
Abstract
Chronic pain constitutes a significant burden to patients and healthcare systems. For many patients, the only option is to attempt to manage their pain within their daily lives. Here, we review evidence provided by three systematic reviews for the effect of diet and diet supplements on patients’ experience of chronic pain.
Introduction
Chronic pain is defined as pain that persists or recurs for more than 3 months. 1 Chronic pain is common in the United Kingdom, affecting up to 30%–50% of the population, 2 is self-reported in all adult age groups, ethnicities, and socioeconomic backgrounds, and is seen to increase in prevalence in later years of life. 3 Chronic pain is associated with reduced physical and mental health-related quality of life for patients and with negative impacts on social relationships and interactions in the workplace. 4 Healthcare resources feel a significant burden from chronic pain, with hundreds of millions of pounds spent annually by the NHS on pain conditions.5,6
The National Institute for Health and Care Excellence (NICE) recommends several evidence-based approaches for clinicians managing chronic pain in adults. 2 These include exercise programmes, psychological therapy, and acupuncture alongside antidepressant use if justified. 2 Due to limited evidence of efficacy, the use of benzodiazepines, non-steroidal anti-inflammatories, paracetamol, ketamine, opioids, local anaesthetics, or corticosteroids is not recommended in such scenarios. The NICE recommends research into alternative pain management strategies such as further types of psychological therapies, manual therapies, and social interventions (e.g. exercise and nutrition assessment).
It is known that chronic pain increases with Body Mass Index (BMI). 3 A higher BMI is also associated with an increased risk of back pain and musculoskeletal pain.7,8 Several systematic reviews have been published on different elements of dietary interventions for managing chronic pain.9–12 It is now timely to provide an overview of this evidence to help guide recommendations for patients. The three systematic reviews discussed in this commentary9–11 were selected on the quality of evidence reported for relevant pain outcomes (moderate to high).
Aims
This commentary aims to explore and critically appraise three systematic reviews by Crawford et al., 9 Field et al., 10 and Prego-Dominguez et al. 11 and expand upon the findings in the context to clinical practice (see Supplementary file 1 for methods, full results, and critical appraisal).
Commentary
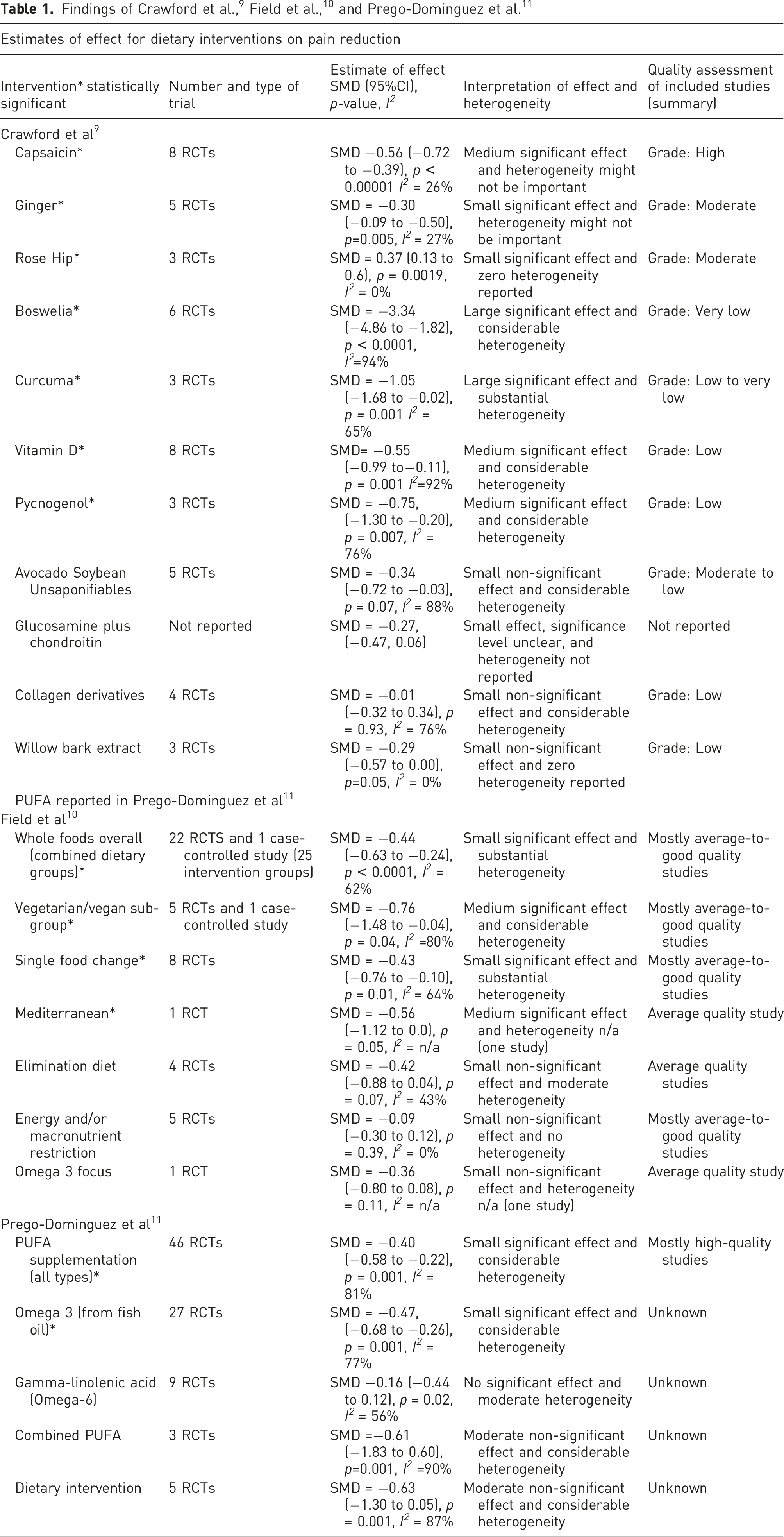
As there appears to be initial evidence for the beneficial effects of some diets and dietary supplements for use in chronic musculoskeletal pain, the results from these reviews present interesting possibilities for applications in practice.13–15 The attraction of these possible benefits is that supplementation is widely available (especially in the UK) without the need for a prescription. Capsaicin, Ginger, Rosehip, and Omega 3 are available as dietary preparations in most supermarkets or supplement shops. Where appropriate, and without evidence of negative health impacts, this is likely to sit well alongside other interventions planned for patients with chronic pain. For specific diets (e.g. Vegetarian and Vegan) this would have to be considered by individual patients as it may reflect a significant change in lifestyle that they are unwilling or unable to adopt. Consideration must additionally be given to the fact that dietary supplementation has the potential to represent a significant financial cost to patients. Chronic pain is more prevalent in areas of greater socioeconomic deprivation, 3 and it is acknowledged that this must be taken into account when educating patients on potential benefits.
Patient education (learning competencies and adapting behaviours) which is both multi-disciplinary and multi-dimensional has previously been described as having a beneficial impact for patients with chronic diseases, 16 and a similar approach may be appropriate in chronic pain. NICE guidance for practitioners on approaches to patient education in the prevention of obesity 17 remains relevant for dietary advice with chronic pain. The guidance highlights the importance of good communication between health professionals and patients and adds that advice should be non-discriminatory, culturally appropriate, written (where appropriate), and tailored to patients’ needs. Patient education that includes verbal teaching with visual media may also be beneficial. 18 Clinicians treating chronic pain will be aware of the subjective impact pain has on each patient and their lifestyle. As such, pain specialists should employ personalised recommendations on possible dietary changes based on individualised discussion for each patient, rather than rely on a set methodology.
Our commentary suggests that there is a gap in the research exploring the development of chronic pain and different types of diets. Despite the moderate-to-high-quality evidence available around the medicinal properties of many supplements, considerable variability exists in studies of this nature and more work is needed to identify dietary interventions that are effective. Future interventions should be well defined to determine the factors that influence the intervention such as vegan versus vegetarian versus non-vegetarian (white meat vs red meat), amount of salt, sugar, fat content, information provided, and mode/frequency of intake. Future research should also use standard reporting frameworks such as the template for intervention description and replication. 19 Furthermore, rather than using unidimensional pain assessments like the VAS and the Numeric Rating Scale, multi-dimensional pain assessment tools should be used to assess dietary interventions. Outcome measures should also consider the biopsychosocial context including physiological measures: physical functioning, development of chronic illness (diabetes and cardiovascular, fibromyalgia), psychological measures (anxiety, depression, and catastrophising), and social measures (family structure, wealth, eating habits, education, employment, and benefits). A longitudinal observational study (20–30 years) of young adults combining the abovementioned outcome measures would help to inform how diet can be changed to avoid or minimise certain pain conditions in the long term. In addition, future research should explore what are the mediating factors of the supplements (e.g. curcuma and its anti-inflammatory effect, specific diets, and reduction in BMI).
Supplemental Material
Supplemental Material - Pain and diet: A summary of the evidence for the role of diet modification in chronic pain
Supplemental Material for Pain and diet: A summary of the evidence for the role of diet modification in chronic pain by David Cameron, Joanna Harrison, Shiva Tripathi, and James Hill in British Journal of Pain.
Ethical statement
Ethical approval
Ethical approval was not sought for this article because it is not required for review articles.
Informed consent
Informed consent was not sought for this article because no individual patient details or results are utilised.
Footnotes
Acknowledgements
The research was partly funded by the National Institute for Health and Care Research Applied Research Collaboration North West Coast (NIHR ARC NWC) and supported by the NIHR Lancashire Clinical Research Facility. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Author contributions
S. T. conceived the review commentary. D. C., S. T., J. H., and J. H. researched the literature. All authors contributed to the first draft of the manuscript and future reviews. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was partly funded by the National Institute for Health and Care Research Applied Research Collaboration North West Coast (NIHR ARC NWC) and supported by the NIHR Lancashire Clinical Research Facility. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.