
Abstract
The coronavirus disease of 2019 (COVID-19) has caused significant morbidity and mortality among infected individuals across the world. High transmissibility rate of the causative virus – Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) – has led to immense strain and bottlenecking of the health care system. While noteworthy advances in vaccine development have been made amid the current global pandemic, most therapeutic agents are repurposed from use in other viral infections and are being evaluated for efficacy in COVID-19. Favipiravir, an orally administered drug originally developed in Japan against emerging influenza viral strains, has been shown to have widespread application and safety across multiple ribonucleic acid (RNA) viral infections. With a strong affinity toward the viral RNA-dependent RNA polymerase (RdRp), favipiravir could be a promising therapy against SARS-CoV-2, by targeting downstream viral RNA replication. Initial trials for usage in COVID-19 have suggested that favipiravir administration during initial infection stages, in individuals with mild to moderate infection, has a strong potential to improve clinical outcomes. However, additional well-designed clinical trials are required to closely examine ideal timing of drug administration, dosage, and duration, to assess the role of favipiravir in COVID-19 therapy. This review provides evidence-based insights and throws light on the current clinical trials examining the efficacy of favipiravir in tackling COVID-19, including its mechanism, pharmacodynamics, and pharmacokinetics.
Introduction
SARS-CoV-2 and its anatomy
The coronavirus disease of 2019 (COVID-19) has infected over 242 million people, leading to over 4.9 million deaths worldwide, at the time of this publication. 1 It is caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2),2,3 closely related to Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) and Middle East Respiratory Syndrome Coronavirus (MERS-CoV).3,4 SARS-CoV-2 is a single-stranded positive sense ribonucleic acid (RNA) virus, 50–200 nm in diameter, consists of four structural proteins (about 33% of viral genome) – Spike (S), Envelope (E), Membrane (M), and Nucleocapsid (N). 5 The S protein, comprising of S1 and S2 subunits, mediates viral entry into the host cell membrane via the human cell angiotensin converting enzyme 2 (ACE2) receptor. 5 The remaining 67% of the viral genome encodes polyproteins and precursors that further cleave into 16 non-structural proteins (nsp), like the RNA-dependent RNA polymerase (RdRp), critical for viral life cycle – replication and host immune system regulation. 6 RdRp complex like nsp-12, with assistance of other cofactor proteins (like nsp7-nsp-8 heterodimer), handles the viral replication and transcription process of the virus.6,7 Interestingly, across RNA viral classes, various sequence motifs and tertiary structures of RdRps are conserved.4,7–11 These conserved RdRp motifs are essential for its catalytic function, hence useful as potential drug targets.4,12
COVID-19 pathogenesis and symptoms
COVID-19 is a multisystemic viral disease and commonly affects the respiratory tract. 13 SARS-CoV-2 is transmitted mainly through droplets and exhibits pulmonary tropism, which is attributable to ACE2 receptors being widely distributed across lung epithelial cells. 14 Clinical manifestations in human hosts can be wide ranging from asymptomatic to symptomatic disease with potential for sudden symptom evolution.12,14 Symptoms of mild disease may include fever, myalgia, cough, fatigue, anosmia, dysgeusia, and shortness of breath while moderate-severe or critical illness may lead to prolonged hospitalization, cytokine storm, viral pneumonia, secondary bacterial or fungal pneumonia, arrhythmias, acute kidney injury, neurological illness, and so on. 12 The COVID-19 response in some individuals can lead to a complex immunological cascade leading to a cytokine storm with damage to multiple organs.13,15 Symptomatic disease could eventually lead to post-acute COVID-19 syndrome.16,17 The exact duration for which these symptoms persist after resolution of acute disease remains to be fully understood.
COVID-19 management
While COVID-19 prevention is largely associated with targeting viral spike and structural proteins by highly efficacious vaccination – generating robust humoral antibody response – hospitalization-associated patient management and therapy is critically symptom associated. Identification of clinical disease staging – clinical symptoms combined with laboratory and radiologic assessment – are critical for risk stratification, triage, and early therapeutic intervention of patients who progress to severe disease, requiring hospitalization.13,18 In hospitalized patients, mechanical ventilation, oxygen therapy, and symptomatic treatment have been the mainstay of therapy. 19 While there is no clinically effective therapy for COVID-19 in singular, several therapeutic agents such as corticosteroids, antivirals, monoclonal antibodies, and convalescent plasma are currently being administered and evaluated, many a times, in conjunction. Antivirals have a special role to play, repurposed through their role in other viral infections, preventing viral entry into the host cells and causing suppression of viral replication at various steps. 20 Some key antivirals of interest are listed in Table 1.
Repurposed antivirals being evaluated for therapeutic activity in COVID-19.

ACE2, angiotensin converting enzyme 2; HIV, Human Immunodeficiency Virus; MERS, Middle East Respiratory Syndrome; RNA, ribonucleic acid; RSV, Respiratory Syncytial Virus; SARS, Severe Acute Respiratory Syndrome.
Several clinical trials recruiting patients across the disease stages are trying to identify the most efficacious drug(s) for efficacious COVID-19 therapy, and retroviral therapies have been of most interest.21,23 Remdesivir has been used under emergency use authorization in several countries, demonstrating some efficacy in shortening recovery time in COVID-19 patients. 27 The combination of lopinavir with ritonavir showed some favorable outcome, but a clinical trial was discontinued due to side effects. 19 Ribavirin, a guanine analog targeting viral RdRp was found to be ineffective in improving COVID-19 recovery outcomes, although in combination triple therapy with lopinavir and ritonavir, with interferon beta-1b, some improvement in efficacy was observed to decrease recovery in hospitalized patients with mild to moderate COVID-19. 25 In addition, singular therapy with umifenovir (arbidol) did not improve patient outcomes. 26 Favipiravir, similar in action to remdesivir, inhibits transcription and replication of multiple RNA viruses by targeting RdRp. 28
Favipiravir
Drug development and pharmacodynamics
In the process of viral replication, RdRp is a critical element, conserved across RNA viruses but absent in human cells, making it a promising antiviral target. 12 Favipiravir was developed by Toyama Chemical Company Limited and was first approved for clinical use in Japan in 2014, for novel and re-emerging influenza virus infections. It was discovered through a library screen of chemical candidates utilizing a plaque reduction assay.28,29 Understanding efficacy of favipiravir in COVID-19 is of particularly high interest,30,31 as it has been shown to have effective in vitro and in vivo antiviral activity against RNA viruses of multiple families – orthomyxoviridae, bunyaviridae, arenaviridae, filoviridae, rhabdoviridae, paramyxoviridae, flaviviridae, togaviridae, picornaviridae, and caliciviridae.22,32,33 Favipiravir is a pyrazine carboxamide derivative and is a prodrug; its active metabolite, favipiravir ribofuranosyl 5′ triphosphate (T-705 RTP), is formed by phosphoribosylation and is a nucleoside analog causing disruption of viral replication.29,33–35 It was observed that neither favipiravir nor favipiravir-ribofuranosyl-5′-monophosphate inhibited RdRp activity, instead the triphosphate metabolism of favipiravir to T-705 RTP lead to active influenza viral inhibition, through concentration dose-dependent studies. 28 Plaque reduction with time of addition assays were utilized to define the mechanism of action by exposing influenza infected cells to favipiravir. It was observed that plaque inhibitory activity was observed during the replication phase and not adsorption or release phase. 28 While competitive assays were used to investigate the mechanism of inhibition, 28 it was observed that the antiviral activity of favipiravir was significantly decreased in presence of natural purine nucleoside and not pyrimidine bases, thus indicating its mechanism of action as a pseudo purine, through RdRp.28,36 Although the precise interaction is not known, it is hypothesized that this active form either binds to the catalytic format of RdRp or gets misincorporated to the nascent growing viral RNA, leading to chain termination by ambiguous base-pairing, in turn causing abrupt break in viral replication36,37 (Figure 1). Sequencing of nucleoprotein clones revealed a higher mutation frequency and associated shift in the nucleotide profiles of the nucleoprotein gene. In addition, no viable favipiravir-resistant mutants were observed, suggesting a ‘virucidal’ effect.28,34 The wide-spectrum activity of favipiravir may be associated with this misincorporation effect. The lethal mutagenesis and subsequent chain termination mechanism has been suggested against multiple RNA viral infections as well.34,35,38,39 One study indicated that binding of the T-705 RTP to RdRp may not lead to sufficient inhibition of norovirus activity. 40 Although, it may be possible that variable concentration and availability of the drug may be key in impacting the mechanism of action. 37 In addition, as this mechanism of action is vastly different to some other antivirals that inhibit cellular RNA or DNA synthesis – as with ribavirin and the neuraminidase inhibitors – favipiravir, instead, specifically acting on viral RdRp may be responsible for observed lower toxicity while being target sensitive and efficacious across multiple classes of RNA viruses. 36 At 50% inhibitory concentration, favipiravir was about 2650 times more selective for influenza RdRp, while lacking inhibition of human RNA or DNA synthesis.36,41

Schematic showing the mechanisms of action associated with favipiravir.
Pharmacokinetics and safety
Favipiravir is metabolized mainly by aldehyde oxidase (AO) and partly metabolized to a hydroxylated form by xanthine oxidase (XO). A glucuronate conjugate was observed in human plasma and urine as a metabolite other than the hydroxylated form. It is predominantly excreted into the urine as a hydroxylated form, with minimal unchanged drug. The pharmacokinetic profile of favipiravir has been studied through dose-escalated studies, with oral dosage for adults at 1600 mg twice daily on day 1 (loading dose), followed by 600 mg twice daily for 4 days, with the total duration of therapy being 5 days. 29 The maximum plasma concentration was achieved within 2 h after administration of a single dose, although plasma concentration quickly decreased, with half-life between 2 and 6 h.29,42 Interestingly, administration of multiple doses led to an increase in the time to maximum plasma concentration and half-life. 42 Favipiravir is associated with dose- and time-dependent pharmacokinetics, possibly explainable by saturation of the main enzymatic pathway as it was shown to inhibit AO in vitro.29,42 In Ebola-infected patients, the favipiravir plasma concentration surprisingly decreased between treatments, potentially due to severe disease conditions or intrinsic properties of favipiravir metabolism. 43 In variable disease conditions, favipiravir bioavailability and the hepatic first pass can be altered, through an increase in the activity of the AO with temperature.32,43
The literature suggests that favipiravir is a well-tolerated drug. 32 The most frequently reported adverse effects of favipiravir when used for influenza treatment, are mild to moderate diarrhea, asymptomatic increase of blood uric acid and transaminases, and a decrease in the neutrophil count. 29 In a study evaluating the inhibition properties of favipiravir against human and mouse norovirus RNA polymerases, it was found that favipiravir ribonucleoside triphosphate was recognized as a substrate of the human mitochondrial RNA polymerase, but did not result in inhibition of the DNA-dependent RNA polymerase nor cause mitochondrial toxicity in cells.32,40 Despite good tolerance observed, a major concern to safety of clinical favipiravir use is related to its teratogenic tendencies. In studies with fetal/embryo models of multiple animal species, teratogenicity was observed across all. 44 The exposure dosage causing teratogenicity was comparable with the proposed human use dosage. Therefore, it is strongly recommended that favipiravir not be administered to pregnant or possibly pregnant individuals.29,44 Due to this high risk of teratogenicity and embryotoxicity, favipiravir is conditionally marketed with strict regulation in Japan. 32 Hence the clinical use of favipiravir is restricted to novel or re-emerging influenza viruses, only when that virus is resistant to other influenza antivirals, while being manufactured and distributed only upon request by the Minister of Health, Labor and Welfare in Japan.29,32
Use in influenza
Early literature on favipiravir dates to 2001. Also known as T-705, favipiravir was tested in vitro for its antiviral properties against Influenza A, B, and C, against all of which it was found effective. It was also reported to have activity against oseltamivir and amantadine-resistant Influenza A. The Influenza A viral strains originally studied included H1N1, H2N2, and H3N2. 45 Selective viral RNA polymerase inhibition without inhibition of cellular RNA or DNA synthesis was reported as its proposed mechanism of action. 36 Takahashi et al. 46 reported that T-705 retained its efficacy against influenza-infected mice when compared with oseltamivir despite a delay of treatment initiation of up to 25-h post infection. Sidwell et al. 47 reported activity of T-705 against mice infected with avian H5N1 influenza. Antiviral drug regimens studied in mice yielded statistically significant protection against death at doses of or higher than 30 mg/kg/day given twice a day for 5 days. The effect of delaying therapy by up to 72 h after infection was also studied and Furuta et al. reported that T-705 retained its antiviral property in protecting mice against death at doses of 300 mg/kg/day given every 6 h for 5 days.41,48 Favipiravir resistance was first reported by Goldhill et al. 49 who stated that a K229R mutation in RdRp would confer drug resistance to favipiravir among pandemic 2009 H1N1 Influenza A viral strains. In one study, the combination of favipiravir with oseltamivir showed synergy at low doses in animal models infected with H1N1, H3N2, and H5N1 Influenza A viral strains. 50 Wang et al. 51 found accelerated clinical recovery among patients with severe Influenza on favipiravir and oseltamivir combination therapy compared with oseltamivir alone.
The approved favipiravir drug regimen in Japan for the treatment of Influenza is 1600 mg (loading doses) on day 1 followed by 600 mg twice a day, with the total duration of therapy being 5 days.29,52 Other experimental clinical studies in influenza53–56 used a regimen of 1800 mg (loading doses) followed by 800 mg twice a day, for a total duration of therapy of 5 days. Evidence from clinical trials assessing over 2000 patients suggests that favipiravir is well-tolerated.51,53–56 Adverse drug reactions reported include elevation in serum uric acid levels, diarrhea, elevation of liver enzymes, and reduction in neutrophil count. 52
Use in other viral diseases
Viral hemorrhagic fevers
The causative agents of viral hemorrhagic fevers (VHFs) belong to Arenaviridae, Bunyaviridae, Filoviridae, and Flaviviridae families of viruses, all of which are RNA viruses. Prominent VHFs caused by these viruses include Ebola viral disease and Yellow Fever among others. Favipiravir was trialed in rural Guinea during the Ebola virus disease (EVD) outbreak in 2014 as a multicenter proof-of-concept non-comparative trial. Nuanced conclusions were drawn about the efficacy of favipiravir as the trial was nonrandomized and all study participants received the drug given the public health crisis at the time. The authors reported that although favipiravir monotherapy may not be effective in patients with very high viremia, its clinical utility in intermediate to high viremia would merit investigation. 57 Another retrospective observational study on outcomes of patients treated with compassionate use favipiravir versus untreated patients showed a lower-case fatality ratio among those treated with favipiravir thereby conferring survival benefit. 58 Translational research on the efficacy of favipiravir against EVD done in macaques showed survival benefit among the infected animals that received ⩾ 150 mg/kg of favipiravir. The authors observed inhibition of viral replication inhibition in a concentration-dependent manner and concluded that favipiravir plasma trough concentrations > 70–80 μg/ml were linked to lower viral loads and improved survival. 59
Favipiravir has been tested in vitro against other etiological agents of VHFs including Bunyaviridae and Arenaviridae. Gowen et al. 60 studied the in vitro inhibitory effects of favipiravir (T-705) and ribavirin in monkey kidney Vero 76 cells against La Crosse virus, Punta Toro virus, sandfly fever virus, and rift valley fever virus (Bunyaviruses) and found that the drug inhibited the growth of the tested viral strains and was less toxic than ribavirin. The same authors examined the in vitro activity of favipiravir (T-705) against Junin virus, Pichinde virus, and Tacaribe virus (Arenaviruses) and found that the drug was highly active against the tested viral strains in cell cultures. The drug also afforded protection to hamsters infected with Pichinde virus and mice infected with Punta Toro virus.
Yellow fever is a VHF caused by the yellow fever virus (YFV), a flavivirus. The YFV distribution runs through tropical and subtropical Africa and South America. Clinical disease could be asymptomatic or may manifest with fever, chills, headache, myalgia, jaundice, bleeding, shock, and organ failure. The mortality rate of those with severe symptomatic disease can be > 30%. Julander et al. found T-705 to be moderately effective against YFV in cell culture. It was also found to be an effective treatment in YFV infected hamsters conferring survival benefit among the infected animals treated with T-705. 61
West Nile Virus
West Nile Virus (WNV) is a vector-borne (mosquito) disease caused by the West Nile Virus, a flavivirus. The spectrum of disease can vary from asymptomatic infection to mild febrile illness to severe viral meningitis or encephalitis. To date, there is no approved antiviral for the treatment of WNV. Morrey et al. studied the efficacy of orally administered favipiravir (T-705) among rodents infected with WNV and found the drug to be active against WNV. The drug’s lack of activity past the second day on viral infection was attributed to either the lack of a standard drug regimen or insufficient bioavailability in the brain or lack of neuronal metabolism to convert favipiravir to T-705 RTP. 62
Nipah virus
Nipah virus is an emerging zoonotic infection caused by the Nipah virus which belongs to the Paramyxoviridae family of viruses. Outbreaks have been reported out of Malaysia, Bangladesh, and India periodically. Fruit bats are its natural reservoir, and the virus can be transmitted to humans either from bats or via an intermediate host such as pigs or via human-to-human transmission. Clinically, the disease manifests as viral encephalitis with features of respiratory compromise. To date, there is no approved treatment or vaccine for Nipah virus. The disease has a high mortality rate, ranging upward of 40%. 63 Favipiravir has shown in vitro activity against vero cells infected with Nipah virus and prevented viral replication. 64 Dawes et al. 64 also found benefit of favipiravir administration among hamsters infected with Nipah virus and reported that treated hamsters infected with the virus did not develop any signs of clinical disease.
Respiratory viral diseases (other than influenza and COVID-19)
Human metapneumovirus (hMPV) and RSV, previously classified under Paramyxoviridae, belong to the family Pneumoviridae and can cause upper or lower respiratory tract disease in humans. Parainfluenza virus can cause similar disease and belongs to the Paramyxoviridae family of viruses. Favipiravir (T-705) demonstrated activity against all these viruses in vitro in a study done by Jochmans et al. The authors also reported in vivo drug activity in hamsters infected with hMPV. 65
Use in COVID-19
Early genomic sequencing of SARS-CoV-2 virion suggested over 90% homology, across several essential enzymes, with other coronaviruses, particularly those causing SARS and MERS. 66 In a quest for identifying effective therapy amid a catastrophic global pandemic, this knowledge helped trigger the ‘repurposing’ of multiple antiviral drugs including broad-spectrum antivirals and more specifically, drugs previously directed toward therapy of SARS, MERS, and other viral infections. The mechanism of action of favipiravir against SARS-CoV-2 is similar to that previously described in literature. After viral incorporation of T-705 RTP by RdRp, the nascent coronaviral RNA undergoes slowed RNA synthesis, chain termination, and viral mutagenesis, while evading the viral RNA repair mechanism. The SARS-CoV-2 RdRp has been described to have 10-fold higher activity than other viral counterparts, while simultaneously being prone to high nucleotide incorporation and error rates. 67 These processes significantly bottleneck the RNA replication by causing nucleotide shifts in an unbalanced viral environment with already low cytosine levels. 67 These critical hallmarks of the SARS-CoV-2 virion machinery make it vulnerable to RdRp inhibitors.
Alongside an effective vaccine, antivirals have a critical role in containing local spread of infection by curtailing viral load and shedding, at an early infection stage. 68 Studies suggest viral load in the upper and lower respiratory tracts in patients with mild infection peak in the early stage of infection, days 4 and 6, respectively, while in moderate-severely infected patients they peak in later stages, days 8 and 11. 69 Thus, the role of antivirals like favipiravir may be higher in mild-moderate infections at an early stage of the disease, to control the viral load, shedding, and infectivity rates, 70 to help reduce the burden of hospitalization and associated patient care on an already overwhelmed system.
An early study (February 2020) showed that favipiravir at higher concentrations (EC50 = 61.88 μM) was able to minimize viral infection in vero E6 cells in vitro. 71 While these in vitro studies suggested a need for further evaluation, the efficacy of favipiravir in patients infected with COVID-19 was initially assessed through two separate clinical trials in China (February 2020). 72 The inclusion criteria for both the trials included patients within the early stage of disease, from manifestation of symptoms and positive test result with reverse transcription polymerase chain reaction (RT-PCR), and patients with severe disease were excluded. In one of the trials, patients with COVID-19 were treated with a combination of favipiravir and alpha interferon (n = 30), while the other treatment arm was treated with lopinavir and ritonavir combination with alpha interferon. 72 The second clinical trial assessed the efficacy of favipiravir against therapy with baloxavir marboxil. 72 In addition, after initial approval of favipiravir for treatment of COVID-19 in China (February 2020), another study with 80 patients showed it had promise as an antiviral therapeutic, with lower side effects when compared with the lopinavir/ritonavir treatment arm. 73 While these initial studies showed some favorable results, there were safety concerns for use due to side effects like teratogenicity, prolongation of QTc interval and hyperuricemia as evidenced in use for other pathologies. 74 Interestingly, in a randomized controlled trial conducted on patients to receive either favipiravir or arbidol, with a primary outcome for recovery on day 7, favipiravir did improve latency to relief of cough and fever but did not improve clinical recovery rate, while the most frequently observed side effect was hyperuricemia. 75
Subsequently, other studies have been conducted to understand the efficacy of favipiravir in COVID-19. Studies have suggested that favipiravir could lead to viral clearance by day 7 and improve clinical outcome by 2 weeks when administered in early stages of infection.76,77 In one study, the median time to viral clearance was about 12.8 days in patients when favipiravir therapy was initiated on day 1, and increased to 17.8 days when therapy was started on day 6. 78 In addition, there were significant differences in duration of hospitalization, with need for oxygenation and mechanical ventilation, in patients with mild or asymptomatic infection when favipiravir therapy initiated late stage versus early. Thus, it may be important to initiate favipiravir therapy at an early stage of disease in asymptomatic or mildly infected COVID-19 patients, to achieve reduction in viral load and disease progression.76,77 Importantly, dosing regimens could significantly change the clinical outcome of the patient, lower doses indicating to have lower association with better outcomes. 76 Comparison of multiple trials suggests that favipiravir may not have a significant beneficial effect on improving patient mortality rate in subjects with mild to moderate COVID-19, and this may be associated with the timeline of therapy initiation. 77 However, it is necessary to assess the favipiravir therapy initiation timeline, dosage, duration, and safety through trials with larger sample size.
The use of favipiravir on a compassionate or approved basis for the indication of COVID-19 treatment has been put through clinical trials across the globe. Table 2 summarizes key published clinical trials (including from preprint servers) to date. The drug was trialed in cases of asymptomatic and mild-moderate disease as well as in moderate-severe cases of COVID-19 pneumonia. While most trialed a regimen of 1600 mg loading dose (two doses) on day 1 followed by 600 mg twice daily, other regimens used 1800 mg loading dose (two doses) followed by 800 mg twice a day. The length of drug therapy with favipiravir was varied and ranged from 7 to 14 days. At the present time, favipiravir is not approved for use in COVID-19 by the United States Food and Drug Administration or its European counterpart, the European Medicines Agency. The formally recommended dose and duration of therapy remain awaited based on results of the ongoing clinical trials. However, it is noteworthy that 600 mg twice daily maintenance dose has been used to manage COVID-19 in some international markets. 79 Doi et al. studied the effect of early versus late favipiravir use among adolescents and adults with asymptomatic or mild COVID-19 and noted that viral clearance by day 6, which was their primary endpoint, was similar between the two groups. Secondary and exploratory endpoints, that is, viral load reduction by day 6 and time to defervescence were met in the early treatment arm. 80 Another group of researchers who studied the drug’s efficacy versus supportive care alone, among patients with mild to moderate COVID-19, found shorter time to cessation of viral shedding with favipiravir but this was not statistically significant. The median time to clinical cure among symptomatic patients at baseline was reportedly significantly faster with favipiravir. 81 Ivashchenko et al. observed statistically significant differences between favipiravir treatment groups compared with standard of care at the time (hydroxychloroquine or chloroquine or lopinavir/ritonavir); in terms of viral PCR clearance, Cai et al. suggested favorable radiographic outcomes in the favipiravir treatment arm compared with control (lopinaivr/ritonavir) in addition to shorter median time for viral clearance.82,83 The optimal dosages and duration of drug therapy with favipiravir for COVID-19 remain indefinite. Further clinical trials with specific aims to guide these aspects of treatment are warranted.
Summary of published (including preprint) literature from favipiravir clinical trials to date.
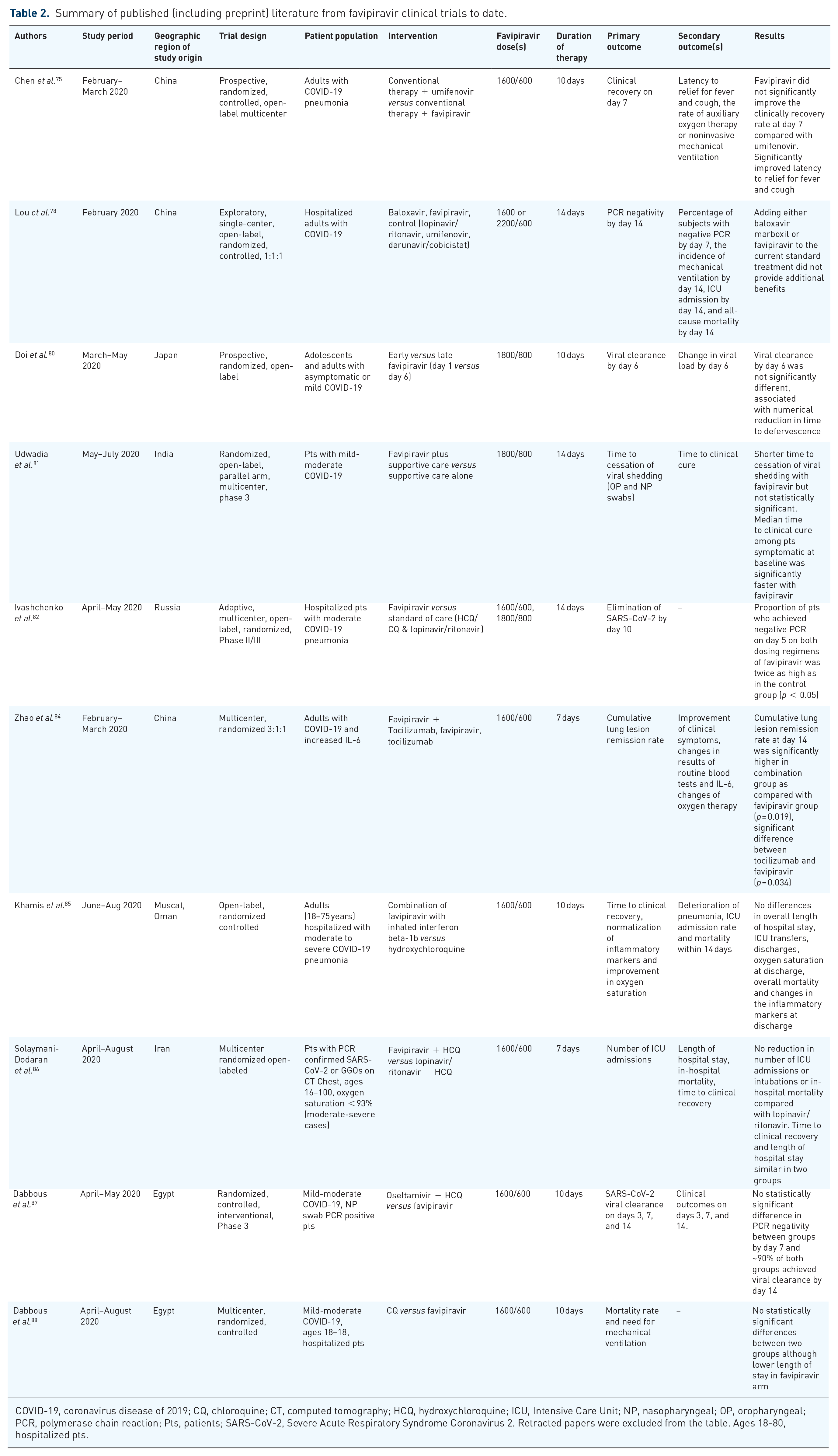
COVID-19, coronavirus disease of 2019; CQ, chloroquine; CT, computed tomography; HCQ, hydroxychloroquine; ICU, Intensive Care Unit; NP, nasopharyngeal; OP, oropharyngeal; PCR, polymerase chain reaction; Pts, patients; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2. Retracted papers were excluded from the table. Ages 18-80, hospitalized pts.
Future directions
Table 3 summarizes publicly available information about ongoing favipiravir clinical trials.89–95 The GETAFIX, FLARE, COVERAGE, and VIRCO trials are focused on drug efficacy early in the treatment of COVID-19 and the COVERAGE trial will be looking specifically at geriatric patients. The PRINCIPLE trial collaborative group evaluated the use of azithromycin among adults 50 years of age or more with medical comorbidities and all adults above 65 years of age with COVID-19 and found that its use did not shorten the time to clinical recovery or reduce the risk of hospitalization. 96 Interim results of the PRINCIPLE trial also reported clinical utility of inhaled budesonide among patients with COVID-19 at risk for adverse outcomes. 97 The findings from the PRINCIPLE trial about favipiravir’s clinical utility remain awaited. Bosaeed et al. 89 have proposed a multicentric randomized controlled trial to evaluate efficacy of favipiravir and hydroxychloroquine combination in comparison with control. Hassaniazad et al. 90 also published about an upcoming single-center, randomized, open-label clinical trial among moderately ill patients with COVID-19 evaluating the safety and efficacy of favipiravir and interferon beta-1a combination in comparison with lopinavir/ritonavir and interferon beta-1 combination.
Summary of ongoing favipiravir clinical trials.
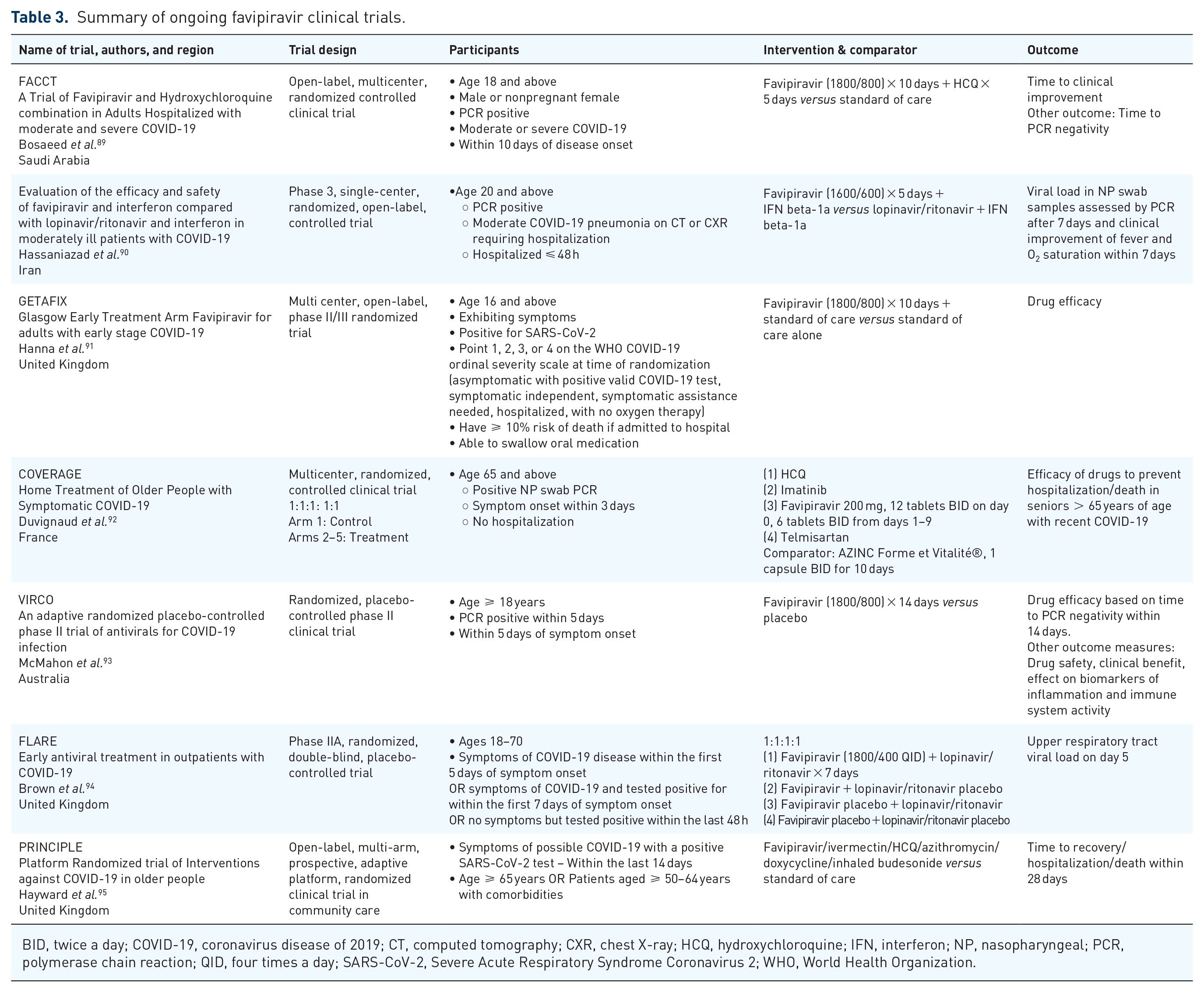
BID, twice a day; COVID-19, coronavirus disease of 2019; CT, computed tomography; CXR, chest X-ray; HCQ, hydroxychloroquine; IFN, interferon; NP, nasopharyngeal; PCR, polymerase chain reaction; QID, four times a day; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; WHO, World Health Organization.
Conclusion
Favipiravir, among other drugs, has gained prominence since 2020 because of the COVID-19 pandemic and its versatility as a broad-spectrum antiviral that inhibits RdRp and targets viral replication. While its utility has shown benefit in a few clinical trials, others yielded mixed results. The drug’s full potential as a therapy for COVID-19 remains to be determined, including its optimal timing of administration, dosage, and duration of therapy. It is fairly well-tolerated with a major safety concern being its teratogenic potential. Adverse drug reactions among patients included hyperuricemia, QTc interval prolongation, and elevation in hepatic enzymes. Finally, favipiravir’s prospect as a post-exposure prophylactic agent in COVID-19 remains to be tested.
Footnotes
Author contributions
KS: Conceptualiztion, manuscript preparation, review and editing.
MR: Conceptualization, manuscript preparation, review, editing and submission.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.