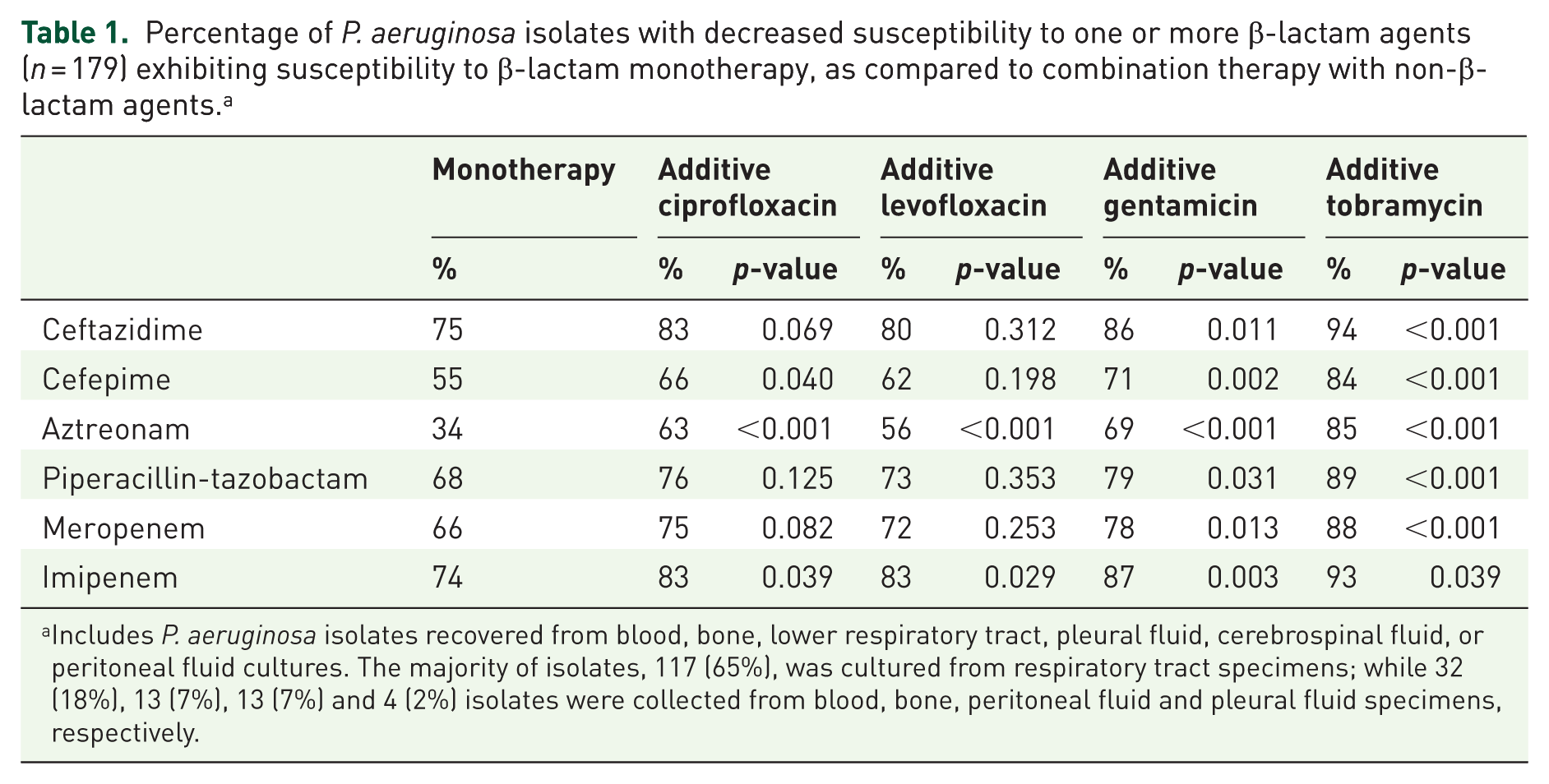
Includes P. aeruginosa isolates recovered from blood, bone, lower respiratory tract, pleural fluid, cerebrospinal fluid, or peritoneal fluid cultures. The majority of isolates, 117 (65%), was cultured from respiratory tract specimens; while 32 (18%), 13 (7%), 13 (7%) and 4 (2%) isolates were collected from blood, bone, peritoneal fluid and pleural fluid specimens, respectively.
Discussion
Results herein demonstrate that the additional coverage from ciprofloxacin or levofloxacin against non-urinary, non-skin/skin structure β-lactam NS P. aeruginosa isolates was less than that of gentamicin and tobramycin. Ciprofloxacin conferred slightly greater additional coverage than levofloxacin, while tobramycin conferred greater additional coverage than gentamicin. Finally, the β-lactam providing the broadest empiric coverage for P. aeruginosa isolates already exhibiting reduced susceptibility to at least one anti-pseudomonal β-lactam was ceftazidime.
Our findings are similar to those previously reported; however, our inclusion of P. aeruginosa isolates with reduced susceptibility to at least one β-lactam from four hospitals recovered from blood, bone, lower respiratory tract, pleural fluid, cerebrospinal fluid, or peritoneal fluid is notable. A combination antibiogram using P. aeruginosa isolates over 5 years recovered from urine, blood, and other sites at a single institution found β-lactam/aminoglycoside combinations most efficacious. 14 Christoff et al. noted the percentage of P. aeruginosa isolates covered by imipenem-cilastatin, ceftazidime, and piperacillin/tazobactam significantly rose following the addition of ciprofloxacin (66.2–75.7%, 70.3–82% and 74.7–82.1%, respectively). However, coverage rates were further increased with gentamicin and tobramycin in combination with the aforementioned β-lactam agents (82.3–93.2%). Additionally, there was no significant increase in coverage when ciprofloxacin was added to ceftazidime or piperacillin/tazobactam for bloodstream infections. 15 Thurman et al. assessed combining fluoroquinolones or aminoglycosides with β-lactams in a retrospective single site study. 17 For P. aeruginosa isolates resistant to a β-lactam, amikacin, tobramycin, and fluoroquinolones were active against 87–92%, 71–78% and 29–43% of isolates, respectively. 16 Smith et al., 17 constructed a combination antibiogram based on P. aeruginosa bloodstream isolates to aid in empiric anti-pseudomonal combination therapy for an oncology population at a single institution. Effective combination was defined as one providing empiric coverage against ⩾85% isolates, and the addition of the non-β-lactam antimicrobial increased the coverage by at least 5%. No combination of a β-lactam with ciprofloxacin met the definition of effective combination, while every combination with amikacin or tobramycin did. Other fluoroquinolones, including levofloxacin, were not described. Lastly, our findings are consistent with the trends in a recent review of P. aeruginosa isolates collected over 4 years (2012–2015) from US medical centers. 21
While several benefits have been explored with the use of combination therapy, ensuring appropriate empiric coverage appears to be the most compelling indication. Our findings add to the growing body of evidence supporting the selection of an aminoglycoside over an anti-pseudomonal fluoroquinolone for ‘double-coverage’ in the context of β-lactam resistance. The current study is unique as it presents data from multiple community, non-teaching hospitals, and only includes β-lactam NS P. aeruginosa isolates recovered from blood, bone, lower respiratory tract, pleural fluid, cerebrospinal fluid, or peritoneal fluid cultures. Including only β-lactam NS isolates presents prescribers with a more realistic appreciation for how fluoroquinolones and aminoglycosides perform in the setting of β-lactam resistance. Lastly, previous studies have used combinations of VITEK® 2, MicroScan®, and Etest for P. aeruginosa susceptibility testing.14,15,17 Concerns regarding the reliability of automated susceptibility testing have been previously described for P. aeruginosa.22,23 In the current study, disk diffusion was exclusively used for all P. aeruginosa susceptibility testing.
The consistent observation in our study, and others, of overlapping-resistance between fluoroquinolones and β-lactams may be explained by the ability of P. aeruginosa to express efflux pumps of the resistance-nodulation division (RND) family. RND efflux pumps usually consist of three proteins forming a complex allowing for the removal of antimicrobials causing sub-therapeutic concentrations at the site of action. Specifically, the MexAB-OprM, MexCD-OprJ, and MexXY possess cross-affinity for certain β-lactams and fluoroquinolones.24,25 While some RND pumps likely have affinity for aminoglycosides, the primary mechanism for aminoglycoside resistance is the production of inactivating enzymes such as acetyltransferases, phosphotransferases, and nucleotidyltransferases, which are not known to confer resistance to β-lactams and rarely confer low-level resistance to fluoroquinolones.26,27
There are several limitations associated with our findings. The retrospective, non-controlled design limits the generalizability of these results. Also, the lack of amikacin susceptibility data for the majority of isolates limits a reliable comparison to other antimicrobials tested. This study only examined in vitro susceptibility data, and clinical outcomes with combination or monotherapy were not evaluated. Lastly, no clear consensus defining optimal empiric coverage is currently available. Smith et al. 17 defined a threshold of 85% as the minimal effective empiric coverage rate, while the most recent guidelines for the management of hospital-acquired and ventilator-associated pneumonia suggest empiric antimicrobial regimens targeting P. aeruginosa should assure ⩾95% of patients receive active empiric therapy in units where >10% of Gram-negative isolates are resistant to an agent being considered for monotherapy. 28 While laudable, the 95% threshold may be unattainable when considering current and previously published studies describing combination antibiograms.14–17 In the current study, no combination reached the 95% threshold. Ceftazidime combined with tobramycin yielded empiric coverage for 94% of isolates. Despite the small number of isolates tested against amikacin, it is conceivable a β-lactam in combination with amikacin may reach this desired threshold of 95%.
Combination therapy for P. aeruginosa remains a controversial practice. Routine use of combination therapy has not been consistently efficacious and, in some studies, was shown to increase adverse events. 29 However, most evidence examining the use of combination therapy is observational and may be prone to bias, thus confounding the ability to assess the benefit of combination therapy. 30 What appear to be the most compelling reasons to choose combination therapy include treating critically ill patients and those at risk for MDR organisms.7,13 With this being the primary purpose, it is prudent to select agents that provide the greatest likelihood of antimicrobial coverage. This study and others demonstrate that aminoglycosides provide better additional coverage than fluoroquinolones; however, we have observed that prescribers are reluctant to choose aminoglycosides on the basis of adverse nephrotoxic effects. Efforts to enforce evidence-based prescribing based upon local combination antibiograms must also account for system-level processes that influence such prescribing, such as electronic order sets that include fluoroquinolones and the availability of fluoroquinolones in the emergency department without pharmacist verification. If used appropriately, it is possible that combination antibiograms may reduce fluoroquinolone consumption within an institution.
Conclusion
Our results indicate aminoglycosides, particularly tobramycin, are more likely to possess activity against β-lactam NS P. aeruginosa isolates recovered from non-urinary, non-skin/skin structure sites. Empiric combination therapy may improve patient outcomes for invasive infections by increasing the likelihood of appropriate antimicrobial coverage. Local combination antibiograms should be generated to allow collaboration with prescribers to ensure optimal empiric prescribing, including appropriate updates to electronic order sets and antimicrobial use pathways. In addition to maximizing the likelihood of empiric antimicrobial activity against P. aeruginosa, these efforts can also serve as an antimicrobial stewardship initiative to reduce fluoroquinolone consumption.
Footnotes
Acknowledgements
Authors acknowledge the contribution of Natalie Carleton, PharmD BCPS for her assistance in data collection.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.