
Abstract
Background:
Neonatal sepsis (NNS) in developing countries continues to be a diagnostic and management challenge due to the delays in identifying the aetiologic pathogens and antibiograms.
Aim:
To determine the predominant bacterial isolates, antibiotic susceptibility pattern and outcomes of blood culture proven sepsis in neonates.
Methodology:
A hospital-based cross-sectional study of 120 neonates admitted into the Special Care Baby Unit (SCBU) of Nnamdi Azikiwe University Teaching Hospital Nnewi with clinical features suggestive of sepsis. A semi-structured questionnaire and proforma were used to record neonatal, maternal and laboratory information. Blood specimens were collected for aerobic culture using Bactenecin (BACTEC)-Ped plus culture system. Antibiotic susceptibility testing was performed using the Kirby Bauer disc diffusion method. Data obtained were analysed using SPSS version 23.0. p value < 0.05 was considered as significant.
Results:
There were 68 males and 52 females giving a male-to-female ratio of 1.3:1. The median age at admission was 48 h. Staphylococcus aureus 13 (43.3%) was the most common bacteria isolated. The prevalence of blood culture proven sepsis were 25% and 6.7% of the subjects with positive blood culture died. Gram-positive bacteria isolated were sensitive to gentamicin, vancomycin (VA), linezolid and resistant to penicillin. Gram-negative bacteria isolated were sensitive to meropenem (MEM), imipenem (IPM), ciprofloxacin (CIP) and resistant to ceftazidime, ceftriaxone, ampicillin and amoxicillin-clavulanic acid.
Conclusion:
The most common bacteria isolated causing NNS using BACTEC automated blood culture system was Staphylococcus aureus. The empirical antibiotics considered for use at the study site are gentamycin, VA for Gram-positive organisms and CIP, IPM and MEM for Gram-negative organisms. Some of the participants with positive blood culture died. Therefore, there is a need for regular antibiogram profiles in all hospitals offering neonatal care.
Introduction
Neonatal sepsis (NNS) is a medical emergency responsible for many neonatal admissions, especially in developing countries.1,2 Despite advances in early identification of risk factors, antimicrobial therapy and neonatal life support measures, NNS remains a major cause of morbidity and mortality in neonates worldwide. 3 It accounts for 26% of neonatal mortality in resource-poor countries. 4 Survivors of the illness experience major disabilities including adverse neurodevelopmental outcomes such as cerebral palsy, visual impairment, impaired growth and lower mental and psychomotor development index scores.5,6 The spectrum of causative organisms responsible for neonatal infection varies across different geographical areas and changes over time, even in the same place. 7 Group B Streptococcus was found to be the most prevalent organism causing NNS in a study conducted in England, 8 while in India, 9 it was observed that Klebsiella pneumoniae was the most prevalent organism isolated. From a study in Ethiopia, 2 Staphylococcus aureus was observed to be the most prevalent organism isolated. This variation within the same region is reflected in two different studies on NNS conducted within Nigeria which independently observed Klebsiella pneumoniae and Staphylococcus aureus to be the most prevalent organisms.1,10
As with the changes in bacterial patterns, the antimicrobial susceptibility patterns of pathogens also vary geographically and are dependent on local pathogens and patterns of antibiotic use. 11 Susceptibility patterns of pathogens to antibiotics also change from time to time even within the same practice region. This is observed in two studies conducted a year apart at different hospitals in South West Nigeria; both studies isolated similar organisms. However, in one of the studies, the isolates were susceptible to ofloxacin and ciprofloxacin (CIP), whereas in the other study, the isolates were susceptible to meropenem (MEM), CIP and amikacin (AK).12,13
Most studies done on NNS have been based on the conventional blood culture methods which are time-consuming, labour-intensive and associated with a lower positive yield.14,15 Automated blood culture systems have been reported to be among the most sensitive methods and are used in most countries worldwide. 15 It uses mechanisms that neutralize antimicrobial agents from blood or render the circulating drugs inactive. Moreover, the automated system can detect bacterial presence even at concentrations of 1–2 colony-forming units (CFU) per ml within 12–24 h using improved bacteriological techniques. 16 One such technology is Bactenecin (BACTEC), a fully automated system for detecting bacterial growth, it also has the advantage of a shorter detection time. 17
This study is, therefore, aimed at identifying bacterial isolates causing NNS using the BACTEC automated blood culture system, which guarantees a faster result, and higher yield. This study also determined antibiotic susceptibility patterns and outcomes. Findings of the study will be used in updating treatment protocols for the management of NNS at the tertiary institution as a similar study was last conducted in the study location in 2003. 18 Also, the findings from the study will improve paediatric practice in Nigeria and other developing countries in terms of increasing the awareness of the variations in pathogens and antibiotic susceptibility of bacterial isolates causing NNS over time in various regions and even in the same region.
Materials and Methods
Study design
This is a hospital-based cross-sectional study.
Study site
The study was conducted at the Special Care Baby Unit (SCBU) of the Paediatrics Department of the Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi, Anambra State, Nigeria.
Study population
All neonates admitted into the SCBU from February to July 2019.
Inclusion and exclusion criteria
All neonates admitted with at least two clinical features which include fever, refusal of feeds, lethargy, fast breathing, difficulty in breathing, irritability, seizures, unconsciousness and so on suggestive of sepsis and whose parents/caregivers gave signed informed consent were included in the study. Neonates with gross congenital abnormalities like obvious neural tube defects, gastroschisis and whose caregivers were not able to give accurate information and refused to give consent were excluded from the study.
Sampling method and sample size
Using Cochran’s formula, 120 neonates who met the inclusion criteria were recruited consecutively.
Data collection
A pre-tested semi-structured questionnaire and clinical proforma were used to record maternal and baby clinical and laboratory information. This information included relevant socio-demographic characteristics. This information was obtained by direct interviews with the caregivers and some from the patient’s hospital record. The socioeconomic class of the families were determined using Oyedeji’s social classification indices. 19
The blood sample collection was done under aseptic conditions and standard precautions were maintained. The site for venipuncture was first prepared to minimize contamination by skin flora with sterile cotton wool soaked with 70% alcohol, followed by 10% povidone-iodine. The site was then allowed to dry for about 30–60 s. One millilitre of the blood sample was introduced into a properly labelled BACTEC-Ped plus aerobic blood culture bottle after disinfecting the cover cap with alcohol. Blood samples were collected before the commencement of antibiotics and where the delay was unavoidable, the antibiotics were commenced before sample collection.
The BACTEC-Ped Plus blood culture bottle was then sent to the laboratory for incubation in the BACTEC 9050 automated system at a temperature of 37°C for 5 days with strict adherence to the manufacturer’s instructions. 20 Bacterial growth was indicated by a signal alarm system in the BACTEC automated blood culture machine, indicating a presumptive presence of a viable microorganism in the vial. Samples with bacterial growth were sub-cultured on blood agar and MacConkey agar and incubated at 35°C–37°C for 18–24 h. A positive culture on solid media was determined as up to one colony-forming unit (CFU) on the surface of the culture media along the line of streaking. The vials with no signal alarm were subcultured terminally by the end of the fifth day and were recorded as negative if no growth was observed on any of the culture plates. All isolates were identified based on colonial morphology, Gram-staining and results of biochemical testing such as catalase, coagulase, indole, citrate utilization, sugar utilization (with Kligler iron agar—KIA) tests using standard techniques for identification of organisms. 12
The antibiotic susceptibility test for the different isolates identified was performed by the Kirby Bauer disc diffusion method following the Clinical Laboratory Standard Institute (CLSI) 2017 guideline for antimicrobial susceptibility testing. The inoculum was standardized to 0.5 McFarland standard, which corresponds to the density of a bacterial suspension of 1.5 × 108 CFU/ml. 21 Different antibiotic discs were used for the test depending on the recommendations of CLSI for the individual isolates. The antibiotic discs were placed on the surface of a lawn of the standardized inoculum made on Mueller Hinton Agar plates, about 24 mm apart from each other (from the centre of one disc to the centre of another), and then incubated at 35 ± 2°C in ambient air for 16–18 h. 21 The isolates were considered susceptible, intermediate or resistant to the test antibiotics based on the breakpoint guidelines of the CLSI and the inhibition zone diameter (IZD) was measured in millimetres (mm). 21
Data analysis
Data were analysed using the Statistical Package for the Social Sciences (SPSS) software version 23.0 for windows. Frequency tables were generated for categorical variables. Test of association between categorical variables was done using the Chi-square test (or Fisher’s exact test as appropriate). A p-value of < 0.05 was taken as statistically significant.
Definition of variables
Early-onset sepsis (EONS) was classified as symptoms or signs consistent with sepsis at or before 72 h of life while late-onset sepsis (LONS) was classified as the onset of symptoms and signs consistent with sepsis after 72 h of life. 22
Neonates delivered before 37 completed weeks of gestation were classified as preterm, those delivered between 37 and 42 weeks of gestation were classified as term, and those delivered after 42 completed weeks of gestation were classified as post-term. 22
Neonates with birth weight less than 2500 g were classified as low birth weight, those who weighed between 2500 and 3999 g were classified as normal birth weight and those who weighed greater than or equal to 4000 g were classified as high birth weight. 22
Results
A total of 397 neonates were admitted into the SCBU during the study period (between February and July 2019). In total, 120 participants who met the inclusion criteria were recruited consecutively for the study.
General characteristics of the study population
The general characteristics of the participants are shown in Table 1. There were 68 (56.7%) males and 52 (43.3%) females giving a male-to-female ratio of 1.3:1. The median age at admission was 48 h while the mean birth weight was 2610.83 ± 913.30 g
General characteristics of the study population.

Class I and II, Upper Socioeconomic class; Class III, Middle Socioeconomic class; Class IV, Lower Socioeconomic class; GA, gestational age; IOR, interquartile range; SD, standard deviation.
Seventy-seven (64.2%) were term delivery and 47 (39.2%) of the study population were low birth weight. The mode of delivery was spontaneous vaginal in 90 (75%) and 64 (53.3%) of the study population were of social class IV.
Association between participants’ characteristics and NNS
The proportions of the male and female sex with positive blood culture were the same (25%).
Neonates delivered outside the study location (out-born neonates) had a higher percentage of positive blood culture (96.7%) than the inborn neonates, though this was not statistically significant (p-value = 0.070).
Term neonates had a higher prevalence of positive blood culture (32.5%) than preterm neonates (11.6%) and this difference was statistically significant (p-value = 0.011) (Table 2).
Association between participants’ characteristics and NNS.

NNS, neonatal sepsis.
Chi-square.
Fischer’s Exact.
Statistically significant.
Distribution of isolates by types of NNS
Thirty of the participants had positive blood cultures with a prevalence rate of 25%.
Staphylococcus aureus was the most frequently isolated organism from the 15 neonates with EONS (40%) and also from the 15 neonates with LONS (46.7%).
Staphylococcus aureus was isolated from 13.3% of term neonates and 6.7% of preterm neonates with EONS compared with 20% of term neonates and 3.3% of preterm neonates with LONS (Table 3).
Distribution of isolates by types of NNS.

EONS, early-onset NNS; LONS, late-onset NNS.
The outcome of NNS by organism
Mortality was reported in 2 (6.7%) of the participants. The organisms responsible for these mortalities were Acinetobacter boumanni and Enterococcus spp., respectively (Table 4).
Outcome of NNS by organism.

Antibiogram of the Gram-positive isolates
Staphylococcus aureus, the most prevalent organism isolated was maximally sensitive to gentamicin (CN) 92.3%, vancomycin (VA) 100% and linezolid (LZD) 100% while coagulase-negative Staphylococcus was maximally sensitive to CN 100%, VA 80% and LZD 80%. Enterococcus spp. was not sensitive to any of the antibiotics tested. Staphylococcus aureus, coagulase-negative Staphylococcus and Enterococcus spp. were 92.3%, 100% and 100% resistant to penicillin (PEN), respectively, as shown in Table 5.
Antibiogram of the Gram-positive isolates.
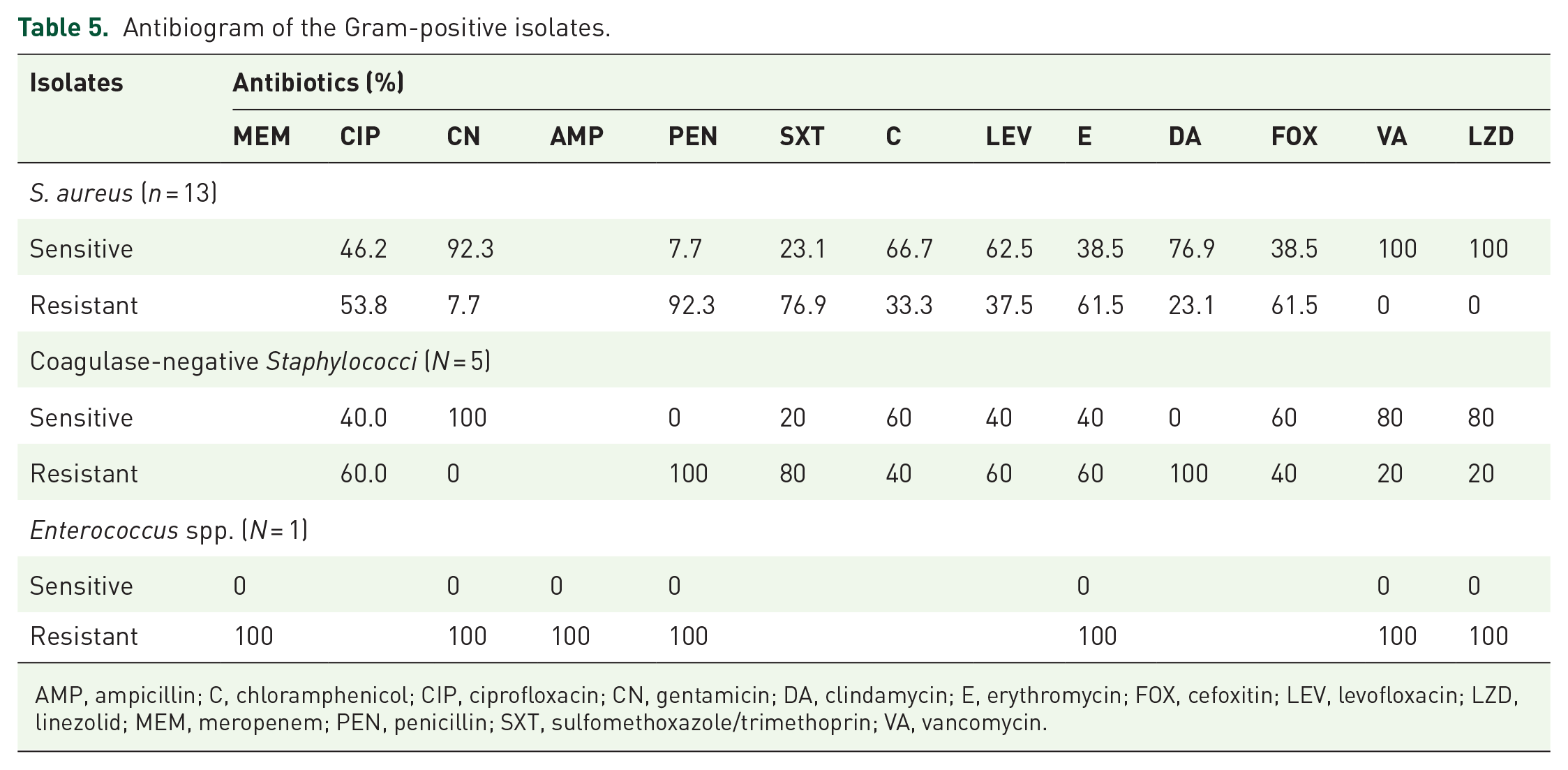
AMP, ampicillin; C, chloramphenicol; CIP, ciprofloxacin; CN, gentamicin; DA, clindamycin; E, erythromycin; FOX, cefoxitin; LEV, levofloxacin; LZD, linezolid; MEM, meropenem; PEN, penicillin; SXT, sulfomethoxazole/trimethoprin; VA, vancomycin.
Antibiogram of the Gram-negative isolates
Gram-negative organisms isolated were 100% sensitive to MEM, CIP, imipenem (IPM) and AK. There was 50% sensitivity of Escherichia coli to AK and 100% sensitivity to MEM, CIP and piperacillin–tazobactam (TZP). All Gram-negative organisms tested showed 100% resistance to ampicillin (AMP) and amoxicillin–clavulanic acid (AMC).
All Gram-negative isolates were majorly resistant to ceftazidime (CAZ) and ceftriaxone (CRO) except Serratia marcescens which was 100% sensitive to both antibiotics.
Pseudomonas aeruginosa, the only organism isolated in the inborn unit was 100% sensitive to MEM, CN, TZP, AK and IPM and showed 100% resistance to cefepime (FEP) and CAZ, as shown in Table 6.
Antibiogram of the Gram-negative isolates.

AK, amikacin; AMC, amoxicillin–clavulanate; AMP, ampicillin; CAZ, ceftazidime; CIP, ciprofloxacin; CN, gentamicin; CRO, ceftriaxone; CXM, cefuroxime; ETP, ertapenem; FEP, cefepime; IPM, imipenem; MEM, meropenem; TZP, piperacillin–tazobactam.
Discussion
The prevalence rate of blood culture proven bacterial NNS among neonates from this study was 25%. This is in contrast to an earlier study in this centre by Ugochukwu who obtained a rate of 10.8%. 18 The conventional blood culture was used in that study. The result of the current study is comparable with the work done by Shittu et al. 12 using BACTEC which reported a prevalence rate of 22.2%. BACTEC is documented to be highly sensitive with a better culture yield than the conventional methods. 17 However, some studies were done in Nigeria1,23 and other African countries2,24 that used the conventional blood culture method and reported higher prevalence rates than the current study. This may be attributable to the differences in the predisposing factors and infection control protocols in these centres. Lower prevalence was observed in studies carried out in Egypt, 25 and Nepal 26 with reported prevalence rates of 8.6% and 12.9%, respectively.
Gram-positive organisms (Staphylococcus aureus) were the predominant bacterial isolates in this study with 43.3% presence. The higher proportion of Gram-positive organisms in this study is similar to 53.6% reported by Peterside et al. 1 in Bayelsa, 54.5% reported by Ojukwu et al. 27 in Abakaliki, 63.8% reported by Ansari et al. 26 in Nepal. Staphylococcus is a normal commensal of the upper airway in about 10–25% of Nigerians and its acquisition through an asymptomatic carrier may be a possible source of infection. 5 Thus, the high prevalence of Staphylococcus aureus may be due to contamination of instruments used during the clinical procedures at birth and at the SCBUs. Also, contamination from mothers and caregivers may have led to an increase in the rate of transmission of Staphylococcus aureus in these neonates. However, studies conducted in India 7 and Pakistan, 28 found the presence of Gram-negative bacterial organisms to be more than Gram-positive.
From this study, Staphylococcus aureus was a common cause of sepsis in both EONS and LONS. It was more prevalent among neonates with EONS (46.7%) than those with LONS (40.0%). Similar studies in Nigeria1,23,27 also reported Staphylococcus aureus as the predominant isolate in LONS. This predominant LONS could be associated with unhygienic birth practices during delivery among health workers and caregivers who might be harbouring the organisms in their hands and nostrils. 23
Staphylococcus aureus was isolated from 76.9% of the term neonates and 23.1% of the preterm neonates. This finding is similar to the study done by Peterside et al. 1 in Bayelsa state who reported Staphylococcus aureus as the most prevalent organism in term neonates. It has been reported that socioeconomic status and vaginal flora of the mother influence the likelihood of sepsis in the newborn. 29 A previous study by Ako-Nai et al. 30 in Ile-Ife showed the existence of Staphylococcus aureus phage types, in the vagina of mothers which are identical to those that colonized the anterior nares of their corresponding neonates. This suggests the maternal contamination of these neonates at birth with potential pathogens. 30
Mortality was reported in 2 (6.7%) of the participants with positive blood culture while 28 (93.3%) of the participants with positive blood culture were discharged. The organisms responsible for these mortalities were Acinetobacter boumanni and Enterococcus spp. This finding is comparable with a hospital-based study conducted in Ethiopia where mortality due to sepsis was 4%. 31 Other studies5,32 reported varied proportions of neonatal mortalities due to NNS. These observations reflect the contribution of NNS to infant mortality.
Concerning the antibiotic susceptibility pattern in this study, Staphylococcus aureus (Gram-positive cocci) which was the most predominant isolate, was highly sensitive to VA (100%), LZD (100%) and CN (92.3%). This may probably be because CN and VA are not frequently used in neonates in the study centre while LZD is not readily available in the country. This finding was closely similar to the study done by Jayasimha et al. 33 who observed that all the Gram-positive isolates were sensitive to LZD, VA and CN. Also, Sarangi et al. 34 in their study showed the maximum sensitivity of Gram-positive isolates to VA and LZD. In the same vein, Komolafe and Adegoke in their study found that more than 80% of Staphylococcus aureus was sensitive to CN and VA. 35 Ansari et al. 26 in their studies also found Staphylococcus aureus to be 100% sensitive to VA. However, an earlier study done in the same centre by Ugochukwu found Staphylococcus aureus to be 100% sensitive to CIP. 18 This is unlike this study which reported 46.2% sensitivity of Staphylococcus aureus to CIP. This variation in findings could probably be because antibiotic sensitivity may differ at different times due to the emergence of resistant strains from the indiscriminate use of antibiotics. 26
Staphylococcus aureus was highly resistant to PEN, sulphadoxine-trimethoprim, erythromycin and cefoxitin in this study suggesting that these antibiotics cannot be used for empirical treatment of NNS in our centre. Mustapha and Ahmed 36 reported that Gram-positive organisms showed high resistance to erythromycin, AMP and amoxicillin. The development of resistance may follow prolonged use of similar antibiotics necessitating the present research into sensitivity patterns and possible change of empirical regimen.
In the present study, the Gram-negative organisms isolated were 100% sensitive to MEM, CIP, IPM and AK. This finding is similar to a study conducted by Jayasimha et al. 33 who reported that Gram-negative organisms isolated were sensitive to AK, IPM, levofloxacin and MEM. Similarly, Sarangi et al. 34 in their study observed that Gram-negative isolates showed maximum sensitivity to AK, IPM, MEM and CIP. The Gram-negative organisms isolated from this study were 100% resistant to AMC, AMP and CRO. This finding may be attributed to the widespread and indiscriminate use of these antibiotics in the country often without prescription and also in inadequate doses. 27 Therefore, the results of the antibiogram in this study suggest that VA, LZD and CN could be considered as possible empirical antibiotics of choice for Gram-positive organisms, whereas MEM, CIP, IPM and AK for Gram-negative organisms as CAZ is presently in use as empirical antibiotics for the treatment at the study centre.
Study limitations
This study did not capture anaerobic organisms due to the lack of facilities. Also, another limitation of this study is the limited generalizability of the results. As this was a hospital-based study, the results might not be representative of the general population.
Conclusion
This study found that Staphylococcus aureus was the most common offending organism. The empirical treatment of NNS based on the research finding is gentamycin, and VA for Gram-positive organisms and CIP, IPM and MEM for Gram-negative organisms. We was found that 6.7% of the participants with positive blood cultures died, whereas 93.3% were discharged.
There is a need for a change from the current empirical antibiotics used for NNS in our neonatal unit and also a need for regular antibiogram profiles in all hospitals offering neonatal care. This will help provide a proper guideline for the empirical treatment of NNS and reduce the emergence of drug resistance.
Future studies should be carried out to assess anaerobic organisms.