
Abstract
Legionella longbeachae is a Legionella bacteria often detected in soil, and is known as a rare cause of Legionella infections in Japan. In addition, detection of this Legionella species is often overlooked due to negative results from Legionella urinary antigen tests, which could lead to errors in the therapeutic approach. An 80-year-old woman was admitted to our hospital because of fever and dyspnea. Her blood tests showed elevated white blood cells, increased C-reactive protein and transaminases, and hyponatremia. Chest computed tomography showed dense consolidation in the right lung. We diagnosed Legionella pneumonia because the Legionella urinary antigen test was positive on the day after her admission. The patient was intubated and mechanically ventilated on the third day of hospitalization, because of respiratory failure. However, her condition did not improve and she died on the 10th day after admission. After her death, L. longbeachae was detected from sputum culture from her tracheal tube, and was diagnosed as the causative organism of her pneumonia. L. longbeachae infection reportedly rarely produces positive urinary antigen test results. Our experience suggests that the urinary antigen test using Ribotest Legionella might be able to detect Legionella spp. other than L. pneumophila.
Introduction
Legionella longbeachae was first detected in California, United States, in 1980. 1 L. longbeachae is often isolated from decaying leaves and soil, and Koide et al. 2 reported that it was detected from commercially available leaf mold in Japan.
Since Legionella spp. infections cause severe respiratory failure and multiple organ damage, rapid diagnosis and immediate treatment for Legionella spp. infections are critical. Currently, the urinary antigen test for Legionella spp. is commonly used for the diagnosis of Legionella spp. infections, because of its speed and convenience. 3 However, the test is mainly used for Legionella pneumophila, and the detection rate of other Legionella spp. is not high. 3 We report here a case of severe L. longbeachae pneumonia that tested positive by the Legionella urinary antigen test.
Case presentation
An 80-year-old woman presented to a nearby clinic for fever and chills that started 1 week earlier, and was prescribed acetaminophen and an oral cephem antibiotic. However, a few days later, she was referred to our hospital and was admitted because of worsening of her symptoms and decreased oxygen saturation levels. She had no significant previous medical history and no history of smoking. She grew vegetables and other crops in a field at home and often used the public bath near her home. On admission, she was completely conscious, her blood pressure was 120/64 mmHg, pulse rate was 92/min, and body temperature was 36.9°C. Her oxygen saturation was 92% while breathing nasal oxygen at the rate of 2 L/min. Auscultation indicated fine crackles in bilateral lower lung fields.
Her laboratory findings on admission are shown in Table 1. Her white blood cell (WBC) count, C-reactive protein (CRP), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and total bilirubin levels were elevated, and she had hyponatremia. There was no evidence of renal dysfunction. Chest computed tomography showed dense infiltrative shadows mainly in her right lung (Figure 1). The day after admission, her urine sample was positive for Legionella infection by the urinary Legionella antigen test using Ribotest Legionella (Asahi Kasei Pharma Corporation, Tokyo, Japan).
Laboratory data (day 1).

Alb, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; CK, creatine kinase; Cr, creatinine; CRP, C-reactive protein; Hb, hemoglobin; Ht, hematocrit; PLTS, platelets; RBC, red blood cells; S. pneumoniae, Streptococcus pneumonia; TP, total protein; WBC, white blood cells.

Chest computed tomography on day 1 showed consolidation in the right upper lung lobe.
Her clinical course is shown in Figure 2. On the day of admission, antibiotic therapy with lascufloxacin and meropenem were administered. Respiratory management with noninvasive positive pressure ventilation was started on day 2. However, since her respiratory condition worsened, she was intubated and mechanically ventilated from day 3 onward. A nasogastric tube was also placed and additional medication with azithromycin was started through a nasogastric tube. Although her CRP, AST, and ALT levels decreased after the start of antibiotic therapy, respiratory failure did not improve, and she died on the 10th day after admission. Her sputum collected from the tracheal tube at the time of intubation was cultured for 4 days at 36°C on buffered charcoal yeast extract (B-CYE) alfa agar (Eiken Chemical, Tokyo, Japan), a selective culture medium for isolation of Legionella spp. Bacteria cultured on B-CYE alfa formed grayish-white colonies with a shiny surface, indicative of possible Legionella spp. When bacterial identification was performed using the MALDI Biotyper (Bruker Daltonics, GmbH& Co. Kg, Bremen, Germany) mass spectrometer on bacteria obtained from cultivation, a score value of 2.0 or higher obtained by the mass analyzer was considered indicative of the same bacterial species. In this case, a score value of 2.55 was obtained, resulting in the identification of L. longbeachae without contradiction.4,5 Although there are some bacterial species that cannot be identified by mass spectrometry, L. longbeachae is considered identifiable using this method. 6 We obtained culture medium, humus, and field soil from the patient’s home. The samples were acid-treated using 0.2 M HCl-KCl buffer (pH 2.2) and incubated with B-CYE alfa for 1 week at 37°C. 2 Although the bacteria obtained were analyzed by mass spectrometry using the MALDI Biotyper, L. longbeachae was not detected. We subsequently tested and confirmed positivity of the cultured L. longbeachae using Ribotest Legionella in the same way as urine test. In order to closely examine the amount of bacteria in sputum culture, we prepared a bacterial solution adjusted to McFarland No. 1.0 and diluted it from 10× to 10,000× (Figure 3). As a result, the amount of bacteria in the original solution was 1.36 × 108 CFU/mL, which was again positive by Ribotest Legionella. However, the amount of bacteria in the solution diluted 100 times was 1.10 × 106 CFU/mL, which tested negative with Ribotest Legionella (Figure 4).

Clinical course of the patient.
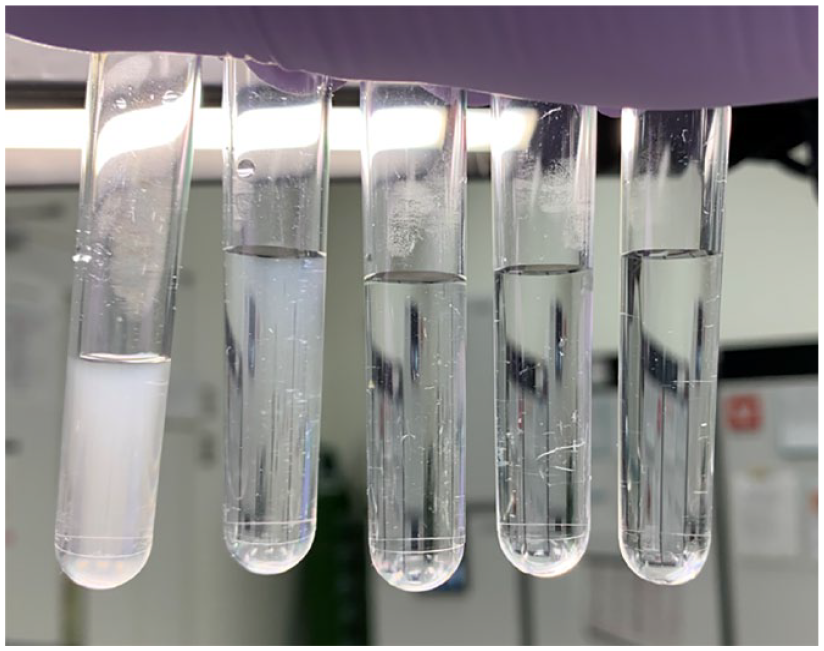
(From left to right) McFarland No. 1.0 and its dilutions of 100×, 1000×, and 10,000×, respectively.

Various dilutions of McFarland fluid were tested using Ribotest Legionella.
Discussion
Legionella spp. are small Gram-negative aerobic non–spore-forming bacilli, 0.3- to 0.9-μm-wide and 2- to 20-μm long. These bacteria require special media for growth, and many laboratories are unable to isolate Legionella spp. Thus, if the laboratory’s expertise is uncertain, a negative culture is meaningless. In addition, Gram stain cannot be used for identifying Legionella spp. Legionella spp. are aquatic organisms that grow in natural and man-made waterways and distribution systems, especially hot water pipes, electric water heaters, cooling towers, and water fountains. However, L. longbeachae grows in soil. 7 The bacteria growing in decaying soil are dispersed into the air by sprinkling water, and inhalation of the aerosol containing the L. longbeachae causes airway infection. In Japan, the Legionella Reference Center, consisting of the National Institute of Infectious Diseases and the Regional Institutes of Health, is responsible for the voluntary collection and analysis of clinical isolates of Legionella spp. According to the reports from this institute, 0.9% of Legionnaires’ disease cases are caused by L. longbeachae. 8 Studies from other countries reported that about 90% of the isolates of Legionella spp. were L. pneumophila, and about 4% were L. longbeachae. 9
The Legionella urinary antigen test is easy and simple. Although its sensitivity is not very high (81%), its specificity is high (100%), and a positive result is often considered a confirmed diagnosis. 10 However, the urine antigen test using the immunochromatographic method typically targets the L. pneumophila serogroup 1, and hence other Legionella spp. and serotypes are usually not identified by this test, producing negative test results. 11 Ribotest Legionella, the urinary antigen test used in our hospital, is a reagent to detect LPS antigen and L7/L12 antigen of L. pneumophila. In general, the reagent targets L. pneumophila serotypes 1–15 and is negative for L. longbeachae. However, Nakamura et al. 12 reported that Legionella spp. other than L. pneumophila can also be detected by this test, although the detection sensitivity is not as high as that for L. pneumophila. In the present case, L. longbeachae obtained from sputum culture was detected by Ribotest Legionella. We speculate that the reason for the positive result by Ribotest Legionella in our case might have been the large amount of L. longbeachae in the test sample. Although the unit for the amount of bacteria in the attached document of Ribotest Legionella was CFU/test, which is slightly different from our test, we found that Ribotest Legionella can detect the bacteria when it is present in large amounts.
L. longbeachae pneumonia and L. pneumophila pneumonia have similar clinical characteristics. According to the Legionella score developed by Miyashita et al., 13 a high possibility of Legionnaires’ disease is indicated if three or more of the following factors are present: male, no cough, dyspnea, hyponatremia, high lactate dehydrogenase, and CRP greater than 18 mg/dL. Despite the fact that our patient exhibited three of these characteristics and that she was able to receive treatment for Legionella pneumonia even before the positive urine antigen test, the administration of lascufloxacin did not improve her respiratory condition.
Conclusion
We report a case of L. longbeachae pneumonia with a positive urine antigen test result with Ribotest Legionella. In general, L. longbeachae infection presents a negative urinary antigen test result using Ribotest Legionella. However, the sensitivity of Ribotest Legionella might vary depending on the amount of bacteria in the test sample.