
Abstract
Objective:
Scalloping of visceral organs is described in pseudomyxoma peritonei, malignant ascites, among other conditions, but not tuberculosis.
Methods:
We report findings from a retrospective study of patients with abdominal tuberculosis who had visceral scalloping on abdominal computed tomography (CT). Diagnosis of abdominal tuberculosis was made on the basis of combination of clinical, biochemical, radiological and microbiological criteria. The clinical data, hematological and biochemical parameters, and findings of chest X-ray, CT, Mantoux test, and HIV serology were recorded.
Results:
Of 72 patients with abdominal tuberculosis whose CT scans were included, seven patients had visceral scalloping. The mean age of these patients was 32.14 ± 8.43 years and four were men. While six patients had scalloping of liver, one had splenic scalloping. The patients presented with abdominal pain (all), abdominal distension (five patients), loss of weight or appetite (all), and fever (four patients). Mantoux test was positive in five, while none had HIV infection. The diagnosis was based on fluid (ascitic or collections) evaluation in four patients, ileo-cecal biopsy in one patient, fine needle aspiration from omental thickening in one patient, and sputum positivity for acid fast bacilli (AFB) in one patient. On CT examination, four patients had ascites, five had collections, one had lymphadenopathy, four had peritoneal involvement, three had pleural effusion, and two had ileo-cecal thickening. All except one patient received standard ATT for 6 months or 9 months (one patient). Pigtail drainage for collections was needed for two patients.
Discussion:
This report is the first description of visceral scalloping of liver and spleen in patients with abdominal tuberculosis. Previously, this finding has been reported primarily with pseudomyxoma peritonei and peritoneal carcinomatosis.
Conclusion:
Visceral scalloping may not conclusively distinguish peritoneal tuberculosis from peritoneal carcinomatosis or pseudomyxoma peritonei.
Introduction
Peritoneal tuberculosis is the commonest form of abdominal tuberculosis. The diagnosis is suspected in setting of clinical features like abdominal pain and distension with radiological findings like presence of ascites, peritoneal thickening, thickening of lymph nodes (with central hypodensity), omental thickening, nodularity and so on. The diagnosis is based on presence of low serum ascites albumin gradient and elevated adenosine deaminase (ADA) levels (>32 U/L). Microbiological confirmation is unusual as acid fast bacilli (AFB) positivity, culture positivity, and polymerase chain reaction (PCR) positivity rates are low. 1 Important differential diagnosis of ascites includes chronic liver disease, malignant ascites, and pseudomyxoma peritonei. Scalloping of the visceral surfaces of intraperitoneal organs represents the indentations that usually are described to occur in patients with pseudomyxoma peritonei and are believed to occur as a consequence of pressure exerted on the surface of visceral organs by intraperitoneal collections or mucin deposits. 2 It is most commonly seen along the margins of the liver and spleen. The scalloping of the visceral surfaces of intraperitoneal organs is considered an important criterion to discriminate peritoneal carcinomatosis from other causes of ascites on computed tomography (CT). 3 The finding of the scalloping of liver and spleen margins, however, to best of our knowledge has not been described in tuberculosis. We retrospectively studied our collected database of CT of patients with abdominal tuberculosis and looked for presence of visceral scalloping.
Methods
Patients
This was a retrospective study of patients with abdominal tuberculosis who were noted to have visceral scalloping on abdominal CT. The study included only those patients who underwent abdominal CT for evaluation of their abdominal complaints and were eventually diagnosed to have abdominal tuberculosis. These patients were seen at a large tertiary care hospital in North India over a period of 18 months. The diagnosis of abdominal tuberculosis was made on basis of combination of clinical, biochemical, radiological and microbiological criteria. A confirmed case was diagnosed if a patient with clinical symptoms consistent with abdominal tuberculosis had confirmatory microbiological findings like positivity for AFB in tissue biopsies or ascitic fluid or culture positive or tuberculosis PCR (TB-PCR) positivity. However, in absence of microbiological evidence, a diagnosis of probable tuberculosis was made if tissue histopathology revealed caseous necrosis or epithelioid granulomas or if ascitic fluid ADA levels were >32 IU/l. Only those probable cases that showed resolution of clinical features (disappearance of ascites or healing of tubercular ulcers) were included for analysis.
The clinical data for patients who had visceral scalloping were recorded. These included presence of symptoms like abdominal pain, distension, fever, loss of weight, loss of appetite, peripheral lymphadenopathy, abdominal lump, and ascites. Occurrences of any comorbid diseases, including diabetes and HIV, were also recorded. Hematological and biochemical parameters and findings of chest X-ray, Mantoux test, and HIV serology were recorded. The findings of ascitic fluid analysis, endoscopic findings, histological findings, and microbiological evaluation were recorded. The CT findings were also recorded.
Imaging technique
All scans were acquired in the portal venous phase (60–65 s delay after the start of the contrast injection) from the domes of the diaphragm to the pubic symphysis on a multidetector scanner. Positive oral or a neutral oral contrast medium and intravenous non-ionic iodinated contrast medium had been administered in all of the patients.
Image analysis
All the scans were retrospectively reviewed by a gastrointestinal radiologist for the presence of lymphadenopathy, ascites, collections, solid organ involvement, scalloping of the visceral surfaces, peritoneal thickening and enhancement, bowel strictures, psoas abscess, and pleural effusion.
Results
Of the 72 patients diagnosed with abdominal tuberculosis who had abdominal CT done, seven patients were found to have visceral scalloping (Figures 1–4). Of these seven patients, four had a confirmed diagnosis of tuberculosis, while the rest had probable tuberculosis. The mean age of these patients was 32.14 ± 8.43 years. There were four men among these seven patients. Six patients had scalloping of liver (Figure 1, 3, 4), while one had scalloping of the spleen (Table 1; Figure 2). The patients presented with complaints of abdominal pain (all), distension (five patients), loss of weight or appetite (all), and fever (four patients). The Mantoux skin test was positive in five patients and one patient had previous history of tuberculosis. None of the patients had evidence of HIV infection. The diagnosis was based on evaluation of fluid in four patients, ileo-cecal biopsy in one patient, fine needle aspiration from omental thickening in one patient, and sputum positivity for AFB in one patient. Table 2 summarizes the diagnostic evaluation done for each of the patients.

Case 1. Axial CECT image showing perihepatic collections causing scalloping of the liver margins.

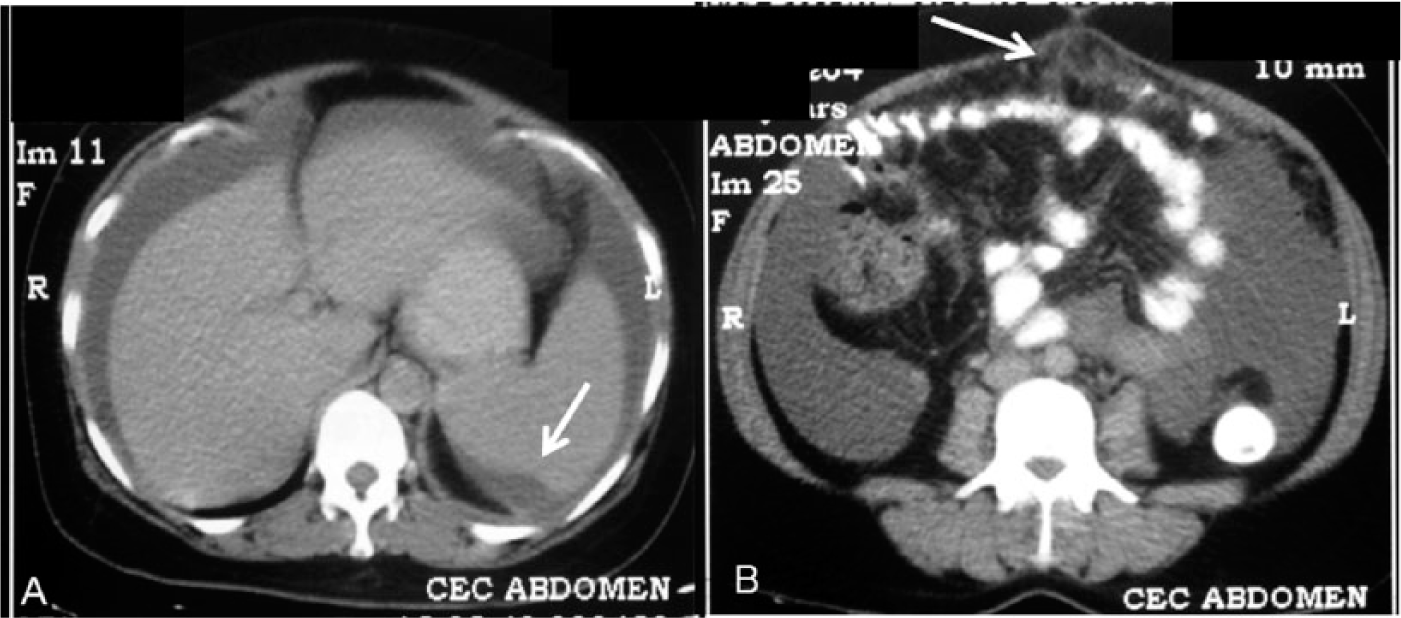
Case 2. Axial CECT images showing scalloping of the liver margins (arrow in a) with loculated ascites (both A and B), peritoneal fat stranding with thickening, and enhancement of the peritoneal lining (arrows in B).
Case 5. Axial CECT image showing scalloping of the splenic surface by perisplenic soft tissue (arrow in A), with ascites (seen in both A and B) and omental fat stranding (arrow in B).

Case 7. Axial CECT images showing loculated ascites with scalloping of liver margins (arrow in A), peritoneal soft tissue thickening and enhancement (arrow in B).
Clinical features of seven cases with visceral scalloping.

ATT, anti-tubercular therapy; F, female; HIV, human immunodeficiency virus; LOA/LOW: loss of appetite or loss of weight; NAD, no abnormality detected; NR, non-reactive; M, male.
Microbiological and histopathological findings.

ADA, adenosine deaminase; AFB, acid fast bacilli; FNA, fine needle aspiration; Nd, not done; Neg, negative; PCR, polymerase chain reaction; SAAG, serum ascites albumin gradient.
Findings of CT suggested presence of ascites in four patients, collections in five patients, lymphadenopathy in one patient, peritoneal involvement in four patients, pleural effusion in three patients, and ileo-cecal thickening in two patients (Table 3). All except one patient received standard anti-tubercular therapy (ATT) with four drugs initially for 2 months followed by two drugs for 4 months. One patient received ATT for 9 months. Pigtail drainage for collections was needed for two patients.
Computed tomographic findings in the seven patients with visceral scalloping.

Discussion
The scalloping of surface of visceral organs like liver is typically described in cases of peritoneal carcinomatosis and pseudomyxoma peritonei, but can be caused by other benign and malignant pathological conditions which may be due to diseases affecting the peritoneum and hepatic subcapsular region. 1
Carcinomas from the gastrointestinal tract (stomach, colon, appendix, gallbladder, and pancreas), ovary, breast, lung, and uterus may metastasize to the peritoneal surface. The imaging findings of peritoneal carcinomatosis vary from multifocal discrete nodules to infiltrative masses. Infiltration of the small bowel mesentery with carcinomatosis may produce characteristic pleated or stellate patterns that occur as the soft-tissue tumor replaces normal mesenteric fat. The term ‘pseudomyxoma peritonei’ is a clinical or radiologic description rather than a pathologic diagnosis. Pseudomyxoma peritonei (or jelly belly) is defined by the presence of copious, thick mucinous or gelatinous material on the surfaces of the peritoneal cavity. Mucin within the peritoneum is usually low in CT attenuation, but areas of soft-tissue attenuation may be present that represent solid tumor elements, fibrosis, or compression of the mesentery. 1 Scalloping of the visceral surfaces of the intraperitoneal organs is an important diagnostic finding that helps differentiate pseudomyxoma from simple ascites (exudative or transduative). It is most commonly observed along the margins of the liver and spleen. Pseudomyxoma peritonei does not invade visceral organs or spread by hematogenous routes. This is in contrast to tubercular involvement of the solid organs resulting in intraparenchymal granulomatous lesions.
The hepatic capsular and subcapsular regions may be affected by a variety of pathologic conditions, and pseudolesions can occur at the hepatic capsular and subcapsular regions. The pathologic conditions at these sites may be caused by infectious and inflammatory diseases (perihepatitis, parasitic diseases), infiltrative diseases (lymphoma, extramedullary hematopoiesis), and metastatic diseases (seeded metastasis, invasion via the perihepatic ligaments, direct invasion by malignancy from an adjacent organ). 2 Fluid, blood, and other benign and malignant entities may occupy the subcapsular space. A subcapsular hematoma appears as a low-attenuation, elliptic collection of blood between the liver capsule and the liver parenchyma. Scalloping may be caused by the compression of the underlying liver margin by the thick, fibrous Glisson capsule; in contrast, free intraperitoneal blood in the perihepatic space does not cause indentation or flattening of the underlying liver margin.
Peritoneal tuberculosis is the commonest form of abdominal tuberculosis and includes the involvement of the peritoneal cavity, mesentery, and omentum.4,5 The wet type of peritoneal tuberculosis presents primarily either as free or loculated ascites, and may be associated with diffuse and smooth peritoneal thickening, while in the dry type, there is a predominance of peritoneal and mesenteric thickening with caseous nodules, lymph node enlargement and fibrinous adhesions. The fibrous variety is characterized by remarkable omental thickening and entanglement of bowel loops clinically resembling a mass, occasionally with loculated ascites, which may be similar to peritoneal carcinomatosis.4,6 The most common CT findings in intraperitoneal tuberculosis include the following: (1) ascites (70–90% of cases); (2) smooth peritoneal thickening with marked enhancement after intravenous contrast injection; (3) densification of the mesenteric root fat planes, which may occur in up 70% of cases; and (4) lymph node enlargement with areas of central necrosis or calcification.6–8 On the other hand, the most frequent findings in peritoneal carcinomatosis include the following: (1) multinodular and irregular peritoneal thickening, (2) homogeneous retroperitoneal lymph nodes enlargement, and (3) omental caking.7,8
Only a few previous reports have compared the CT features of peritoneal tuberculosis with peritoneal carcinomatosis.9,10 Rodríguez and Pombo 9 compared 19 patients with peritoneal tuberculosis with 19 patients of peritoneal carcinomatosis and found that irregular thickening and peritoneal nodules suggested peritoneal carcinomatosis. Charoensak and colleagues. 10 in a report comparing 27 patients with peritoneal tuberculosis with 53 patients of peritoneal carcinomatosis suggested that presence of irregular peritoneal thickening and peritoneal nodules, omental nodularity and caking, and abnormal contour of visceral organs like the liver or spleen are suggestive of peritoneal carcinomatosis.
The present series describes visceral scalloping as a novel radiological finding in patients with abdominal tuberculosis. Therefore, the presence of visceral scalloping may not conclusively discriminate peritoneal carcinomatosis or pseudomyxoma peritonei from peritoneal tubercular involvement.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.