
Abstract
Background:
The aim of this study was to assess whether daptomycin is safer and more efficacious than comparators for the treatment of serious infection caused by gram-positive microorganisms.
Methods:
Electronic databases (Medline, EMBASE, the Cochrane Central Register of Controlled Trials and clinical registered trials) were searched to identify randomized controlled trials (RCTs) that assessed the efficacy and safety of daptomycin versus therapy with any other antibiotic comparator. Two reviewers independently applied selection criteria, performed a quality assessment and extracted the data. Heterogeneity was assessed, and a random-effects or fixed-effects model, when appropriate, was used for estimates of risk ratio (RR). The primary outcome assessed was the risk of clinical treatment failure among the intention-to-treat population and the presence of any treatment related adverse event (AEs).
Results:
A total of seven trials fulfilled the inclusion criteria. Daptomycin treatment failure rates were no different to comparator regimens (RR = 0.96; CI 95% 0.86–1.06). No significantly different treatment related AEs were identified when comparing groups (RR = 0.91; CI 95% 0.83–1.01).
Conclusions:
No significant differences in treatment failure rates and safety were found using daptomycin or any of the comparators treatment.
Introduction
Antibiotic resistance is steadily increasing, creating a growing worldwide health problem. Methicillin-resistant Staphylococcus aureus (MRSA) has emerged as a common cause of complicated skin infections, bacteremia, endocarditis, and pneumonia. 1
Vancomycin remains the first treatment option in patients with invasive MRSA infections, but its renal toxicities, narrow spectrum, and low concentration in some tissues has led to the need for new treatment alternatives.1,2 In addition, the emergence of vancomycin-resistant enterococci (VRE) as a cause of nosocomial infections is a current concern, raising the need for new antibiotic options.
Daptomycin is a lipopeptide antibiotic with a broad spectrum of activity against clinically relevant gram-positive bacteria, including S. aureus regardless of methicillin susceptibility. In addition, it demonstrates significant activity against VRE. Given the possibility of once-a-day administration and its safety profile, daptomycin is considered a good option to complete treatment in the ambulatory setting. 3
Daptomycin is approved by the Food and Drug Administration in adults for skin and soft tissues complicated infections (cSSI) and infectious right-side endocarditis. This drug is not indicated for the treatment of pneumonia because it binds to the pulmonary surfactant and loses activity3–5 Detailed descriptions of its use remain limited particularly in children. 2
Taking into account the previous statements, the following clinical question can be raised: Is daptomycin an effective and safe option for gram-positive infections?
To answer this question the authors developed the present systematic review and meta-analysis to evaluate daptomycin’s risk of treatment failure and treatment related adverse events (AEs) compared with the standard of care (SOC).
Material and methods
A literature search was conducted in EMBASE, Medline, and the Cochrane Central Register of Controlled Trials and clinical registered trials databases using the search terms ‘daptomycin’ with the following filters: clinical trial, review, comparative study, systematic reviews, randomized controlled trial (RCT), controlled clinical trial, practice guideline, meta-analysis and guidelines, and use in human studies. Articles published in English, Spanish, or French until September 2018 were reviewed. The reference lists in the reviewed articles were manually examined for additional relevant studies (Table 1). The efficacy end-point was treatment failure. We used this criterion because it is the main concern at the moment for antibiotics prescription. The safety end-point was any AE that was treatment related.
Included studies’ main characteristics.
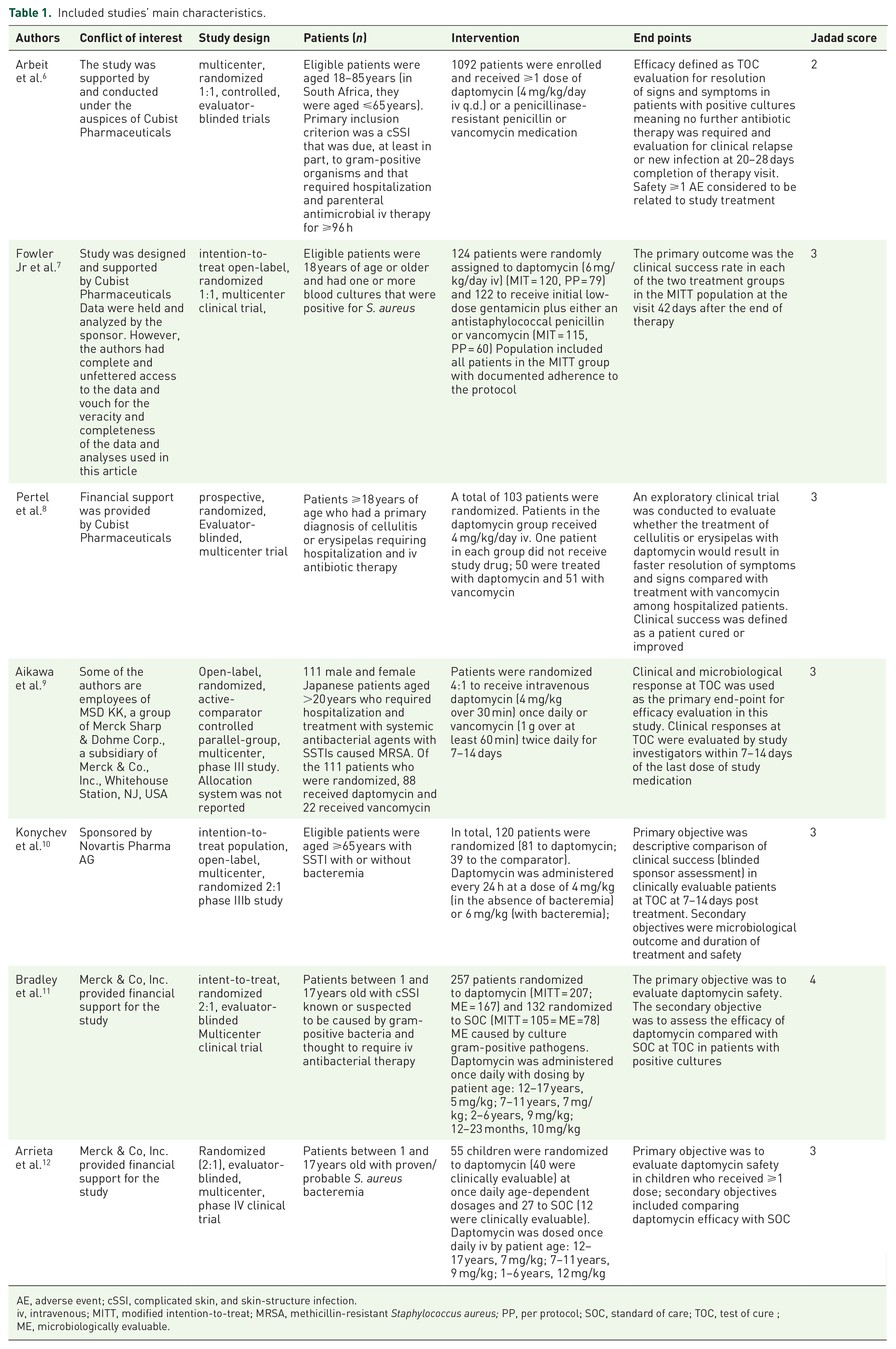
AE, adverse event; cSSI, complicated skin, and skin-structure infection.
iv, intravenous; MITT, modified intention-to-treat; MRSA, methicillin-resistant Staphylococcus aureus; PP, per protocol; SOC, standard of care; TOC, test of cure ; ME, microbiologically evaluable.
Study selection
Data extraction and qualitative assessment were performed by two reviewers (MTR and DB) who independently appraised the literature and considered only RCTs for further assessment. In case of disagreement, a third reviewer (RL) analyzed the data and managed the scientific discussion until consensus was reached.
A study qualified if it was a RCT, and it compared the efficacy and safety of daptomycin with other antibacterial agents or placebo. Trials were included regardless of being blinded or open-label. The methodological quality of the included studies was assessed with the Jadad scale. 13 Trials scoring ⩾2 were considered for evaluation.
Data analysis and statistical methods
The risk of therapeutic failure end points was based on intention-to-treat or modified intention-to-treat (MITT), that included only patients with documented S. aureus infection or other selected specifications by authors and we determine relative risk based on this appropriate measure. In order to be more conservative pooled risk ratio (RR) and 95% confidence intervals (CIs) were calculated for failure and safety outcomes using the random-effects model (DerSimonian-Laird), calculations were carried out using the meta-analysis calculator by EpiData software version 3.1, Geneva, Switzerland (WHO). Heterogeneity bias was estimated using the Q test. Potential publication bias was estimated using Egger’s test. The null hypothesis was rejected if p < 0.05. The systematic review was carried out using the Preferred Reporting Items for Systematic Reviews Statement. 14
Results
The literature search identified a total of 566 potentially relevant articles, a total of 64 were RCTs and were initially evaluated by screening of the title and abstract. A total of 57 RCT studies were excluded because they did not meet the inclusion criteria, were duplications, or new analysis of previously published studies. (Figure 1)

Flow diagram of the identification process and selection of the included articles.
Included studies and main characteristics
Finally, 7 full-text articles including 1798 patients under analysis for therapeutic failure rates were selected to be included in this systematic review and fully analyzed.6–12 Two out of the seven studies included were carried out in a pediatric population9,11 (one for treatment of bacteremia 11 and one for microbiologically documented skin infections 9 ), five were carried out in adult patients (four for skin infections) and one for the treatment of bacteremia and endocarditis. Table 1 summarizes the main characteristics of included articles.
Comments about included studies
Arbeit and colleagues 6 studied the safety and efficacy of daptomycin versus the standard of care (SOC) for treatment of microbiologically documented cSSI and concluded that daptomycin was similar and comparable with conventional therapy. Frequency and severity of AEs were similar in both groups, with gastrointestinal disorders being the most commonly reported AEs.
The trial carried out by Fowler and colleagues 7 supported the efficacy of daptomycin in adults with bacteremia and endocarditis caused by S. aureus. This study was not able to identify a statistically significant difference when compared with standard treatment. Rates of AEs were similar between daptomycin and standard therapy. Renal impairment was more common in patients who received standard therapy and creatine kinase elevation was significantly more common in the daptomycin group.
Pertel and colleagues 8 reported a similar clinical response and AEs rates between daptomycin versus vancomycin comparator in adults with cSSI mainly in erysipelas and cellulitis.
Kornychev and colleagues 10 analyzed the efficacy and safety of daptomycin in adult patients with cSSIs reporting no significant clinical failures in the daptomycin group. Incidence rates of AEs were similar in both groups.
Aikawa and colleagues 9 studied the efficacy and safety of daptomycin versus comparators in Japanese patients with MRSA cSSI infections and concluded that daptomycin was clinically and microbiologically effective. AEs occurred with similar frequency in patients treated with daptomycin or vancomycin.
Pediatric patient trials carried out by Bradley and colleagues 11 and Arrieta and colleagues 12 were also included (one in patients with bacteremia and one in patients with microbiologically documented cSSI). Daptomycin performance in both trials was no different from comparators and the rate of any reported AEs were not statistically significant different between groups (Tables 1–3).
Studies’ efficacy end-point: therapeutic failure.

Studies’ safety (at least one adverse event).

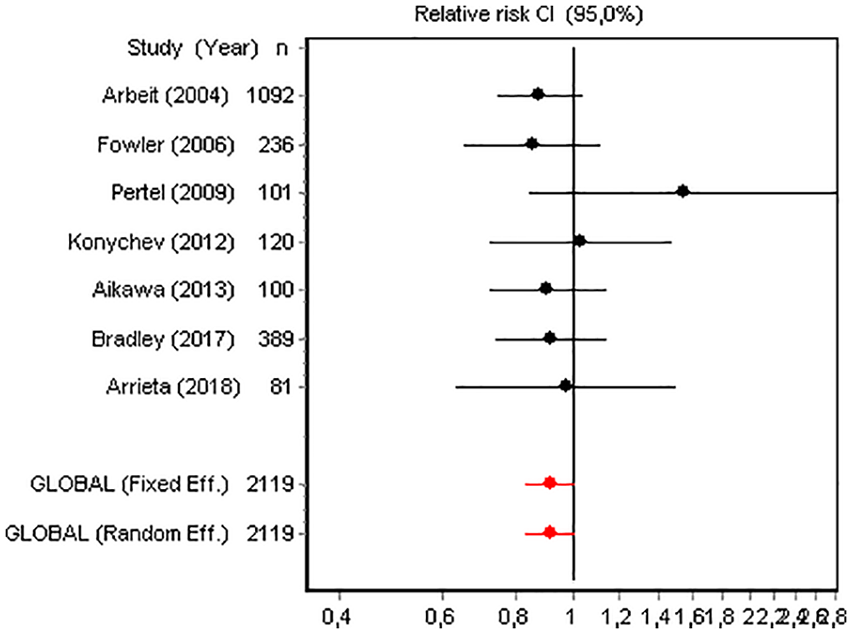
Therapeutic failures rate, no heterogeneity in trials ‘results for therapeutic failure were detected’ (heterogeneity bias: DerSimonian-Laird’s test: Q: 1.12; df: 5; p = 0.95). Typical RR for therapeutic failure was RR 0.96; CI 95% 0.86–1.06 (Figure 2). The cumulative meta-analysis shows a persistent but nonsignificant direction and magnitude of the therapeutic failure rate. Consistency is according with the homogeneity of included trials results (Figure 3). Sensitivity analysis did not demonstrate any relevant result modification [withdrawal of Arbeit’s study reduced risk by 3.94% (the highest) and Aikawa’s study 0.02% (the least)]. Egger’s test yielded a significant probability of publication bias for treatment failure: t = 5.11; df = 5; p = 0.003 (Figure 5).

Forest plot about probability of therapeutic failure.

Cumulative probability of therapeutic failure.
Treatment related AEs rate: Rates of treatment related AEs were not different between daptomycin and comparators (typical RR 0.91; CI 95% 0.83–1.01) (Figure 4). No heterogeneity was detected (heterogeneity bias: DerSimonian-Laird’s test: Q = 3.90; df = 6; p = 0.67).
Forest plot about the probability of adverse events.
The most frequently reported AEs were gastrointestinal disturbances in all groups. It is well known that a creatine phosphokinase (CPK) level increase is considered a subrogate index of muscle toxicity 7 All of the trials included paid special attention to this topic, in a very heterogeneous way, making its synthesis not advisable by means of a meta-analysis. We present these observations in Table 4.
Drug-related CPK elevations.

CPK, creatine phosphokinase; SOC, standard of care.
Sensitivity analysis did not highlight any relevant result modification (withdrawing Arbeit’s paper reduced risk by 2.27% (the highest) and withdrawing Pertel’s paper reduced risk by −1.38%). Egger’s test yielded a significant probability of publication bias: t = 3.23; df = 5; p = 0.02. (Figure 5)

Publication bias in therapeutic failure assessment.
Discussion
We conducted this systematic review to evaluate the performance of daptomycin, in terms of safety and risk of therapeutic failure, when it was prescribed for the treatment of all types of infections (except pneumonia) in children and adults, against the usual therapy antibiotic comparators.
A nonsignificant trend for less risk of therapeutic failures of daptomycin in patients with cSSI, endocarditis, or bacteremia was demonstrated in the clinical trials included in this meta-analysis, especially for those caused by S. aureus. All RCTs included in this systematic review suggested this trend, both in adults and children suffering complicated skin infections, bacteremia, or endocarditis. This meta-analysis achieved the same conclusion.
With regard to AEs, daptomycin had been reported to have the potential to cause muscle toxicity, therefore, CPK levels were measured in all included studies.
Some studies showed that high doses of daptomycin may elevate CPK levels, however, in healthy volunteers doses up to 12 mg/kg/day were not associated with muscle toxicity and in one study carried out on patients treated with high doses (>6 mg/kg/day) of daptomycin, the rate of CPK elevations were low.1,15
Our meta-analysis showed that elevated CPK levels were more frequent in the daptomycin group, but discontinuation of the drug was seldom required due to this AE. In addition, in these patients, the elevated CPK levels dropped rapidly. No data is available about the long-term AEs related to its potential muscle toxicity because this follow-up was not carried out.
Given the similar risk of therapeutic failure of daptomycin, its low incidence of any AEs, and the potential to be used as monotherapy, there is support for its use as an alternative strategy to reduce the use of broad spectrum antibiotics. In addition, daptomycin administration once-a-day is an important therapy for use in ambulatory treatment in selected patients to reduce health care associated infection risk.
Emergence of antibiotic resistance is a major problem in health care and it is, therefore, very important to control the use of antibiotics. It is remarkable that daptomycin resistance is uncommon. In our setting, the daptomycin price per 500 mg is 10 times higher than the price of 500 mg of vancomycin. If the need of vancomycin and the potential risk of renal failure is considered, economical concerns should be balanced against the benefits in selected cases, especially in an endovascular setting. A study, using a Monte Carlo simulation, shows that daptomycin was the most cost-effective treatment in 100% of the 10,000 simulations, with a willingness to pay €12,000 per additional cure (the approximate cost of treatment for an MRSA bacteremia episode). This study concluded that daptomycin is more cost-effective than vancomycin when treating MRSA bacteremia and that the higher cost of daptomycin does not imply a higher cost of treatment for this infection. 16
Daptomycin should potentially be reserved for intolerance, or when the narrower spectrum antibiotics fail, especially when targeted against MRSA and VRE in selected infections.
A limitation of the present meta-analysis is that all of the RCTs included in this systematic review were funded by the pharmaceutical industry, resulting in a considerable risk of bias. Concerns arose when it was discovered that all of the funded RCT studies were only conducted in patients with cSSI infections, only a few were in patients with bacteremia or endocarditis, with different doses and follow-ups. For these reasons, we applied strict selection criteria in an effort to standardize our study, but this strategy does not allow for publication bias. Other limitation are that the microbiologically documented infections were caused in the majority of cases by S. aureus, and we cannot extrapolate the results to other gram-positive bacteria.
The authors concluded that to answer the initial clinical question further studies are required on other types of infections, comparing daptomycin with new antigram-positive pathogens and other gram-positive microorganisms, and with studies of cost versus efficacy.
Footnotes
Acknowledgements
All authors made substantial contributions to the design of the work; acquisition, analysis, and interpretation of data, and they contributed to the final drafting and all have approved the final version to be published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there are no conflicts of interest.