
Abstract
Background:
Coronavirus disease-2019 (COVID-19) is a potentially life-threatening illness with no established treatment. Cardiovascular risk factors (CRFs) exacerbate COVID-19 morbidity and mortality.
Objective:
To determine the prevalence of CRF and clinical outcomes of patients hospitalized with COVID-19 in a tertiary hospital in Somalia.
Methods:
We reviewed the medical records of patients aged 18 years or older with a real-time polymerase chain reaction (RT-PCR)–confirmed COVID-19 hospitalized at the De Martino Hospital in Mogadishu, Somalia, between March and July 2020.
Results:
We enrolled 230 participants; 159 (69.1%) males, median age was 56 (41–66) years. In-hospital mortality was 19.6% (n = 45); 77.8% in the intensive care unit (ICU) compared with 22.2%, in the general wards (p < 0.001). Age ⩾ 40 years [odds ratio (OR): 3.6, 95% confidence interval (CI): 1.2–10.6, p = 0.020], chronic heart disease (OR: 9.3, 95% CI: 2.2–38.9, p = 0.002), and diabetes mellitus (OR: 3.2, 95% CI: 1.6–6.2, p < 0.001) were associated with increased odds of mortality. Forty-three (18.7%) participants required ICU admission. Age ⩾ 40 years (OR: 7.5, 95% CI: 1.7–32.1, p = 0.007), diabetes mellitus (OR: 3.2, 95% CI: 1.6–6.3, p < 0.001), and hypertension (OR: 2.5, 95% CI: 1.2–5.2, p = 0.014) were associated with ICU admission. For every additional CRF, the odds of admission into the ICU increased threefold (OR: 2.7, 95% CI: 1.2–5.2, p < 0.001), while the odds of dying increased twofold (OR: 2.1, 95% CI: 1.3–3.2, p < 0.001).
Conclusions:
We report a very high prevalence of CRF among patients hospitalized with COVID-19 in Somalia. Mortality rates were unacceptably high, particularly among those with advanced age, underlying chronic heart disease, and diabetes.
Introduction
The coronavirus disease-2019 (COVID-19) is an emerging infectious disease of global public health significance caused by a novel coronavirus called the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) which first appeared at the end of December 2019 in Wuhan, China. 1
Most persons with COVID-19 present with mild to moderate disease characterized by nonproductive cough, fever, and malaise. However, a small but significant proportion of the patients present with multisystemic involvement manifesting as multi-organ failure, hypercoagulability, and secondary bacterial or fungal infections.2,3
Overall, COVID-19 has a mortality rate of about 4–5%. 4 However, mortality is markedly increased in patients with underlying medical conditions, such as diabetes mellitus, hypertension, obesity, chronic lung disease, and malignancies. 5 In addition, poor outcomes have been reported in patients with advanced age (⩾65 years) and those with uncontrolled HIV infection.4,5
The association between increased cardiovascular disease (CVD) mortality and viral infections, for example, caused by the influenza virus is well known.6,7 Pre-existing CVDs such as hypertension and dyslipidemia have also been associated with worse outcomes of COVID-19.4,7,8
In a single-center study, from the early outbreak of COVID-19 pandemic in China, the in-hospital mortality rate was about 36% with hypertension, diabetes mellitus, CVDs, and chronic obstructive pulmonary disease being the commonest risk factors associated with higher mortality rates. 9 Another study from Brazil reported in-hospital mortality rate of about 40%, with cardiovascular and kidney diseases being strongly associated with deaths. 10 However, in this study, smoking and obesity were not associated with COVID-19-related deaths. 10
However, only a limited number of studies have investigated morbidity and mortality predictors among patients hospitalized with COVID-19 in resource-limited settings. As of 19 February 2022, Somalia had recorded 26,260 cases with 1345 deaths – translating to a 5.1% mortality rate. With this relatively high death rate, associated factors must be investigated. Therefore, in this study, we determined the prevalence of cardiovascular risk factors (CRFs) and clinical outcomes of patients hospitalized with COVID-19 in a tertiary hospital in Somalia.
Materials and methods
Study setting and design
This retrospective study was conducted at the De Martino Hospital in Mogadishu, Somalia, from March to July 2020. We reviewed the medical files of hospitalized COVID-19 patients who were 18 years or older with a positive real-time polymerase chain reaction (RT-PCR).
CVD risk assessment
Demographic data (age, sex) as well as CRF (hypertension, diabetes mellitus, previous or current chronic heart disease, smoking, obesity), history of renal disease, asthma, chronic obstructive pulmonary disease, tuberculosis, and liver diseases were extracted from the patient’s medical records. Our primary outcome was COVID-19-related mortality and our secondary outcome was the need for intensive care unit (ICU) admission.
Definitions
Critical COVID-19 illness was defined by the criteria for acute respiratory distress syndrome, sepsis, septic shock, or other conditions that would normally require the provision of life-sustaining therapies such as mechanical ventilation or vasopressor therapy.
Severe COVID-19 disease was defined by the presence of any of the following criteria:
Oxygen saturation <90% on room air;
Respiratory rate >30 breaths;
Signs of severe respiratory distress (accessory muscle use, inability to complete full sentences).
Data analysis
Continuous data were presented as mean with standard deviation (SD) or median with interquartile range (IQR), whereas categorical data were summarized as frequencies and percentages. Numerical variables were compared using the Mann–Whitney U test or Wilcoxon signed rank sum test and categorical variables using either the chi-square or Fisher’s exact tests as appropriate. A multivariable simple logistic regression analysis was performed to investigate mortality and ICU admission factors. All variables with a p < 0.2 at univariate analysis were introduced in the final logistic regression analysis to determine associations. We conducted Kaplan–Meier survival curve analysis and Cox-proportional hazard ratios to establish 7-, 14-, and 21-day mortality, and predictors of mortality and ICU admissions. All data analyses were performed using STATA version 16 software. p < 0.05 was considered statistically significant.
Results
Baseline characteristics
Data of 230 eligible participants with RT-PCR-confirmed COVID-19 were analyzed. Of these, 159 (69.1%) were male and the overall median age was 56 years (IQR: 41–66 years). About two-thirds (64.8%) were aged 50 years and above, and only one patient was a health care worker (Table 1).
Characteristics of the patients at admission.
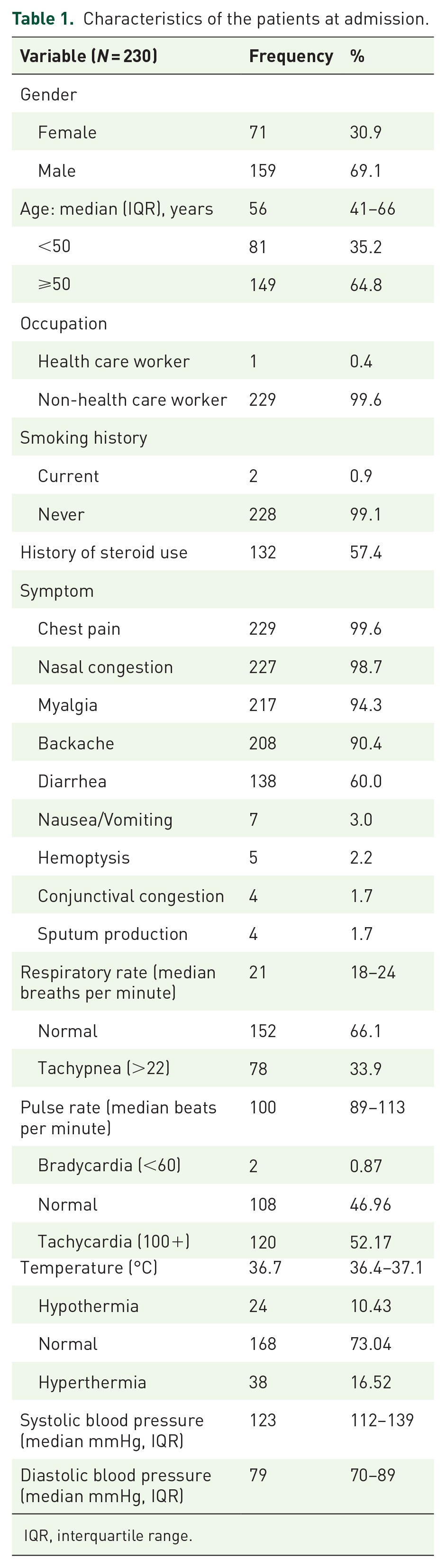
IQR, interquartile range.
About 57.4% (n = 228) had been treated with dexamethasone for their SARS-CoV-2 infection. There was a history of smoking in two, but alcohol intake was not reported. More than half (52.2%) had tachycardia and 38 patients (16.5%) had hyperthermia.
Cardiovascular risk factors
Diabetes and hypertension were the commonest comorbidities, present in 82 (36%) and 42 (21%) patients, respectively (Figure 1).
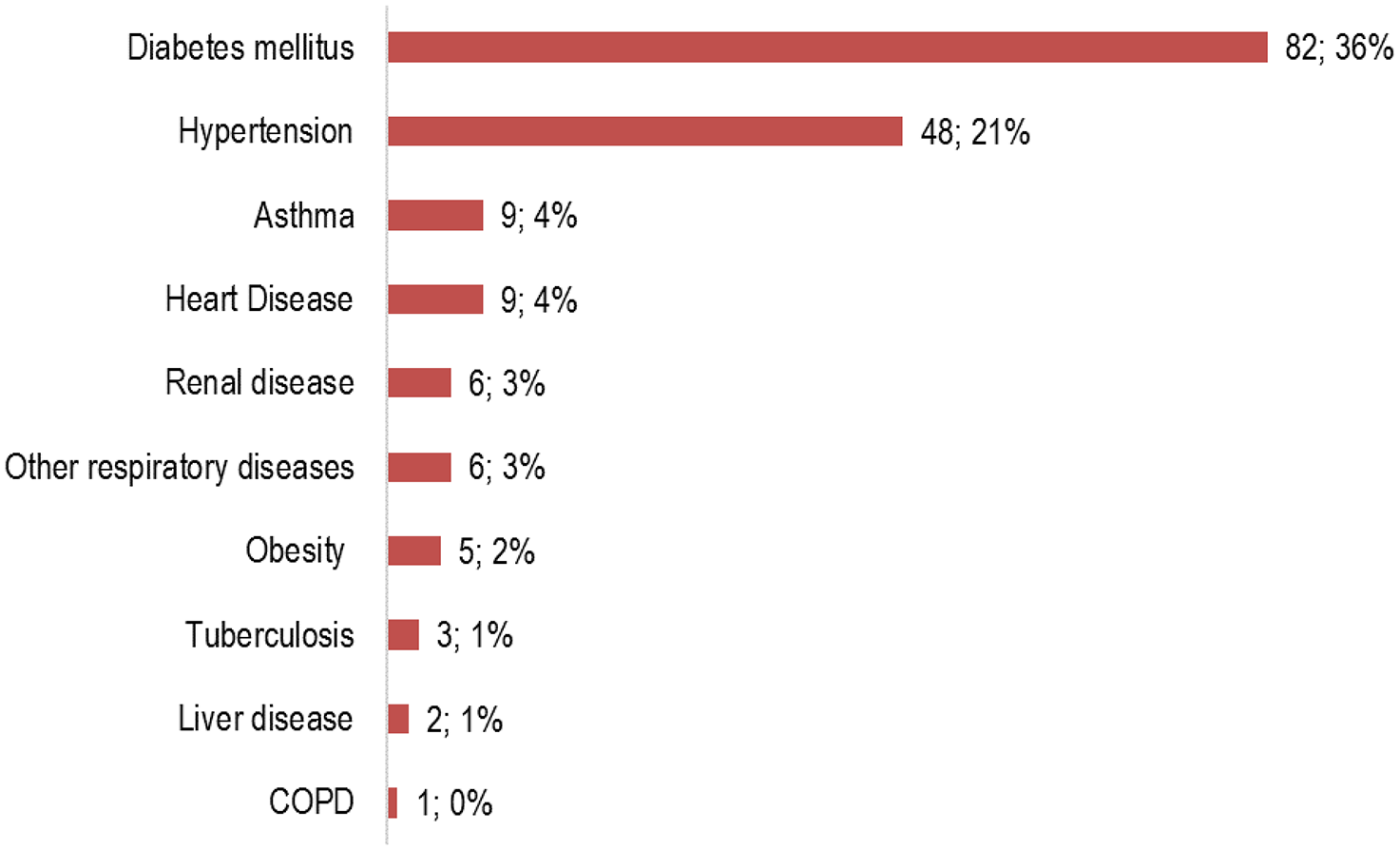
Underlying comorbidities of the participants. Heart disease included cardiomyopathies, vulvular heart diseases, and coronary artery diseases.
Overall, 221 patients [96.1%, 95% confidence interval (CI): 92.6–98.0%] had at least one CRF, with more than one-third (n = 85, 37%) having two CRFs (Figure 2).

Number of comorbidities among the 230 hospitalized patients.
COVID-19 outcomes and associated factors
Twenty-two (9.6%) had been admitted with severe or 36 (15.7%) with critical COVID-19 (Figure 3).

Severity of COVID-19 illness among the participants.
During the study period, 45/230 deaths (19.6%, 95% CI: 14.9–25.2%) were recorded (Table 2). The majority of deaths occurred in the ICU compared with the general wards 35/45 (77.8%) versus 10/45 (22.2%), p < 0.001. Thirty-five (81.4%) out of 43 patients hospitalized at the ICU died. CRFs associated with mortality at bivariate analysis were age ⩾40 years (p = 0.016), diabetes (p = 0.001), and underlying chronic heart disease (p = 0.002). Patients aged ⩾40 years were 3.6 times more likely to die [odds ratio (OR): 3.6, 95% CI: 1.2–10.6, p = 0.020]. Patients with diabetes mellitus (OR: 3.2, 95% CI: 1.6–6.2, p = 0.001) and previous heart disease (OR: 9.3, 95% CI: 2.2–38.9, p = 0.002) also had higher odds of dying.
Factors associated with intensive care unit admission and mortality.

CI, confidence interval; CRF, cardiovascular risk factor; OR, odds ratio.
Chronic heart disease included cardiomyopathies, arrythmias, and vulvular heart diseases.
Forty-three (18.7%, 95% CI: 14.2–24.3%) patients had been admitted to the ICU (Table 2). Age ⩾40 years (p = 0.001), smoking history (p = 0.034), diabetes mellitus (p = 0.001), and hypertension (p = 0.012) were associated with ICU admission. At simple logistic regression, age ⩾40 years (OR: 7.5, 95% CI: 1.7–32.1, p = 0.007), diabetes (OR: 3.2, 95% CI: 1.6–6.3, p = 0.001), and hypertension (OR: 2.5, 95% CI: 1.2–5.2, p = 0.014) remained significantly associated with increased likelihood of ICU admission.
The number of CRFs among patients with COVID-19 disease was significantly associated with both ICU admission and death. Patients who were admitted to the ICU or those who died had more CRFs than those who were admitted to the general ward or those who survived (3 versus 2 CRFs, p < 0.001), respectively. In addition, for every additional CRF, the odds of admission into the ICU increased threefold (OR: 2.7, 95% CI: 1.2–5.2, p < 0.001) whereas the odds of dying from COVID-19 increased twofold (OR: 2.1, 95% CI: 1.3–3.2, p = 0.001).
In-hospital mortality
Overall, survival at 7, 14, and 21 days from the date of admission was 78% (95% CI: 71–84%), 62% (95% CI: 48–74%), and 56% (95% CI: 37–71%) (Figure 4).

Kaplan–Meier curve showing overall survival.
The log-rank test showed that survival time significantly differed by diabetes status and the ward where the patients were admitted (Figure 5). A Cox-proportional hazards regression model was performed to estimate risks of dying from the date of admission. Patients with diabetes mellitus were 2.5 at higher risk of dying (hazard ratio: 2.5, 95% CI: 1.4–4.8, p = 0.004) (Figure 5).

Kaplan–Meier curve showing survival in patients with diabetes mellitus versus those without (log-rank test, p = 0.002).
In addition, patients admitted to the ICU were 19 times at higher risk of dying compared with those admitted to general wards (p < 0.001) (Figure 6).

Kaplan–Meier curve showing survival from admission (log-rank test p value < 0.0001).
Discussion
Data on clinical outcomes of patients hospitalized with COVID-19 in resource-limited settings remain scarce. In this retrospective cohort study of hospitalized patients admitted with COVID-19 in a tertiary health care center in Mogadishu, more than 95% of the participants had at least one CRF. More than one-third of the patients had diabetes mellitus, about one-fourth had hypertension, 4% had chronic heart disease, and 2% were obese. These findings are consistent with previous systematic reviews and large cohort studies which report a high prevalence of CRF such as age, male sex, hypertension, diabetes mellitus, and tobacco use in patients with severe COVID-19.11–13
Up to one-fourth of the patients presented with severe or critical illness, with close to 19% of the patients requiring ICU admission. Moreover, patients admitted to the ICU had 19 times higher risk of dying of COVID-19 compared with those admitted to the general wards. The Mogadishu De Martino Hospital ICU mortality of 81.4% is much higher than the 32% ICU COVID-19 mortality reported in a similar study in Cameroon. 14 This higher mortality rate could be explained by the high CRF in the study population. This is also higher than the 48.2% in-hospital mortality reported in a recent multicenter, prospective cohort study of more than 3000 critically ill patients with COVID-19 enrolled in 64 hospitals in 10 African countries. 15 In the latter study, in addition to the traditional risk factors for adverse COVID-19 outcomes, persons living with HIV/AIDS and those who experienced delayed access to high-care units and ICU had higher mortality rates.15,16 The prevalence of HIV infection in Somalia is low and none of the participants had an underlying HIV infection. Even in high-income settings, ICU mortality is high. A recent study from the United States reported that about 50% of patients requiring ICU admissions chose palliative care instead to avoid medically ineffective treatment. 17 In resource-limited settings, however, non-ICU utilization is mostly due to nonavailability, inaccessibility, or inability to afford ICU care. 16 At Mogadishu De Martino Hospital, the ICU disposes of 20 beds and 4 ventilators but there is a lack of intensive care expertise and supplies, explaining the high mortality.
Our overall 19.6% in-hospital mortality rate is slightly higher than the 12% reported in a recent systematic review of main studies from China, 5 the United States, 17 and Europe. 13 This could be due to a lack of adequate treatment options in our setting. Predictors of deaths in our study were age ⩾40 years (3.6-fold), diabetes (3.2-fold), and underlying chronic heart disease (9.3-fold). These findings are consistent with data from a meta-analysis that suggested that older age and diabetes mellitus are associated with a higher risk of in-hospital mortality in SARS-CoV-2-infected patients. 13 Obesity is a strong predictor of poor outcomes in COVID-19 irrespective of age and gender. 18 However, in our study, the prevalence of obesity was very low and therefore its association with increased mortality could not be assessed. Underlying CRF is key determinant of in-hospital mortality, and therefore requires adequate management in addition to COVID-19-specific treatments.
COVID-19 and CRF have negative bilateral interactions. 19 On one hand, patients with CRF are more likely to develop severe disease or die of COVID-19.13,17,20 On the other hand, indirect and direct cardiovascular insults such as myocardial injury, acute coronary syndrome, acute heart failure, myocarditis, pericardial diseases, arrhythmias, takotsubo syndrome, and arterial and venous athero-thrombotic and thromboembolic events are more likely to occur in patients with COVID-19. 19 Moreover, patients with COVID-19 are at an increased risk of developing diabetes due to the destructive effect of SARS-COV-2 on the pancreatic beta islets 21 and the hyperglycemic effect of glucocorticoids which are routinely used in the treatment of severe COVID-19. 22
Our study has several important limitations. First of all, it was a retrospective review of medical records with limited data that could be extracted. Data on pharmacological treatment and administration of oxygen were not captured. Therefore, the effect of various treatment options could not be investigated. We also only collected in-hospital mortality data. Therefore, we may have underestimated the real mortality rate as some patients, after leaving the hospital, may have died at home. Finally, the data were captured from a tertiary, referral, and academic health care facility set up to manage only patients with COVID-19, most of whom had moderate to severe disease. As such, these findings may not be generalized to other centers across the country which may be caring for mainly mild cases. A large, multicenter prospective study would be welcome to validate our findings and provide further insights into this evolving viral illness.
Conclusion
In conclusion, we report a very high prevalence of CRF among patients hospitalized with COVID-19 in Somalia. Mortality rates were unacceptably high, particularly among those with advanced age, underlying chronic heart disease, and diabetes. In this resource-limited setting, a multidisciplinary management of patients with COVID-19, with emphasis on the treatment of underlying poor prognostic comorbidities, may improve clinical outcomes. Most important is the prevention of CVD and the prioritization of vaccination against COVID-19 of persons with CRF.
Footnotes
Acknowledgements
We are grateful to the De Martino Hospital administration for providing the patient records, and we thank the frontline health workers for collecting these important data from patients despite the pandemic.
Ethics approval
The study protocol was approved by the Mogadishu University’s Institutional Review Board (MU-IRB), reference number (Ref.MU-IRB/02/21), and conducted according to the Declaration of Helsinki. A consent waiver to review medical records was obtained from Mogadishu University’s Institutional Review Board. All data were anonymously and securely stored in a password-protected server.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and material
All data are available upon reasonable request from the first author.
Code availability
Not applicable