
Abstract
Advancements in medicine have led to a considerable increase in the proportion of patients living with severe chronic diseases, malignancies, and HIV infections. Most of these conditions are associated with acquired immune-deficient states and treatment-related immunosuppression. Although infections as a result of neutropenia have long been recognized and strategies for management were developed, non-neutropenic immunosuppression has been overlooked. Recently, community-acquired infections in patients with frequent, significant exposure to healthcare settings and procedures have been classified as ‘healthcare-associated infections’ since they are more similar to hospital-acquired infections. Most of the non-neutropenic immunosuppressed patients have frequent contact with the healthcare system due to their chronic and severe diseases. In this review, we focus on the healthcare-associated bloodstream infections in the most common non-neutropenic immunosuppressive states and provide an update of the recent evidence for the management of these infections.
The immune system can be damaged by various clinical conditions and medications. In adult patients, acquired immunosuppression occurs mostly due to end-stage liver and renal diseases, diabetes mellitus, solid and hematologic malignancies, acquired immune deficiency syndrome (AIDS), organ and tissue transplantation, immunosuppressive medications including corticosteroids, and also due to aging. The significance of neutropenia as a cause of immunosuppression has been recognized for many decades, but it is only the tip of the iceberg. Non-neutropenic immunosuppressive states are increasing globally due to the aging of populations and increases in the prevalence of chronic diseases. Although there are several guidelines providing recommendations for the management of various infections among neutropenic patients, there are no recommendations for the immunosuppressed patients without neutropenia. Most of these patients have frequent contact with healthcare settings and therefore fit into the definition of healthcare-associated infections, even the episode is community-onset. 1 In this article, we use the term healthcare-associated bloodstream infections (HCA-BSIs) to define community-onset bacteremia in patients with recent and/or frequent exposure to the healthcare setting and procedures.1,2 We specifically focus on HCA-BSIs in the most common non-neutropenic immunosuppressive states and provide an update of the recent evidence for the management of these infections.
Elderly patients
People living beyond 65 years are an increasing portion of the world’s population. Infection risk and related mortality are higher in the elderly due to diminished cognitive and physiologic functions and age-related changes in immunity, that is, immunosenescence.
Immunosenescence mostly affects adaptive immune system, presenting with major defects in cell-mediated immunity and significant impairment of humoral immune response.3–5 The innate immune response is preserved to a great extent, even in the extreme old age.3,4 Thymic involution due to aging leads to loss of T cells, both CD4 and CD8, and reduced proliferative capacity of naïve T cells. 6 Diminished CD40 and CD28 ligand co-stimulatory molecules and diminished interleukin-2 (IL-2) synthesis cause further limitation in T-cell proliferation after exposure to antigens.4,6 In addition to defects in cellular immunity, B cell and plasma cell populations also decrease gradually. In contrast, immunoglobulin levels progressively increase with increasing the age, generating low-affinity, polyspecific, and T-cell independent antibodies with autoantibody reactivity. 7 As a result, loss of rapid and appropriate humoral response to new microbial antigens occurs although amnestic response to previously recognized antigens is mostly intact.5,7 The cumulative effect of these defects in the adaptive immune system is the impaired ability to rapidly and effectively respond to new pathogens leading to increased susceptibility to systemic infections due to both extracellular and intracellular pathogens. As average life expectancy increases in most parts of the world, infections will pose a significant clinical problem among this age group.
Previous studies have shown that community-onset BSI rates among the elderly are steadily increasing.8,9 This increase has been mostly attributed to older populations living longer with chronic diseases such as cancer, end-stage renal diseases (ESRDs), and more frequent use of medical devices. The risk of hospitalization due to septicemia increases linearly with the increasing age; a large community-based study from the United States estimated that the risk of hospitalization due to septicemia was four times higher among those aged >85 years compared to those aged 65–74 years. 8 In the geriatric population, it is difficult to differentiate HCA from community-acquired infections even if the infections are clearly ‘community-onset’. Along with the nursing home exposure, elderly have frequent contact with the healthcare system due to recurrent hospitalizations, chronic wound management, infusion center visits or hemodialysis, which all put them at greater risk for HCA-BSIs which frequently occur with antimicrobial-resistant organisms. 10 A recently published study, large study which included 830 hospital-acquired BSIs, showed that majority were central line associated and caused by Gram-positive bacteria: 23% were due to methicillin-resistant Staphylococcus aureus (MRSA), followed by methicillin-susceptible S. aureus (MSSA; 10.6%), Enterococci (6.1%), and coagulase-negative Staphylococci. 11 A more recent study which differentiated between community-acquired HCA and hospital-acquired BSIs confirmed that most commonly isolated organisms were still S. aureus in both hospital-acquired (24%) and HCA-BSIs (25%) and half of the isolates were methicillin-resistant, in contrast to Escherischia coli (37%) in community-acquired BSIs. 10 In the same study, only 20% of BSIs were primary and secondary cases most commonly originated from gastrointestinal tract and urinary tract infections (UTIs), with the exception of hospital-acquired cases, of which 41% were central catheter–related BSIs (CRBSI). 10 Mortality rates were 15% for hospital-acquired BSIs and 14% for HCA-BSIs.
Nursing home and long-term care facility residents are a distinct subgroup of the geriatric population who are most frail and debilitated. Infections arising in nursing homes are defined as HCA, and epidemiology of BSIs in the nursing home residents has been well described. 12 The incidence was about 0.3/1000 resident days and most common source for BSIs was UTIs (45–56%), followed by respiratory tract infections (7–14%) and skin and soft tissue infections (4–14%). Frequently isolated bacteria among nursing home residents were E. coli, Providentia spp., and Proteus spp. which were also the main causes of UTIs in this population.12,13 Pop-Vicas et al. 14 reported that multidrug-resistant (MDR) E. coli, Klebsiella, and Proteus spp. in elderly bacteremic patients were associated with nursing home residency and estimated a 16-fold increase from 1999 to 2005. Mortality rates were higher than the non-resident geriatric population, but seemed to be decreasing over the last 20 years, and 35% mortality was reported in 1982 in contrast to 23% in 2005.10,12
One of the main problems contributing to high mortality of BSIs among elderly is the lack of signs and symptoms classically associated with bacteremia, such as fever, hypothermia, or leukocytosis. These patients have the highest likelihood for afebrile bacteremia and more commonly present with organ failure, mental confusion, respiratory distress, and septic shock. 15 Several studies have shown that early and appropriate antimicrobial treatment decreases mortality in BSIs in the geriatric population. A recent comparison of older population (age > 65 years) with younger population has shown that the impact of inappropriate treatment was higher among the elderly; risk of mortality was approximately four times higher in the elderly patient who received inappropriate antibiotics for BSIs. 15 Choice of the antibiotics should be based on individual patient risk factors, most importantly, community-acquired versus HCA-BSIs, being a nursing home or long-term care facility resident, and possible source of bacteremia. Pop-Vicas et al. reported an increase of MDR Gram-negative bacteria among the elderly from 1% to 16% between the years 1999 and 2007 and proposed that the long-term care facility residents could be the main reservoir of MDR Gram-negative bacteria in the hospitals. 14 Crane et al., 10 based on their own data, recommend consideration of S. aureus coverage including MRSA in the initial empirical treatment of HCA-BSIs. However, both of these authors base their recommendations on data from the United States, where community-associated MRSA (CA-MRSA) has emerged as a main cause of skin and soft tissue infections and long-term care facilities are associated with large medical centers. Therefore, we suggest that local data on the epidemiology of BSIs in the geriatric population should closely be followed. Since studies showed that long-term care facilities can be the epicenters for development of MDR bacteria, guidelines for infection control practices and antimicrobial stewardship have been developed,16,17 and these have utmost importance to protect the elderly and also the population at large.
Non-neutropenic cancer patients
Cancer patients are a heterogeneous population with different malignancies; various defects in their immune system are due to both the underlying disease and chemotherapy. Nevertheless, there has been a striking increase in the BSIs with resistant bacteria in this whole population during the last decade.18,19 Chemotherapy in patients with solid tumors leads to neutropenia less frequently, and episodes are of shorter duration with the use of colony-stimulating factors and newer treatment modalities. Yet, patients with solid tumors are still predisposed to infections due to obstructive phenomenon, damage to anatomic barriers like skin and mucosal membranes, invasive procedures, radiotherapy, use of catheters or other devices, and previous antibiotic therapy. 20 Patients with hematologic malignancies are prone to BSIs even in the non-neutropenic state because of immunosuppression due to the disease itself, myeloablative therapy, recurrent and long-duration hospitalizations, and central venous catheter (CVC) use. Due to their frequent contact with the healthcare system, most of the community-onset bacteremias in cancer patients can be defined as HCA-BSIs. 21
It has been shown that BSIs in non-neutropenic cancer patients are mostly secondary and either spread from a primary infected focus (58%) or CVC related (22%).21,22 Most non-neutropenic patients with HCA-BSIs have advanced tumors and concomitant chronic diseases and they are older in comparison to the neutropenic patients with HCA-BSIs. 22 Mortality is also higher among non-neutropenic patients diagnosed with BSIs, 36% versus 26%, respectively; this difference is most likely to be due to older age, higher burden of malignancy, and comorbidities. 22 The prompt approach to febrile neutropenia with broad-spectrum antibiotics which has been the rule for many years may be another factor for the difference in mortality outcomes. Other studies have also shown similarly high mortality rates, changing between 20% and 40%, partly depending on the causal pathogen.20,23,24 Use of catheters in cancer patients has emerged to be the major source of HCA-BSIs; Raad et al. 25 have shown that CVCs were the cause for 69% of Gram-positive and 60% of Gram-negative BSIs in cancer patients.
In recent years, significant changes have occurred in the spectrum of organisms causing HCA-BSIs in cancer patients. The dominance of Gram-positive organisms has subsided over the last two decades, and Gram-negative bacilli have become the leading pathogens isolated from blood cultures in cancer patients, including non-fermentative Gram-negative bacilli in patients with long-term catheters.18,22 Several factors have been hypothesized to be the reason for this epidemiological change; such as decreasing use of quinolone prophylaxis or the use of less cytotoxic agents leading to less severe mucositis, whereas mucositis is related to bacteremia due to viridans Streptococci, Enterococci, as well as Gram negatives. 18 Another concerning trend in this population is the emergence of resistance, reported in both Gram-positive and Gram-negative isolates from BSIs.18,19,26
Being vigilant of BSIs in all cancer patients at the time periods when they are not neutropenic and assessment of specific risk factors are the first steps in the management of BSIs. Evaluation of CVC insertion site and searching for a primary site of infection are essential for source control in cancer patients with BSIs. Surveillance of pathogens causing BSIs stratified by hospital acquired versus HCA, underlying disease, presence of CVC and nature of chemotherapy is very helpful for building treatment decisions according to the local data. Prompt administration of antibiotics based on local resistance patterns and individual risk factors is crucial, as well as identifying modifiable risk factors, such as the removal of CVC. Several studies have shown that the CVCs should be removed in patients with CRBSI caused by S. aureus, Gram-negative bacilli, and Candida spp. 25
For the prevention of HCA-BSIs in cancer patient, risk factors need to be recognized and reduced or eliminated as much as possible, and routine prophylaxis is not recommended due to emergence of resistance. Patients and their families should be informed and educated on measures such as the care of CVCs outside of the hospital and important aspects of personal and environmental hygiene.
HIV/AIDS
The introduction of highly active antiretroviral therapy (ART) has dramatically improved the outcome of opportunistic infections in human immunodeficiency virus (HIV)-infected patients. Although not considered as opportunistic infections, studies conducted after the beginning of ART utilization showed a significant downward trend in the incidence of BSIs.27,28 But, even in the current ART era, the rates of BSIs in HIV patients remain significantly higher than that of the general population and are associated with increased morbidity and mortality.29–31 In the literature, data on the HCA-BSIs are very limited among HIV patients, and there seems to be a confusion of HCA infections with nosocomial infections. 32 Therefore, in this section, we considered severe community-onset BSIs in advanced patients in addition to clearly defined HCA-BSIs.
HIV infection leads to extensive changes in the immune system but abnormalities in cell-mediated immunity primarily, such as the progressive decrease in CD4+ T-cell counts and phagocytic cell dysfunction, increase the risk for bacterial infections. Elevated IL-10 levels with defective innate immune response have been shown to predispose HIV/AIDS patients to severe sepsis.33,34 Advanced HIV disease may lead to bacteremia due to failure of gut immunity in controlling bacterial translocation. 35
Major risk factors for HCA-BSIs were shown to be low CD4 counts, injection drug use (IDU), and the presence of CVCs.35,36 Common primary foci of BSIs were CVCs, pneumonia, and urinary tract and skin infections. 37 Due to frequent exposure to the healthcare system, most bacterial infections including BSIs are caused by resistant bacteria in HIV patients.36,38 This is also promoted by antibiotic usage related to intercurrent infections, as well as the selective pressure of chronic antibiotic use, such as co-trimoxazole prophylaxis. The study which described sepsis and septic shock in HIV patients has shown that 38% have primary BSIs caused by Gram-negative bacteria which are mostly acquired in the hospital. 39
The epidemiology of BSIs among HIV patients varies with the geographical region. Worldwide most common causes of community-onset BSIs are non-typhoidal Salmonella (NTS), Streptococcus pneumoniae, E. coli, and S. aureus, and there is a general increase in the resistant strains. Distribution of bacteria and resistance patterns depends on the region; Salmonella spp. are most frequently isolated in Africa or Southeast Asia, whereas coagulase-negative Staphylococci, S. aureus, Enterococcus spp., and E. coli are more commonly reported from developed countries.40–42 Injection drug users are at very high risk of repeated BSIs due to S. aureus including methicillin-resistant strains.43–45 Recently, countries with high IDU reported increases in BSI rates.29,31 HIV patients represent a particularly high risk group for invasive disease with S. pneumoniae, both in developing and developed countries except for Southeast Asia where 47% BSIs are caused by NTS.31,46 Although the incidence of invasive pneumococcal disease (IPD) has decreased significantly after widespread use of ART, the risk of IPD in HIV-infected patients remains up to 60-fold higher than that of the age-matched general population.47,48 For clearly defined hospital-acquired BSI cases, etiological agents were predominantly Gram-positive: S. aureus, coagulase-negative Staphylococci, and Enterococci.32,37,38 Gram-negatives, mainly Pseudomonas aeruginosa and Enterobacter spp., were less frequently isolated compared to Gram-positives.37,38
For an HIV patient presenting with fever, it should be kept in mind that BSIs either primary or secondary are still one of the most frequent infections, especially in advanced HIV infections. Therefore, clinicians should have a low threshold for initiating parenteral antibiotics in HIV patients with fever. 49 Due to geographically varying distribution of bacteria and resistance patterns, empirical treatment should follow local data and guidelines. There are additional factors that should also be considered for the empirical treatment. Most importantly, patient’s history or a previous record of IDU must lead to consideration of S. aureus BSI, promptly. These patients are also at considerably higher risk for the development of endocarditis and early detection is crucial to improve treatment outcomes. 45 Recent evidence suggests that MRSA and CA-MRSA are becoming an emerging epidemic among HIV patients in some developed countries.43,45 Therefore, depending on the local epidemiology, empirical use of glycopeptides or daptomycin can be considered in those settings. 49 In Africa and Southeast Asia, NTS show high prevalence of multidrug resistance, particularly to antibiotics regarded as first line in low resource settings, that is, ampicillin, chloramphenicol, and co-trimoxazole. 42 Therefore, ceftriaxone and ciprofloxacin are recommended for the initial treatment in Africa. 49
Finally, Advisory Committee on Immunization Practices (ACIP) and British HIV Association recommend pneumococcal vaccination to all HIV-infected adults in order to prevent IPD.50,51
End-stage liver disease
With the development of effective vaccines and new antiviral therapies, there are less end-stage liver disease (ESLD) caused by chronic viral hepatitis; currently, steatohepatitis and alcoholic liver disease are the leading causes in developed countries.52,53 Independent of the cause, ESLD is an immunosuppressive state, and these patients are at significantly high risk of developing severe infections, and all-cause mortality rates remain high for 1 year even after successful treatment. 53 Furthermore, bacterial infections are the most important precipitating factor of acute decompensation in this group of patients. Rapid progression of bacterial infections to multiorgan failure and septic shock can increase short-term mortality rates up to 75%.54,55 Cirrhotic patients with HCA-BSIs have 30% mortality rates within 30 days.56,57
Several factors lead to an immunosuppressive state among ESLD patients which is called cirrhosis-associated immune dysfunction syndrome (CAIDS). In CAIDS, both humoral and cell-mediated immune systems are adversely affected. Monocyte chemotaxis and macrophage Fcɣ-receptor–mediated clearance of bacteria and bacterial killing are reduced; downregulation of Human Leukocyte Antigen–antigen D Related (HLA-DR) on antigen-presenting monocytes, decreased neutrophil mobilization, and phagocytosis occur.54,58–61 In addition, increased intestinal mucosal permeability, delayed intestinal transit time, and bacterial overgrowth facilitate bacterial translocation from gastrointestinal lumen to lymph nodes, to ascitic fluid, and to systemic circulation. Even though bacterial translocation can be controlled by a functional immune system among healthy individuals, CAIDS and porto-systemic shunting will lead to frequent BSIs among ESLD patients.54,58 A dysregulation of the immune system also occurs due to increased levels of nitric oxide, pro-inflammatory cytokines like tumor necrosis factor-alpha (TNF-α) and IL-6, and defective production of anti-inflammatory cytokine IL-10, resulting in excessive inflammation and ‘cytokine storm’.58,62,63
Progression of bacterial infections can be rapid and highly mortal; therefore, clinical vigilance and early diagnosis are important. Spontaneous bacterial peritonitis (SBP) is the most prevalent bacterial infection in this patient group, and bacteremia accompanies nearly half of SBP. 64 The prevalence of SBP has been reported in up to 30% of hospitalizations; half of these being present at admission and other half develops during hospitalization.58,65 Majority of these infections are caused by E. coli, Klebsiella spp., other Enterobacteriaceae, P. aeruginosa, Enterococci, and Streptococci; BSIs secondary to SBP occur with these same agents.58,63,66 In a recent, retrospective cohort study, the incidence of BSIs was 11.7/10,000 patient-days; 67% of these were HCA-BSIs and majority (72%) were primary without any other site of infection. 56 Same study also showed that Gram-negative bacilli constitute more than two-thirds of all isolated pathogens from blood; of these, 47% were Enterobacteriaceae and 15% were non-fermenters. Prevalence of MDR and extensively drug-resistant pathogens, among Gram-negative bacilli, was 25% and 21%, respectively. 56 Studies showed that MDR pathogens among ESLD patients were associated with long-term norfloxacin prophylaxis, use of beta-lactam antibiotics, and infections with MDR bacteria in the previous 6 months. Use of invasive procedures and central catheters in intensive care was associated with infections due to Gram-positive cocci, most frequently S. aureus and Enterococcus spp.56,64
During management of ESLD cases, it should be noted that most cases of SBP do not have typical symptoms; therefore, a diagnostic paracentesis in all patients with ascites, at the time of hospitalization and in those with systemic signs of infections, hepatic encephalopathy, gastrointestinal bleeding, shock, and progressive renal impairment are indicated.58,65 In patients with suspected BSIs, prompt empirical treatment with antibiotics is necessary without waiting for the culture results. Sources of secondary bacteremia among ESLD patients, other than SBP, are urinary tract, respiratory, biliary tree, and soft tissue infections.56,57,67 Most community-onset infections should be treated as ‘healthcare associated’ in these patients, due to their frequent exposure to the healthcare environment.
For the appropriate empirical treatment of HCA-BSIs, the presence of a local infection or central catheter, long-term prophylaxis with quinolones, as well as the local epidemiology must be taken into consideration. Hospital acquisition, MDR bacteria, the presence of hepatorenal syndrome, sepsis, high Child–Pugh score, and high Model For End-stage Liver Disease (MELD) score increased the risk of mortality in patients with BSIs.15,56,68
Due to high mortality risk and predominance of highly resistant Gram-negative pathogens, empirical treatment of HCA-BSIs requires starting with wide-spectrum antibiotics and later tailoring the treatment according to culture results. Depending on the local epidemiology, anti-pseudomonal beta-lactam/beta-lactamase inhibitors or carbapenems would be the first-line empirical choice in many centers. 57 There are insufficient data to guide the decision whether to include agents covering Enterococci or methicillin-resistant Staphylococcus spp. in the initial empirical therapy. However, based on the most recent epidemiological data, approximately 40% of cultured bacteria from BSIs episodes are Gram-positive agents, and empirical coverage might be considered in patients with sepsis or septic shock.15,56 Suggestions for antibiotic dose adjustment in ESLD were given in Table 1.
Antibiotic administration recommendations in patients with end-stage liver disease.
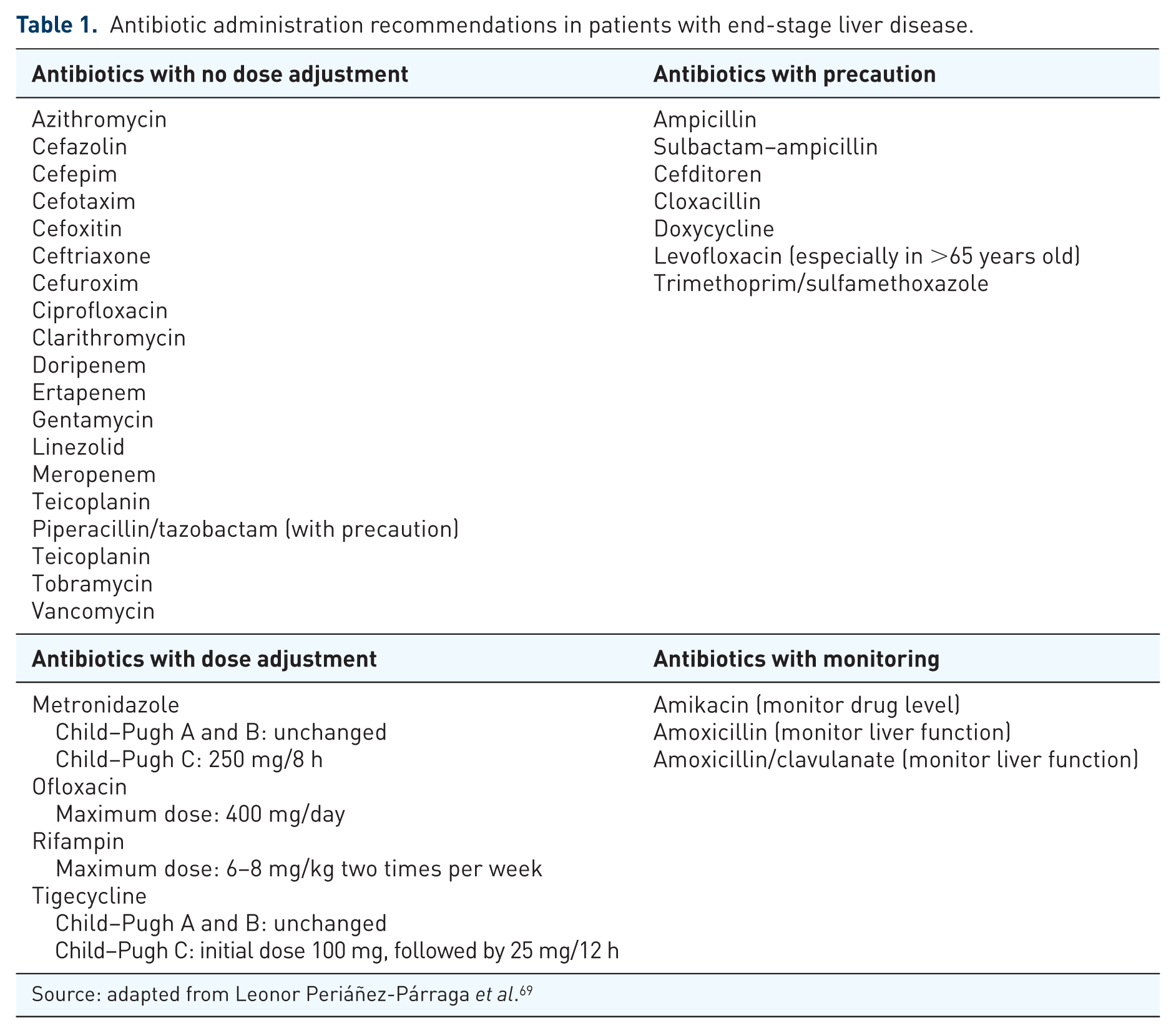
Source: adapted from Leonor Periáñez-Párraga et al. 69
Long-term primary or secondary prophylaxis to prevent BSIs is not recommended. However, variceal bleeding which complicates up to 30% of patients with cirrhosis has been shown to be associated with bacteremia; therefore, guidelines for treatment of patients suffering variceal gastrointestinal bleeding also include short-term antibiotic prophylaxis. 70 A Cochrane meta-analysis has shown statistically significant 75% reduction in BSIs [risk ratio (RR): 0.25, 95% confidence interval (CI): 0.15–0.40] and 21% reduction in mortality (RR: 0.79, 95% CI: 0.79–0.98), with the use of short-term antibacterial prophylaxis in patients with variceal bleeding. 70 No significant difference was shown between the types of antibiotics; both quinolones and cephalosporins were equally effective. As the recurrence of SBP is as high as 70%, secondary prophylaxis with norfloxacin 400 mg/day, orally, is recommended. 71
Chronic kidney disease and ESRD
In this section, chronic kidney disease (CKD) refers to patients who has estimated glomerular filtration rate <60 ml/min/1.73 m2 but not receiving dialysis, and ESRD refers to patients who have stage-5 CKD and are receiving maintenance dialysis.
Large cohort studies have shown that patients with CKD are at increased risk of morbidity and mortality from infections, and this risk increases as renal function deteriorates.72,73 A recent systematic review has shown that CKD increases the risk of BSIs, UTIs, and pneumonia, yet BSIs are associated with the highest rates of hospitalization and mortality.73,74
It is well known that loss of renal function is strongly associated with immune dysfunction; both the innate and adaptive cellular immune systems are adversely affected and CKD patients are susceptible to infections and respond poorly to vaccination. 75 Other multiple risk factors also predispose patients with CKD to infections such as hypoalbuminemia, immunosuppressive therapy, nephrotic syndrome, uremia, anemia, and malnutrition. 76 After initiation of dialysis, vascular or peritoneal access, repetitive break of skin integrity, S. aureus nasal carriage, and iron overload become additional strong risks factors for infections.76,77
In ESRD patients, major cause of BSIs is hemodialysis vascular access; 90% of all hemodialysis-related BSIs occur in patients dialyzed through CVCs. 78 The risk is highest if the patient is receiving hemodialysis using a non-tunneled CVC and decreases in the order of tunneled CVC, arteriovenous grafts, and arteriovenous fistula. 79 During the use of CVCs, organisms enter into the bloodstream either through intraluminal or extraluminal pathways and both involve formation of biofilm, triggered by the adherence of the organism to the catheter surface.80,81 Bacteria are enclosed in the biofilm which is a matrix produced by bacterial products and host constituents adherent to the catheter surface. Susceptibility of bacteria within the biofilms to antimicrobials is decreased up to 100–1000 fold.80,81 Most common microorganism implicated in CRBSIs is S. aureus followed by coagulase-negative Staphylococci and Enterococci. Gram-negative organisms, mostly E. coli, have also been isolated in a small group of patients.41,81–83 In a recent, population-based study, the risk of S. aureus BSI was found to be 65-fold higher among ESRD patients compared with population controls. 82 Overall mortality rate, for S. aureus BSIs, is above 20% and has not shown a major decline in recent years. 84 Furthermore, S. aureus BSIs are associated with severe complications such as endocarditis, osteomyelitis, and pneumonia due to septic emboli. The proportion of MRSA among S. aureus infections has been reported in broadly varying proportions from 1% to 62%, depending on the country and location.81–83,85 The proportion of vancomycin-resistant species among the Enterococcal BSIs has also increased in recent years; ESRD patients are at risk of acquiring vancomycin-resistant Enterococci (VRE) due to their frequent hospitalizations and exposure to vancomycin.41,86,87 It has been shown that VRE infections can cause outbreaks in hemodialysis centers due to poor infection control practices and associated with complications similar to those for S. aureus, such as endocarditis and metastatic infections. 80
The proportion of patients receiving hemodialysis with a CVC has increased dramatically in recent years, which has created a large cohort of patients with a very high risk of BSIs.79,81 The burden of CRBSIs is enormous in the hemodialysis population; as a result of growing awareness of this problem, many countries have initiated surveillance systems and programs to decrease the CRBSI rates.80,88 Surveillance definitions for BSIs which arise from a CVC are different from clinical definitions such as the most commonly used Infectious Diseases Society of America (IDSA) definitions. 89 When attempting to diagnose whether a CVC is the source of a BSI and for making treatment decisions, the use of clinical definitions (which are more specific compared to the surveillance definitions) is more appropriate. 89 IDSA definitions of CRBSI require specialized testing, such as the blood and CVC cultures and determining either time to positivity or quantitative colony counts. 89 However, it is common that a peripheral blood sample cannot be obtained in hemodialysis patients due to exhaustion of peripheral veins; in these cases, positive culture results obtained from blood line of dialysis catheters should guide the treatment if no other source of infection is found. 89 It has been shown that prior to a BSI, CVCs are colonized both endoluminally and extraluminally; however, studies on surveillance cultures had conflicting results; therefore, routine surveillance cultures of CVCs are not recommended. 88
The first step in the management of HCA-BSIs, in this group of patients, is being alert to the significantly increased risk of BSIs and quick progress to sepsis. As shown by a recent study, CKD patients may lack typical symptoms and those patients who did not have fever at the initial presentation experienced delays in receiving adequate treatment. 90 These patients were more likely to die due to the associated sepsis. This is a finding emphasizing the initiation of most appropriate empirical therapy, as soon as possible, in CKD patients. Broad coverage for both Gram-positive and Gram-negative organisms while culture results pending is recommended.78,81,89 Due to the high incidence of MRSA infections in ESRD patients and associated high mortality, empirical coverage should include MRSA, particularly in critically ill patients and in healthcare settings with high incidence of MRSA.80,81,89 Vancomycin is the most frequently used glycopeptide antibiotic for this purpose, but in institutions where there is a prevalence of MRSA isolates with vancomycin minimal inhibitory concentration (MIC) > 2 µm/ml, alternative antibiotics, such as daptomycin, should be considered.81,89 In patients who were started glycopeptides empirically, if the culture results yield MSSA, glycopeptide antibiotic should be changed to an antistaphylococcal beta-lactam, such as cefazolin or nafcillin. This approach has been shown by several studies to be more effective and improve survival.84,89 If possible, antibiotics should be selected based on suitable pharmacokinetics in ESRD patients, so that the administration intervals can be synchronized with dialysis sessions. Main examples for this kind of administration are vancomycin and cefazolin. Due to the recent high-flux dialysis membranes, suggested vancomycin dose in dialysis patients have been updated; 20 mg/kg (or 1 g) loading dose followed by 500 mg supplementation after each dialysis session leads to the recommended trough levels between 15 and 20 µg/ml. 80 Since half-life of cefazolin increases in renal failure, it can also be administered as three times per week, parenterally, after dialysis sessions. 84 Use of linezolid, aminoglycosides, clindamycin, co-trimoxazole, and rifampicin are not recommended in CRBSIs caused by MRSA. 80 In hemodialysis centers where methicillin resistance among staphylococci is rare, antistaphylococcal beta-lactams may be chosen for empirical therapy. All patients diagnosed with S. aureus BSIs should thoroughly be investigated for endocarditis and metastatic complications.
For empirical Gram-negative coverage, fourth-generation cephalosporins, carbapenems or β-lactam/β-lactamase combinations, with or without an aminoglycoside, can all be used, depending on the local susceptibility data and whether the patient is in critical condition. 89 For example, Ceftazidime has the pharmacokinetic advantage which allows dosing after each dialysis session; and ceftriaxone does not need renal dose adjustment and used once daily. 89 In severely ill patients with sepsis or patients known to be colonized, empirical coverage for MDR Gram-negative bacteria can be considered based on local susceptibility data. After isolation of causative agent, if possible, de-escalation of antibiotic treatment by narrowing the coverage should be performed. 89
Using only intravenous antibiotics among hemodialysis-associated CRBSIs is not sufficient due to the high relapse rates. Centers for Disease Control and Prevention (CDC) guidelines recommend prompt catheter removal if the causative agent is S. aureus, Pseudomonas spp., or Candida spp. in critically ill patients and in patients with persistent bacteremia or who has metastatic infections. 89 In these patients, a short-term temporary catheter inserted from another anatomical site should be used for dialysis until negative blood cultures are obtained, that is, only when another long-term dialysis catheter insertion can be inserted.78,89 For infections caused by coagulase-negative Staphylococci and Gram-negative bacteria other than Pseudomonas spp., catheter salvage or change over a guidewire can be attempted in patients with good response to antimicrobial treatment within 2–3 days. In these cases, antibiotic lock is also recommended as an adjunctive therapy. 89 For antibiotic lock treatment, a suitable antibiotic is combined with heparin and instilled into each lumen of the CVC at the end of dialysis sessions for 10–14 days. 89
Duration of treatment for CRBSIs in ESRD patients depends on the microorganism; most recent IDSA guidelines recommend 3 weeks of treatment for uncomplicated S. aureus CRBSI and 7–14 days for Enterococcus spp. and Gram-negatives. If the patient has persistent bacteremia or metastatic infections such as endocarditis, the recommended duration of treatment is 4–6 weeks. 89
Avoiding the use of CVCs for long-term hemodialysis, access will significantly reduce the excessively high burden of HCA-BSIs among ESRD patients. Since arteriovenous fistulas (AVFs) have the lowest rates of infections, as well as other complications, programs such as the ‘Fistula First Breakthrough Initiative’ have been instigated to promote the use of AVF and lower their rates for the use of CVCs for dialysis. 91 It has been shown that using recommended catheter insertion and maintenance guidelines significantly lowers the CRBSI rates. 92 Strict adherence to hand hygiene and wearing clean or sterile gloves before any contact with the CVC hub is necessary. Guidelines recommend the use of maximal aseptic techniques and barrier precautions using cap, mask, sterile gown, sterile gloves, and a sterile full-body drape during the insertion of CVCs.80,93 The preferred topical antiseptic is >0.5% chlorhexidine preparation with alcohol for skin antisepsis during insertion and exit-site care. 93 CDC guidelines also recommend the use of povidone iodine antiseptic ointment or bacitracin/gramicidin/polymyxin B ointment at the hemodialysis catheter exit site after catheter insertion and at the end of each dialysis session, as well as the use of sterile gauze or sterile transparent, semipermeable dressing to cover the catheter site.78,93 Randomized trials investigating the efficacy of antibiotic lock solutions for prevention of CRBSIs have failed to show efficacy, and since this kind of long-term use can promote antibiotic resistance, routine use of lock solutions for prevention is not recommended. 93 Although lower than CVCs, patients who have AVFs or Arteriovenous graft (AVG) are also at risk of HCA-BSIs, and effective skin antisepsis should be performed prior to cannulation for hemodialysis session. Education of both patients and healthcare personnel on catheter care is an essential part of CRBSI prevention.
Connective tissue diseases
In addition to the immune suppressive agents used for treatment, connective tissue diseases have well-documented immune function abnormalities. However, data on the BSIs among these patients are very limited and exist only for patients with systemic lupus erythematosus (SLE) and dermatomyositis (DM)/polymyositis (PM).
There is a long list of both humoral and cellular immune system abnormalities in SLE patients some of which include the decreased phagocytic action of monocytes, defective phagocytic and chemotaxic activity of neutrophils, CD4+ T-cell depletion, defects in CD8+ T-cell cytolytic activity, decreased number and activity of natural killer (NK) cells, and polyclonal B cell activation with hyperglobulinemia and defective cytokine production. 94 Frequently used treatments to control the disease activity, such as systemic corticosteroids, methotrexate, cyclosporine, and cyclophosphamide, also cause immunosuppression and predisposition to bacterial infections. SLE patients with advanced disease have frequent contact with the healthcare system; almost 50% of BSIs were hospital acquired in a 6-year follow-up study. 95
Cohort studies have shown that bacterial infections are the primary cause of mortality among SLE patients.96–98 Bacteremias are frequently seen, reported in 16–47% of patients, and they have the highest mortality rates among all the infections, reported to occur between 10% and 15% of all BSIs.95,99 Almost a quarter of patients with primary BSIs have recurrent bacteremias, mostly occurring with the same microorganism. 95 In the largest study from a tertiary-care center in China, most frequent causes of BSIs were S. aureus, non-typhoidal Salmonella, E. coli, Klebsiella spp., and Pseudomonas spp. 95 Secondary BSIs in SLE patients most frequently occurred due to spread from vascular catheters and genitourinary tract infections. 99 Low C3 levels, recent hospitalization, and prednisone dose at the time of infection are factors increasing the risk of BSIs with drug-resistant bacteria, including MRSA, P. aeruginosa, and extended-spectrum beta-lactamase (ESBL)-positive E. coli.99,100
PM and DM are idiopathic inflammatory myopathies also affecting internal organs. Given the rarity of disease, there are a few small case series evaluating the rates and types of infections among DM/PM patients; data about HCA-BSIs are very limited. There are reports showing that bacterial infections complicate the course of disease in 30% of PM/DM patients.101–103 Moreover, in a recent study, approximately 56% of the bacterial infections were BSIs significantly increasing the risk of mortality in hospitalized DM/PM patients. 104 In small series regarding the infections in PM/DM, etiologic pathogens were S. aureus, Klebsiella spp., Salmonella spp., E. coli, and S. pneumonia in both BSIs.101,103
We recommend that in SLE and DM/PM patients, clinicians have a low threshold for initiating antimicrobial treatment when BSIs are suspected, keeping in mind that these patients, especially with advanced disease, have frequent contact with healthcare institutions and dialysis centers. Furthermore, we believe that analytical studies assessing the risk and its magnitude for community-acquired BSIs and HCA-BSIs in patients with autoimmune diseases and biological agent recipients are urgently needed.
Solid organ transplantation
Solid organ transplantation (SOT) is another severe non-neutropenic immunosuppressive state due to both end-organ failure and immunosuppressive drug use. In addition to the immunosuppressive state, surgical complications, prolonged hospitalization, existence of co-morbidities, and increased frequency of invasive interventions predispose SOT patients to infectious complications. As the number of SOT procedures grew steadily over the last decade, reports of increased frequency of BSIs among this group of patients also increased.105,106 BSIs are still a major cause of mortality after transplantations. Since SOT patients are a heterogeneous group, we will review the risk factors and etiological agents separately for different transplantation procedures.
Incidence of BSIs after
Infections with MDR bacteria are a growing problem in liver transplant recipients as well. BSIs with ESBL-producing Enterobacteriaceae and other Gram-negatives like Stenotrophomonas maltophilia, Pseudomonas spp., and A. baumanii have all been reported with increasing frequency.123,126 Recently, carbapenemase-producing K. pneumoniae has been reported in 8.4% of infections in which 18 of 20 infection were BSI with a very high mortality (45%). 127 Mortality of BSIs is high in liver transplant patients, some studies reporting up to 52% mortality especially with BSIs caused by MDR bacteria.107,128 Empirical treatment in these patients must be based on local antimicrobial surveillance data, previous antibiotic use especially the long-term prophylaxis frequently given to these patients at the pre-transplant period, and the presence of risk factors in particular intra-abdominal infections, presence of a central catheter, and presence of septic shock.
After
Management of BSIs in SOT recipients includes prevention, prompt accurate diagnosis, and early effective antibacterial treatment. It should be noted that SOT patients can also acquire bacteria through the donor, and these infections are difficult to diagnose, leading to delayed treatment and high mortality. 124 Adherence to the pre-transplant infection screening guidelines can provide reductions in early post-transplantation infections. 146 In addition, following infection control measures is extremely important to prevent BSIs in SOT patients who are vulnerable due to serious surgical procedures, underlying disease, and post-transplantation immunosuppressive treatment.93,147,148 In addition, perioperative antibacterial prophylaxis guidelines should be followed without leading to prolonged use, except in patients with pre-transplant infections such as CF patients or patients who received a graft from an infected donor. 135
Appropriate and early antibacterial treatment is crucial for the treatment of BSIs in SOT. Antibiotic choice should be based on the underlying transplantation type, immunosuppressive regimen and severity of immunosuppression of the individual patient, the presence of surgical complications, clinical severity of infection, and local antibiotic resistance patterns of pathogen microorganisms. If BSI is secondary to another infection, source control is essential. 149 Empirical treatment must be adjusted according to the culture results and must take into account the toxicity of the chosen antibiotics for the transplanted end-organ. Duration of antibacterial treatment differs from 7 to 10 days to 4 to 6 weeks according to the etiologic microorganisms, source of BSI, and end-organ involvement. 89 Another aspect of the treatment is the drug–drug interactions between antibiotics and immunosuppressive drugs. For MDR microorganisms, combination of different classes of antibiotics, continuous intravenous infusions, or higher doses of antibiotics can be used and synergy testing could point out the most useful combination choices. 150 In the case of MRSA, vancomycin-intermediate Staphylococcus aureus (VISA), or VRE treatment guidelines must be followed.151,152 Table 2 summarizes the common sources and pathogens of BSI in different SOT patients and empirical antibiotic choices.
Common sources of infection and bacteria for BSIs in SOT patients.

SOT: solid organ transplantation; BSI: bloodstream infection.
Conclusion
HCA-BSIs are important causes of morbidity and mortality in non-neutropenic immunosuppressive patients. Awareness of the increased risk in this group of patients, evaluation of risk factors, and prompt appropriate antimicrobial administration are essential. Further studies are urgently required for detailed epidemiologic data and for the management of HCA-BSI in this group of highly vulnerable patients.
Footnotes
Appendix 1
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.A. is a full-time employee of GSK since May 2016.