
Abstract
Background:
Secondary peritonitis, following intestinal perforation, constitutes a significant proportion of cases admitted as a surgical emergency and has a mortality rate of 6–21% worldwide. As a part of an antimicrobial stewardship program, we noted considerable variation among the choice of empirical regimens among such cases. Hence, we conducted a prospective study to generate the evidence for a rational empiric regimen for patients with secondary peritonitis following intestinal perforation.
Methods:
The study included a complete follow up of 77 cases of secondary peritonitis admitted during a 12 month period. The intraoperative fluid (peritoneal) sample of the patient was sent for culture and sensitivity pattern analysis.
Results:
The sites of perforation as seen in decreasing order were lower gastrointestinal (GI) (50.6%), upper GI (36.4%), and unclassified (13%). The most common organism found in the intraoperative fluid was Escherichia coli (47.9%) followed by Klebsiella pneumoniae (12.5%). amikacin, cefoperazone-sulbactam, piperacillin-tazobactam and imipenem were sensitive in 22 (out of 23 tested), 5 (out of 9), 13 (out of 13) and 22 (out of 22) isolates of E. coli and 3 (out of 6), 1 (out of 3), 4 (out of 6), 4 (out of 6) isolates of K. pneumoniae, respectively. The most common empirical antibiotic was cefoperazone-sulbactam (38.7%) followed by piperacillin-tazobactam (29.3%).
Conclusion:
Based on our prospective study, piperacillin-tazobactam or imipenem should be used empirically in patients presenting with complicated intra-abdominal infections secondary to perforated viscus, especially if they have sepsis or septic shock.
Keywords
Introduction
Complicated intra-abdominal infections with or without sepsis constitute an important category of patients reporting to our surgical emergency department. Perforation peritonitis, secondary to intestinal perforation, constitutes a significant proportion of these cases and is a surgical emergency with 6–21% mortality worldwide.1–3 It is a type of secondary peritonitis, where initial resuscitation followed by adequate surgery and good postoperative care is required for best outcomes.4,5 There is a difference in the demographics of the disease between the eastern and western world. The age group commonly affected with perforation peritonitis is the younger age group in the eastern world, whereas in the west, it is the older age group. 6 The segment of bowel involved is the proximal bowel more commonly than the distal in the eastern world.7,8 Though the incidence of infective perforations secondary to typhoid or tuberculosis is decreasing in the western world, it still remains a major concern in developing countries like India, and about 50% of the total perforations in India are secondary to infections, whereas infections constitute only 2–3% in the western world.9,10 Infective complications occurring after surgical repair are a major cause of the morbidity associated with perforation peritonitis. 5 Hence, drainage of the collections with administration of appropriate antibiotics, forms the core therapy in the postoperative period.
Peritoneal fluid sampling during surgery and assessment of the organism has been practiced over the years; 11 Even though the relevance of this has been questioned, such sampling allows the isolation of the infective organism and can guide postoperative antibiotic therapy. Escherichia coli is the most commonly isolated Gram-negative bacteria, whereas Bacteroides tops the list among the anaerobes.12–14 The empiric therapy used is a combination of aminoglycoside with clindamycin or metronidazole in the western world. Monotherapy with cefoxitin or ampicillin has also been used with good results. 11 Such empiric therapies are generally based on studies conducted by or on guidelines given by organisations such as the Infectious Diseases Society of America (IDSA).
IDSA guidelines give recommendations for antimicrobial use in the management of complicated intra-abdominal infection. 15 However, we as a part of our antimicrobial stewardship program, noted considerable variation among the choice of empirical regimen for different cases of perforation peritonitis. There was also a lack of available policies for these cases that led to overuse or the unnecessary use of antibiotics. 16 Further, we suspected that culture sensitivity patterns involved pathogens which may warrant consideration of different empiric antibiotic regimen. The present study was conducted to assess the profile of features in patients with secondary intra-abdominal infections due to peritoneal perforation with or without sepsis, with a view of proposing appropriate empiric antibiotic regimens. The study also serves as evidence-based support for surgeons in making decisions on the empiric regimen to be given in secondary peritonitis following intestinal perforation.
Methods
The study was approved by the Institutional Ethics Committee of the Institute (approval number NK/1798/Study/2135) and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments and local national guidelines. The study was undertaken in a tertiary care hospital (Postgraduate Institute of Medical Education and Research, Chandigarh) located in northern India. Adult patients of either sex reporting to the surgical emergency were screened for potential eligibility. As the study did not involve any direct intervention, written informed consent from the patient was not required.
Eligibility criteria of the study
The inclusion criteria for the study were: (1) Adult patients of either sex presenting with abdominal sepsis; (2) Patients who had confirmed hollow viscus perforation by ultrasonography or computed tomography (CT) scan; and (3) Patients in whom the samples were collected and cultured from the abdomen during surgery. The exclusion criteria were: (1) Patients of hollow viscus perforation in whom the surgery was not performed; (2) Children <12 years of age; and (3) Patients who had abdominal sepsis without hollow viscus perforation
Study design
The patients were followed up for their entire period of stay in the hospital. The duration of stay of the patients at different levels of care was noted. The level of care in which the patients stayed were divided into three levels namely level 1, level 2 and level 3. Level 3 corresponds to the intensive care unit in routine hospital setting and facilities for emergency ventilation are available. All the patients included in the study had at least 1 day in level 3 care. Level 2 represents a step-down facility and level 1 represents the inpatient ward in hospital. Standard definitions for the concomitant presence of sepsis and septic shock were used. 17
Sample collection and analysis
The procedure followed for collecting intraoperative samples were as follows. Peritoneal fluid was aspirated using a sterile syringe under strict aseptic precautions and then transferred to a sterile container. The specimen was sent for microbiological examination and results were followed up. Briefly, the peritoneal fluid was inoculated on routine microbiological media (sheep blood agar, MacKonkey agar and Robertson’s cooked meat broth) and incubated aerobically at 37°C overnight. Next day, the plates were observed for bacterial/fungal growth and isolated colonies from morphologically distinct growth were identified by MALDI-TOF MS (Bruker Daltoniks, Bremen, Germany). In a few cases, peritoneal fluid was directly inoculated to Bactec bottles and incubated in automated systems. For blood culture, 8–10 ml of the blood sample was inoculated in Bactec bottles and inserted into an automated system for closed continuous monitoring. Once a positive beep was obtained from the Bactec 9240 (Becton Dickinson, New Jersey, U.S.A), a drop of broth from the culture bottle was inoculated onto routine culture media and processed as described before. Once the organism/organisms were identified, antimicrobial susceptibility was performed using the Kirby–Bauer disk diffusion method in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines for designating an organism as sensitive, intermediate and resistant. 18
Outcome definition
If a patient had been operated more than once during the stay in hospital, then the intraoperative sample was collected and evaluated at each surgical intervention and samples of the same patient were reported as separate entity in the study. This was referred with the term ‘unique surgery events’ as the surgical intervention was taken as a factor for discriminating and identifying the samples. In addition to classifying an organism as sensitive, intermediate and resistant, the organisms were further classified to identify the predominant organism in the upper and lower GI tract perforation peritonitis. A match was made to assess whether the organism in the intraoperative fluid of a patient was found subsequently in the patient’s blood culture.
The details of the antibiotic administered during the entire duration of stay was noted. For a patient referred from another healthcare setting, an attempt was made to obtain the details of culture and its sensitivity report, antimicrobials received and the intervention performed.
The final outcome was classified as discharged, death or leave against medical advice (LAMA). LAMA represents those patients that required treatment and hospitalization but were discharged from the hospital against medical advice. This being a pilot study, a convenient sample size of 77 was taken.
Statistical analysis
Statistical analysis was carried out using R statistical software (version 3.4.1). 19 The figures were created using Adobe Illustrator CC 2018, Adobe Inc., U.S. The values were expressed as mean ± standard deviation (SD) for parametric data and median with range for nonparametric data. The frequency of events was represented as the number of events along with a percentage.
Results
The study was conducted between May 2015 and April 2016. A total of 77 cases were included in the study. Among the included cases, 59 (76.6%) were male and 18 (23.4%) were female. The mean age of the patients was 43.1 ± 18.9 years with a median of 45 years and range between 13 and 86 years. The mean age among the males and females admitted in the study was 41 ± 18.3 and 49.8 ± 19.8 years respectively.
The sites of perforation were categorized as upper GI tract, lower GI tract and unclassified perforation peritonitis categories. The upper GI tract perforation peritonitis was seen in 28 (36.4%) patients, lower GI tract perforation peritonitis was seen in 39 (50.6%) patients and 10 (13%) patients were classified as ‘unclassified’.
The frequency of different antibiotics started empirically in the patients are represented in figure 1.

Horizontal bar chart representing the frequency of different antibiotics started empirically in patients in the study. The ‘other’ category included those antibiotics whose frequency of administration to patients was less than three patients in the study. This encompassed ceftriaxone, cefoperazone, colistin, ciprofloxacin and amikacin. In 2 patients (out of 77), the data on the type of empirical antibiotic started was missing.
A total of 80 unique surgery events were considered in the study. Out of the 80 events, the intraoperative fluid was sterile in 12 (15%), had a single bacterium in 32 (40%), two bacteria in 5 (6.2%), three bacteria in 1 (1.2%), fungus in 1 (1.2%) and both bacteria and fungus in 1 (1.2%). The remaining events were categorized under ‘others’ 28 (35%). This consisted of those events in which intraoperative fluid could not be obtained, such as those patients with sealed perforation peritonitis, patients in whom conservative management was undertaken, patients in whom the intraoperative fluid on examination came with inconclusive results (contaminated or bacteria with doubtful significance) and those patients who were loss to follow up.
The most common organism which was seen among the positive intraoperative fluid was E. coli (n = 23, 47.9%). The second most common organism was Klebsiella pneumoniae (n = 6, 12.5%). The other organisms which were isolated from the culture include Enterococcus faecium (n = 3, 6.2%), Staphylococcus aureus (n = 3, 6.2%), Acinetobacter baumannii (n = 3, 6.2%), anaerobic bacteria (n = 3, 6.2%), Enterococcus faecalis (n = 2, 4.2%), yeast (n = 2, 4.2%), Pseudomonas aeruginosa (n = 1, 2.1%), Pseudomonas monterilli (n = 1, 2.1%) and alpha-haemolytic streptococci (n = 1, 2.1%).
Out of 23 intraoperative fluid samples which came positive for E. coli, 22 were sensitive to amikacin (total of 23 were tested and 1 was resistant), 5 were sensitive to cefoperazone-sulbactam (total of 9 were tested and 2 were intermediate sensitive and 2 were resistant), 13 were sensitive to piperacillin-tazobactam (total of 20 samples were tested and 3 were intermediate sensitive and 4 were resistant) and 22 were sensitive to imipenem (total of 23 samples were tested and 1 was resistant). Out of six intraoperative fluid samples which came positive for K. pneumoniae, three were sensitive to amikacin (total of six were tested and three were resistant), one was sensitive to cefoperazone-sulbactam (total of three were tested and two were resistant), four were sensitive to piperacillin-tazobactam (total of six were tested and two were resistant) and four were sensitive to imipenem (total of six were tested and two were resistant). All the three cultures that came back positive for E. faecium and S. aureus were sensitive to both vancomycin and teicoplanin.
Table 1 represents the frequency of different organism according to the location of the perforation in the GI tract.
Frequency of the organism in upper GI, lower GI and unclassified perforation peritonitis. The percentage in brackets stands for the percentage frequency of organism under each category.

GI, gastrointestinal.
Out of 77 patients evaluated in the study, during the course of hospital stay, blood culture was positive in 13 (16.9%) patients. Among these 13 patients, a total of 29 different samples collected at different points of time during the stay in the hospital were positive. Out of these 29 positive samples, the predominant organism was A. baumannii (n = 6, 20.7%) samples and the second most common organism was Candida tropicalis (n = 5, 17.2%). Out of 13 patients found positive with blood culture, in only 2 (15%) patients, the organism (E. coli and S. aureus) that was found in the intraoperative fluid was subsequently found in the blood culture.
Out of all the patients evaluated in the study, 41 (53.2%) were discharged in an improved state, 25 (32.5%) died and 11 (14.3%) patients were LAMA from the hospital. The number of patients who stayed in level 3, level 2 and level 1 were 75 (97%), 41 (53%) and 38 (49%), respectively.
Table 2 represents the duration of stay at different level of care in the hospital shown against the outcome of the patient.
Mean duration of stays (in days) in different level of care shown against the outcome of the patient (discharge, death and LAMA). Data are represented as mean ± SD.
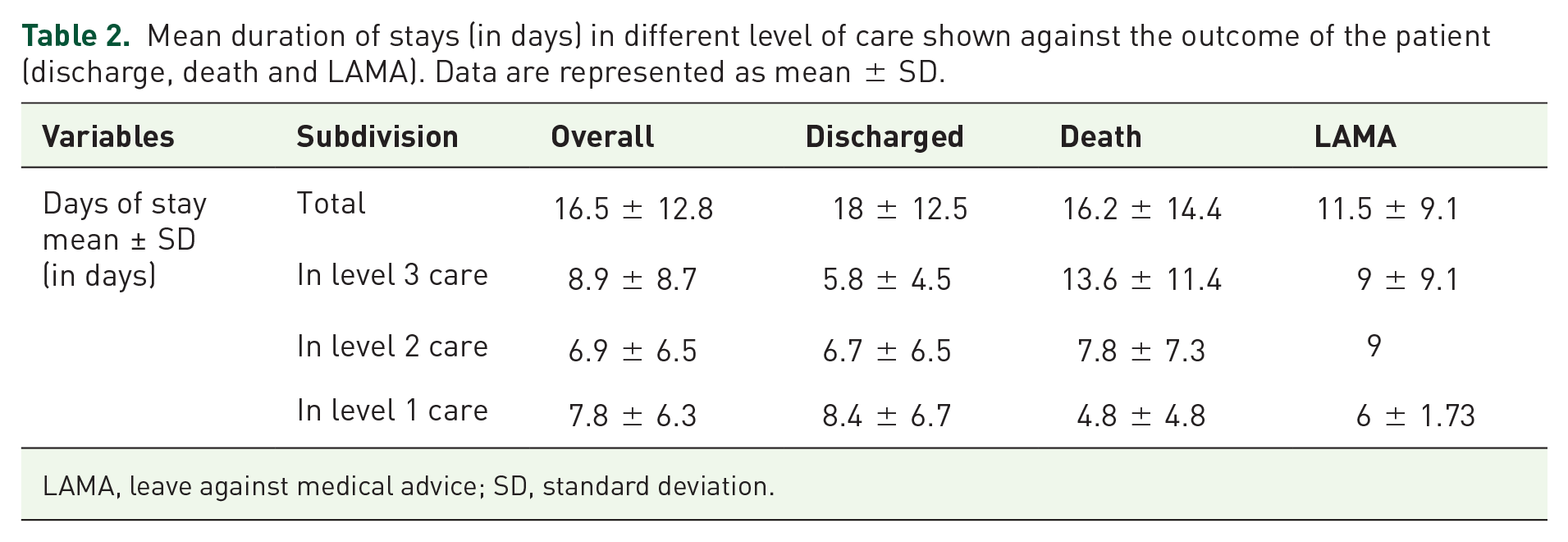
LAMA, leave against medical advice; SD, standard deviation.
Table 3 shows site of perforation, causes of perforation peritonitis and blood pressure at the time of admission in different outcome categories.
Site of perforation, causes of perforation peritonitis and BP at the time of admission in different outcome categories. The percentage in brackets stands for the percentage frequency of diagnosis, causes of perforation peritonitis and BP at the time of admission under each outcome category. The ‘others’ subdivision under the ‘site of perforation’ variable included those diagnostic categories for which the frequency of occurrence in the study were less than three patients and it encompassed caecal perforation peritonitis, oesophageal perforation peritonitis, sealed perforation peritonitis, gastric perforation peritonitis. The ‘others’ subdivision under ‘causes’ variable consists of iatrogenic injury, inflammatory bowel disease, neuroendocrine tumour of body of pancreas, ingestion of foreign body and stab injury.

BP, blood pressure; BTA, blunt trauma abdomen; LAMA, leave against medical advice.
Discussion
The study evaluated the cases of complicated intra-abdominal infections, associated with peritonitis secondary to perforation who were admitted to our hospital for treatment. The demographic profile of the patients with respect to sex (male predominance) and age (average age of 44 years) was similar to that seen in the previous studies. 20
The most common organism which was seen in the intraoperative fluid was E. coli followed by K. pneumoniae. One previously conducted study in which the bacteriology of intraoperative fluid following perforated appendicitis with peritonitis was examined has reported that E. coli and Bacteroides fragilis were present in almost all the samples examined. 21 The study further reported that the unusual high bacterial load which was found in the intraoperative fluid might be the reason for the therapeutic failures associated with patients with perforation. 21 Only the cases of secondary peritonitis following perforated appendicitis were considered in that study. In our study, patients with complicated intra-abdominal infection following perforated viscus with the site of perforation involving any segment of the GI tract were included.
The organisms were tested for sensitivity in accordance with the CLSI guidelines and this is the reason for them not being tested against all the antibiotics. Of the two organisms most commonly isolated, sensitivity to imipenem, amikacin and piperacillin-tazobactam was relatively preserved. On account of the possibility of pus collections and expected prolonged treatment, amikacin is not a choice initially for these patients but a decision has to be made between piperacillin-tazobactam and imipenem. It was further seen in the study that cefoperazone-sulbactam is the most commonly used empirical agent. But it has shown sensitivity to E. coli in only 5 (out of 23) cases. Moreover, the anaerobic activity of cefoperazone-sulbactam is not well established and is has to be given with a combination of metronidazole for covering the spectrum of anaerobes. 22 The anaerobic activity of piperacillin-tazobactam and imipenem is documented, and these two antibiotics need not be given with metronidazole.23–25 In certain settings, the routine prolonged use of cephalosporins is restricted to prevent the development of resistance. In only 2 (15%) out of total 13 patients found positive for blood culture, the organism which was found in the intraoperative fluid was subsequently found in the blood culture. This shows that it is unlikely that the migration of the intraoperative organism is the cause of subsequent bloodstream infection in these patients.
The patients were followed up during the entire duration of their stay in the hospital and the final outcome of the patient was noted. The death rate reported in this study was similar to that of some other studies.26,27 Two important factors needs to be considered when taking this mortality rate into consideration. One factor is that 97% of the patients included in this study needed at least a day of care in the level 3 setting of the hospital and the second factor is the kind of patients the hospital serves. The hospital in which the study was conducted is an apex tertiary care hospital catering mainly to the needs of referred cases from the surrounding areas.
The number of patients with shock at the time of admission was evaluated and shock was found to be present in only 22% of patients admitted in study. The mean duration of stay of 16.5 ± 12.8 days demonstrates that patients require at least 2–3 weeks of hospital care. The long period of stay predisposes the patient vulnerable to acquiring a hospital-based nosocomial infection. 28 This makes it all the more important in judiciously administering antibiotics in the preoperative and postoperative period of stay. It is important that the empiric regimen to be administered for perforation peritonitis is based upon local evidence rather than blindly following international guidelines. The microbial patterns found, and therefore the resistance to antibiotics, vary between different geographical regions. The study conducted as a part of the antibiotic stewardship program serves the much needed purpose of generating evidence for critical decision-making in such cases.
The sample size could be a limiting factor in the study; however, it was conducted over 6 months. Both referred and directly admitted (without reference) patients were included in the study.
Conclusion
We would suggest use of piperacillin-tazobactam or imipenem in patients presenting with complicated intra-abdominal infections secondary to perforated viscus, especially if they have sepsis, and imipenem if the patient is in septic shock. It is important that in future, local data are considered for making antibiotic policies for a particular setting and these must be updated regularly. Antimicrobial stewardship programs can have such discrete research undertaken to generate evidence-based policies in their respective healthcare settings.
Footnotes
Acknowledgements
Kumar-MP collected the data, did statistical analysis and wrote the manuscript. NS conceptualized the idea, oversaw the research and wrote the manuscript. PK and AG collected the samples and edited the manuscript. SM suggested changes to the study plan and edited the manuscript. VG and PR analysed and interpreted the microbiological samples and were involved in editing the manuscript. NM drafted the manuscript and compiled the results. All other authors (RG, VG, TDK, GRV, RS, GS) were surgeons who treated the patients, gave inputs to the study design, assisted in carrying out the study and edited the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.