
Abstract
Objective
To examine differences in healthcare utilisation and costs associated with opioid prescriptions for non-cancer pain issued in primary care.
Method
A longitudinal, case-control study retrospectively examined Welsh healthcare data for the period 1 January 2005–31 December 2015. Data were extracted from the Secure Anonymised Information Linkage (SAIL) databank. Subjects, aged 18 years and over, were included if their primary care record contained at least one of six overarching pain diagnoses during the study period. Subjects were excluded if their record also contained a cancer diagnosis in that time or the year prior to the study period. Case subjects also received at least one prescription for an opioid analgesic. Controls were matched by gender, age, pain-diagnosis and socioeconomic deprivation. Healthcare use included primary care visits, emergency department (ED) and outpatient (OPD) attendances, inpatient (IP) admissions and length of stay. Cost analysis for healthcare utilisation used nationally derived unit costs for 2015. Differences between case and control subjects for resource use and costs were analysed and further stratified by gender, prescribing persistence (PP) and deprivation.
Results
Data from 3,286,215 individuals were examined with 657,243 receiving opioids. Case subjects averaged 5 times more primary care visits, 2.8 times more OPD attendances, 3 times more ED visits and twice as many IN admissions as controls. Prescription persistence over 6 months and greater deprivation were associated with significantly greater utilisation of healthcare resources. Opioid prescribing was associated with 69% greater average healthcare costs than in control subjects. National Health Service (NHS) healthcare service costs for people with common, pain-associated diagnoses, receiving opioid analgesics were estimated to be £0.9billion per year between 2005 and 2015.
Conclusion
Receipt of opioid prescriptions was associated with significantly greater healthcare utilisation and accompanying costs in all sectors. Extended prescribing durations are particularly important to address and should be considered at the point of initiation.
How this fits in
It is known that opioid analgesics can have long-term, harmful effects other than misuse and dependence. Previous studies examined the association between healthcare utilisation and the presence of opioid-induced adverse effects or misuse. This study examined the relationship between opioid prescribing for a range of pain-associated conditions and all-cause healthcare utilisation. Receipt of opioid prescriptions, particularly for durations of more than 6 months, were associated with a significant increase in healthcare utilisation and associated costs, when compared to a similar population who did not use opioid analgesics.
Introduction
Opioid prescribing has markedly increased in the United Kingdom (UK) since the early 2000s.1–8 In Wales, opioid prescribing rates rose 44% (from 692 to 994 prescriptions per 1000 population) between 2005 and 2015. 3 Reasons for the widespread use of opioids are manifold but rising prevalence of chronic non-cancer pain is often cited.10–13 A major contributor to continued opioid prescribing may be the paucity of non-pharmacological support to live more effectively with painful conditions.14–16 Socioeconomic costs of pain are substantial,17,18 with back pain estimated to cost the UK economy £10 billion per year. 19
The focus of discussion around opioid prescribing is commonly the risk of dependence and misuse.20–24 Studies examining healthcare utilisation and costs associated with opioid misuse disorders25,26 found that incremental healthcare costs associated with prescription opioid misuse in Europe were estimated between €900 to €2551 per person per year, with annual healthcare costs up to €279,927 per 100,000 population. 23
Other harms of opioids especially when used at high dose and for longer durations have been acknowledged.27,28 Adverse effects such as constipation, nausea, vomiting and sedation are well known, identified and managed routinely, whatever the underlying pain-related diagnosis.29–32 Other harms of opioid analgesics include endocrine disorders, 33 depression,34,35 respiratory depression,36,37 sleep impairment, 38 falls and fractures,39–41 which, whether or not recognised as related to opioid use, will require additional healthcare intervention and support.
Our study is the first to compare healthcare resource utilisation and associated costs, in a large cohort of people with recorded pain-related diagnoses where case subjects were receiving opioid prescriptions and control subjects were not, in Wales between 2005 and 2015. The findings of our study highlight a potential consequence of opioid analgesic prescribing which is not often discussed. It provides a baseline on which to develop further research to examine how opioid-related healthcare utilisation and costs may be mitigated within a system of scant resource.
Method
Study design and data source
A retrospective, longitudinal case-control study design was used. Individual’s anonymised data were extracted from the Secure Anonymised Information Linkage (SAIL) databank, part of the national e-health records research infrastructure for Wales.42,43 Each individual with records in the SAIL databank was allocated a unique anonymised linkage field (ALF) number allowing cross-linking between different datasets. Data from all individuals aged 18 years and over, without a recorded diagnosis of cancer between 2004 and 2015 on their primary care medical record was included in the primary data extraction.
Data were taken from the Welsh longitudinal general practice (WLGP) source, downloaded directly from electronic health records in GP practices around Wales; the Welsh demographic service dataset (WDSD); patient episode database Wales (PEDW) which records all inpatient (IN) and day-case hospital activity; emergency department (ED) and outpatient (OPD) data, which is collated by Digital Health and Care Wales (previously National Health Service (NHS) Wales Informatics Service, NWIS). 44
Cohort identification
Read codes, a thesaurus of clinical terms used to record interactions, diagnoses and interventions in Primary Care settings, were used to identify the case and control cohorts using the NHS Information Authority’s Clinical Terminology Browser and accessed via the SAIL secure gateway. Read codes for six commonly occurring conditions associated with persistent pain, rheumatoid and osteoarthritis, neck and back pain, fibromyalgia and neuropathic pain, were compiled
Opioid prescription identification
Read codes were compiled for all oral and transdermal opioid medicines commonly prescribed as analgesics in Wales, as previously described
3
(Supplementary file 2
Identification of case and control subjects
During dataset preparation, searches found 657,243 subjects with the defined, non-cancer conditions listed on their primary care medical record during the study period and who had received at least one prescription for an opioid analgesic between 2005 and 2015. That group was classified as case subjects. There were 101,176 who matched case subjects by pain-diagnosis, gender, age and deprivation score but did not receive opioid prescriptions and so were used as control subjects. Consequently, every control subject was matched to multiple case subjects, a method recommended by SAIL and described in the literature. 47 For example, if a control subject had 6 years of medical records without receiving an opioid prescription, they could potentially be matched to case subjects who had received opioid analgesic prescriptions for any period up to 6 years. This effectively provided 2,628,972 control subjects.
Prescription persistence
At the time of the study, SAIL was not able to access data on dose instructions or quantity of medicine prescribed in Primary Care. Those variables can be used to estimate daily dose and the likely duration of the prescription. 1 An estimated measure was therefore developed, considering recommendations that the quantity of medicine given on a controlled drug prescription should not exceed more than 30 days’ supply. 46 In the absence of prescribed quantity, it was assumed that if prescriptions were issued to the same individual within 31 days of each other, it was more likely the individual was consistently using opioid analgesics. The duration of 31.5 days maximum between prescriptions as a marker of continuous prescribing in large datasets was previously described by Braden et al. {Braden.2010}. The duration between each prescription issued to any individual was calculated using the recorded ‘event dates’ from the Primary Care General Practice (GP) dataset. Prescribing persistence (PP) was calculated as the number of days of consecutive prescriptions, when subsequent prescriptions were issued within 31 days of each other. If the period between prescriptions was longer than 31 days, it was classed as a new period of prescribing. Case subjects were stratified by PP of less than or more than 6 months.
Statistical analysis
Case subjects’ data were collected from the first opioid prescription until 31 days after the last recorded issue or until death and compared to control subjects’ data for the same duration. Healthcare attendances, tests and investigations for the period opioid prescriptions were received for each subject were counted, totalled and compared.
Due to the large sample size in both arms of the study (case and control), we determined parametric tests could provide accurate analysis. Central limit theorem suggests when sample size is large, distribution tends to normal even if the population itself is not normally distributed.4,48 Analysis was undertaken using SPSS version 26. 45 Descriptive statistics were used to compare case and control groups. We used two-way analysis of variance (ANOVA) to examine inter-dependence of different variables, for example, male-female and case-control. An interaction effect between factors was deemed significant at 5%. Where there was significant interaction, univariate tests (independent t-test or one-way ANOVA) were conducted, with a significance level of 5%. Bonferroni–Holm sequential corrections were used to adjust for Type I error rate inflation in multiple comparisons. 46
Linear regression
Multiple linear regression analyses were used to predict which, if any, variables affected attendance in Primary Care (number of appointments) as well as OPD, ED or IP attendances. The factors used to make the predictions were opioid prescription, age, gender, deprivation status (WIMD2011), recorded diagnosis of depression and/or anxiety and whether an opioid prescription was issued or not, where prescriptions were issued and if they persisted for less or more than 6 months.
Cost analysis
Cost analysis was undertaken from a UK NHS perspective. Costs included primary care GP attendances, staff time, tests, investigations and imaging, ED and OPD department attendances and IP admissions which included day/night charges and excess day charges. Weighted average costings were calculated from nationally available standard NHS unit costs for 201551,52 taking account of the number of attendances in each area (e.g. outpatient department, inpatient admission) and the nature of said attendance (e.g. elective, or non-elective admission; Supplementary files 3 & 4). General practice attendance costs were weighted according to published data giving standardised proportions of attendances with general practitioners compared to other professionals in Primary Care, such as nurses. 49 Data were not available to calculate drug costs.
Research approvals
This research was approved by the Information Governance Review Panel (IGRP) of the Secure Anonymised Information Linkage databank (SAIL), based in Swansea University (SAIL identification number: 0507).
Patient and public involvement statement
There was no direct patient involvement in development and design of this study. However, the SAIL databank has members of the public who provide advice and give recommendations on safeguarding and ethical approval via a Consumer Panel. Panel members also provide input to the IGRP, which approves all data applications.
Results
Overall healthcare utilisation
Characteristics of the two groups of study subjects.
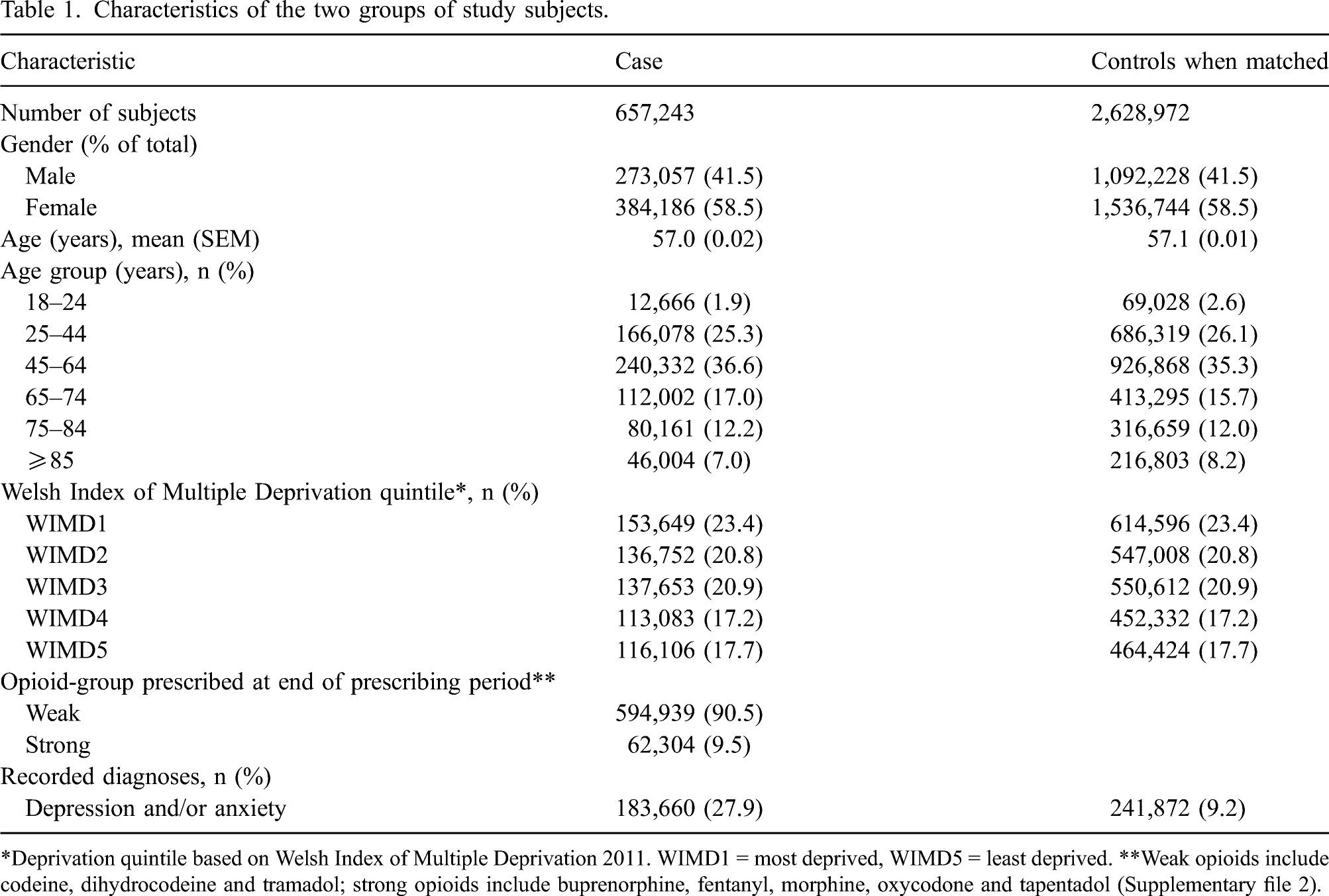
*Deprivation quintile based on Welsh Index of Multiple Deprivation 2011. WIMD1 = most deprived, WIMD5 = least deprived. **Weak opioids include codeine, dihydrocodeine and tramadol; strong opioids include buprenorphine, fentanyl, morphine, oxycodone and tapentadol (Supplementary file 2).
Comparison of healthcare utilisation between case subjects (in receipt of opioid prescriptions) and controls (no opioids) between 2005 and 2015.
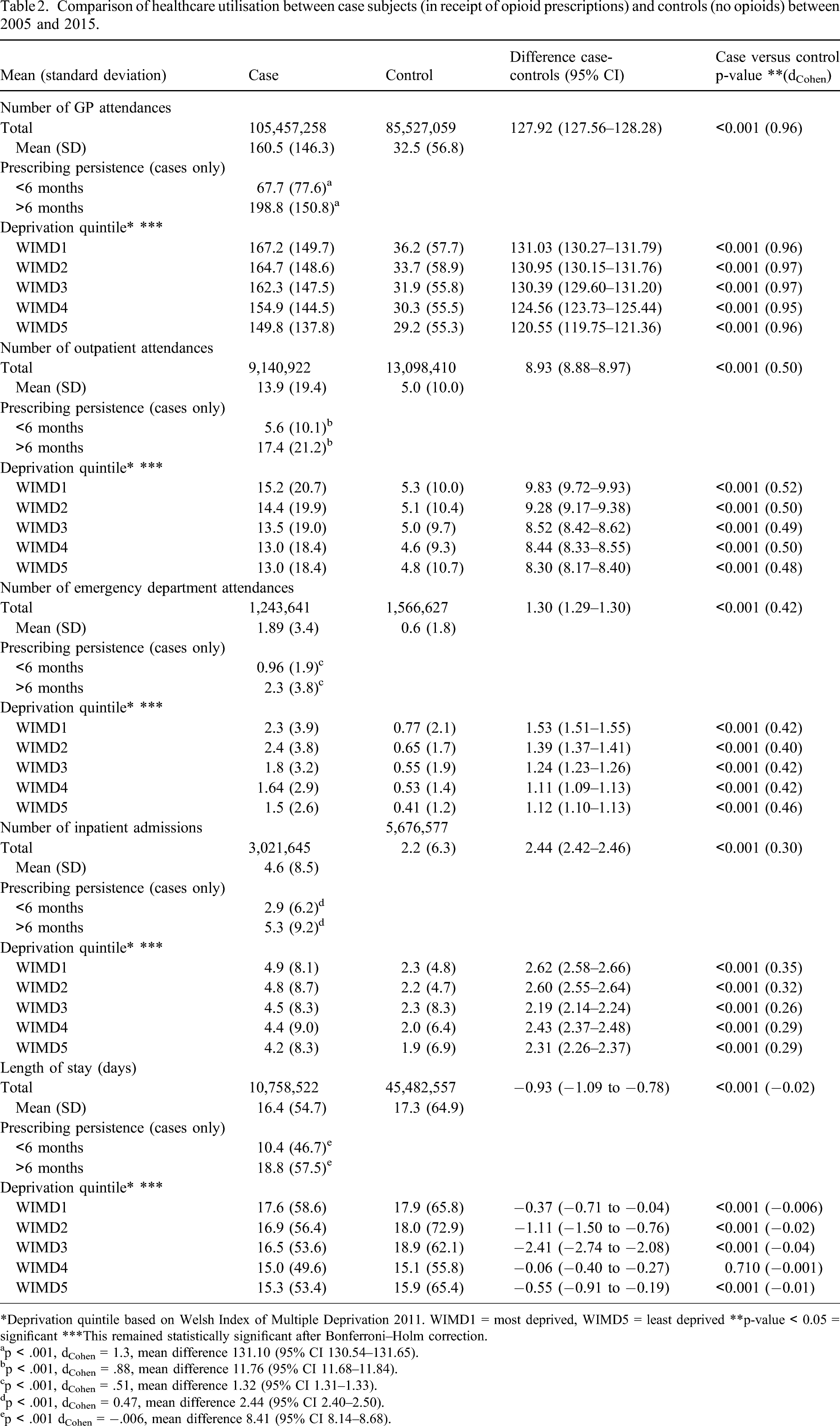
*Deprivation quintile based on Welsh Index of Multiple Deprivation 2011. WIMD1 = most deprived, WIMD5 = least deprived **p-value < 0.05 = significant ***This remained statistically significant after Bonferroni–Holm correction.
ap < .001, dCohen = 1.3, mean difference 131.10 (95% CI 130.54–131.65).
bp < .001, dCohen = .88, mean difference 11.76 (95% CI 11.68–11.84).
cp < .001, dCohen = .51, mean difference 1.32 (95% CI 1.31–1.33).
dp < .001, dCohen = 0.47, mean difference 2.44 (95% CI 2.40–2.50).
ep < .001 dCohen = −.006, mean difference 8.41 (95% CI 8.14–8.68).
Emergency department attendance was three times more frequent for people receiving opioid prescriptions (1.89 vpp) than controls (0.6 vpp, p < 0.001). Case subjects had twice as many hospital admissions as controls (4.6 vs 2.2 admissions per person (app), p < 0.001)
Healthcare resource utilisation associated with PP
Opioid PP of more than 6 months (long-term) was associated with a significant increase in healthcare utilisation, compared to durations less than 6 months (short term) or controls Comparison of healthcare utilisation stratified by PP of greater or less than 6 months and compared to control subjects (not prescribed opioid analgesics). Insert: detail of resource utilisation comparison for outpatient, ED attendances, inpatient admissions and length of stay (given in days). Note: PP: prescribing persistence; ED: emergency department;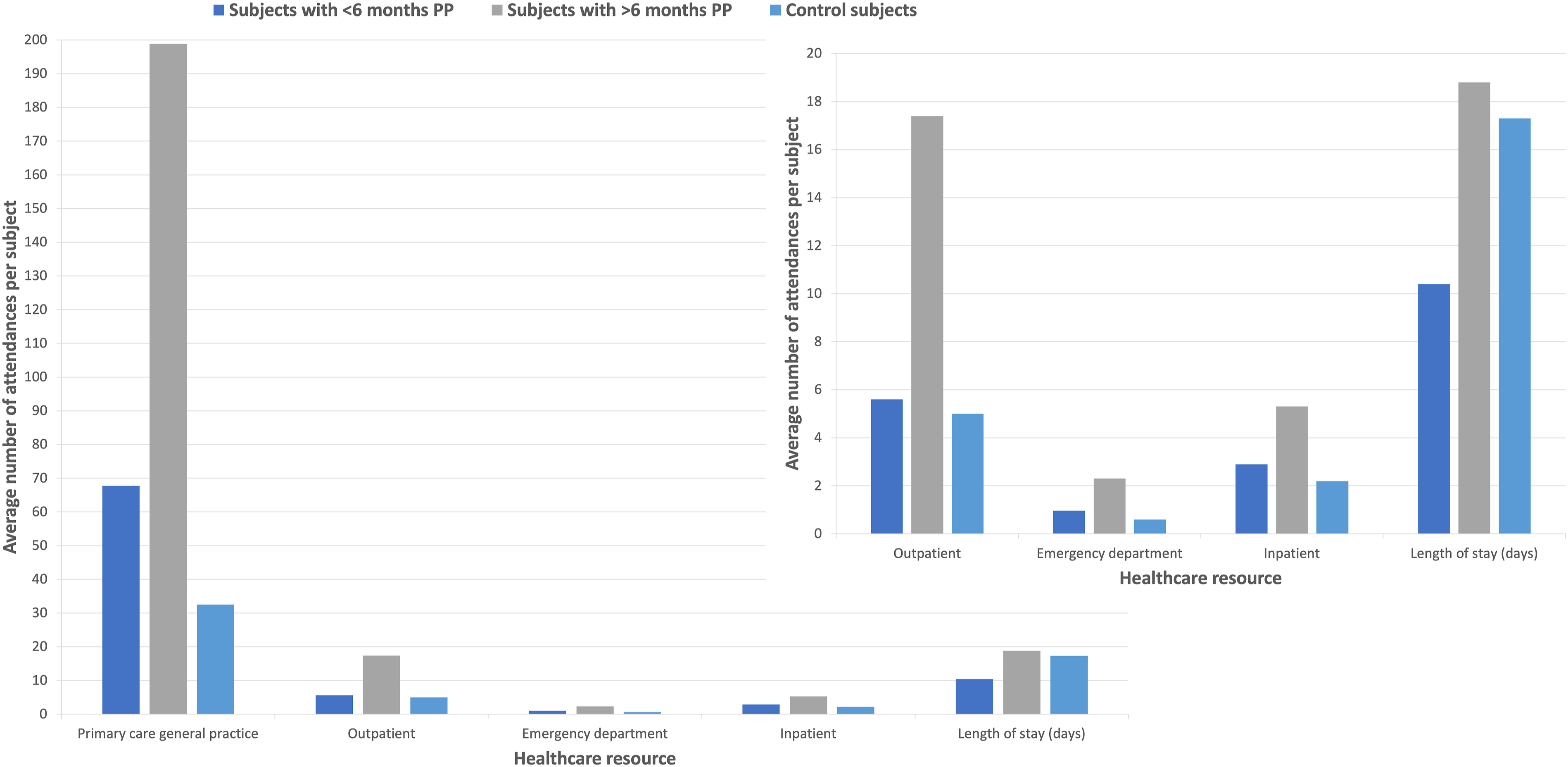
Long-term use was associated with 2.8 times more OPD appointments (17.4 vs 5.6 vpp) and 2.4 times more ED. attendances (2.3 vs 0.96 vpp) than short term. Inpatient admissions were 1.8 times more frequent with long-term (5.3 app) than short-term opioid use (2.9 app).
Healthcare resource utilisation associated with differing levels of socioeconomic deprivation
Statistically significant, albeit empirically modest differences, increases in healthcare attendance with rising deprivation (Table 2 Comparison of healthcare utilisation by socioeconomic deprivation using Welsh Index of Multiple Deprivation 2011 (WIMD2011). WIMD1 = most socioeconomically deprived, WIMD5 = least socioeconomically deprived.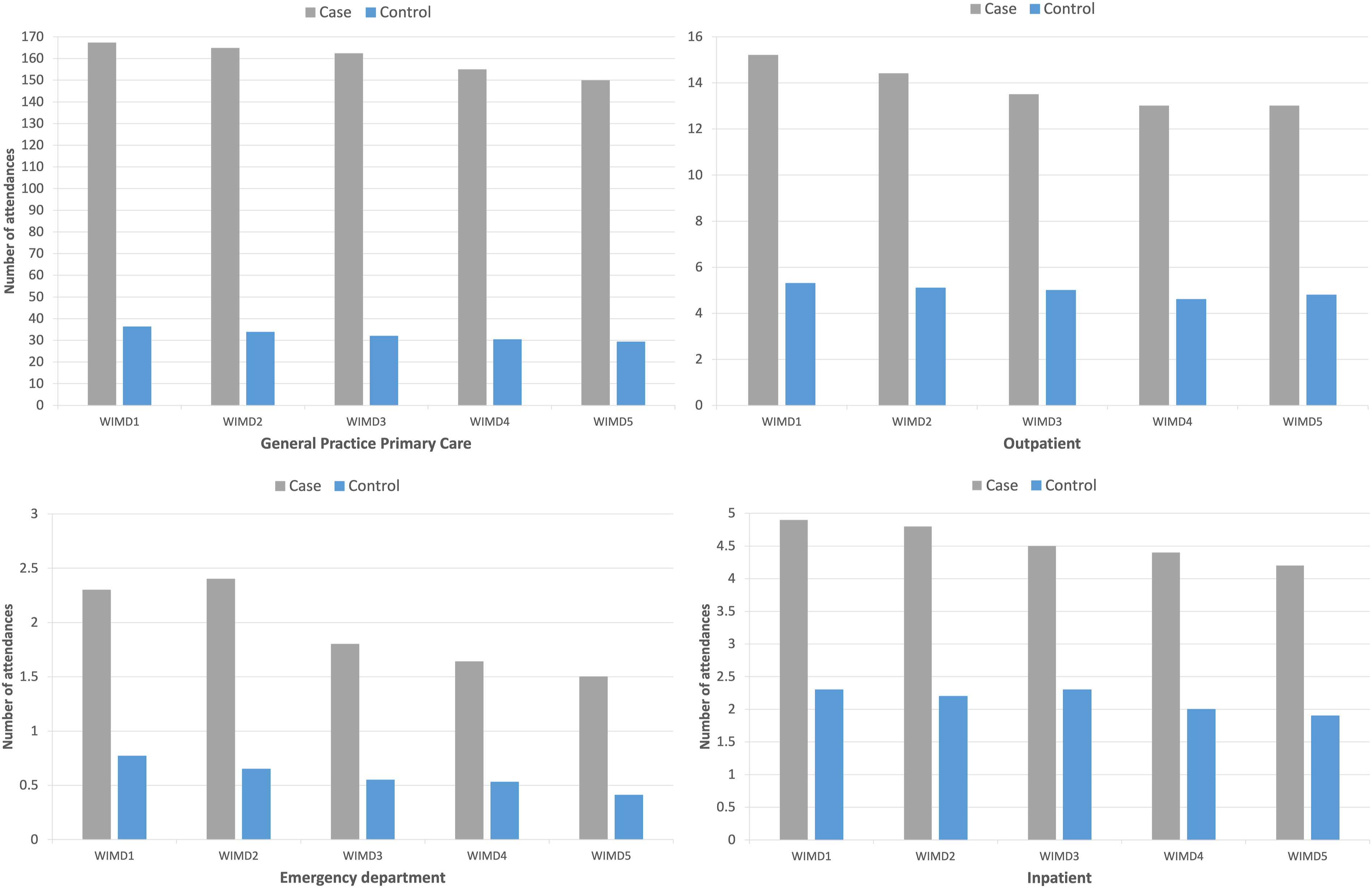
Case subjects had around 1.5 times more ED. visits recorded (2.3 vpp) in the most deprived quintiles compared the least deprived (1.5 vpp, p < 0.001) with similar differences noted in the control group
Factors associated with healthcare use
Multiple linear regression results indicated that the model was a good predictor of the number of attendances in Primary Care (GP). An R2 of 0.457, SE = 71.75 (R = 0.676), meant 45.7% of the variation in the original data could be explained by the model. The models for predicting factors contributing to outpatient attendance (R2 = 0.134, SE = 12.08), ED attendance (R2 = 0.081, SE = 2.14) and inpatient admission (R2 = 0.047, SE = 5.51) were less reliable.
Output from multiple linear regressions to predict number of healthcare attendances.
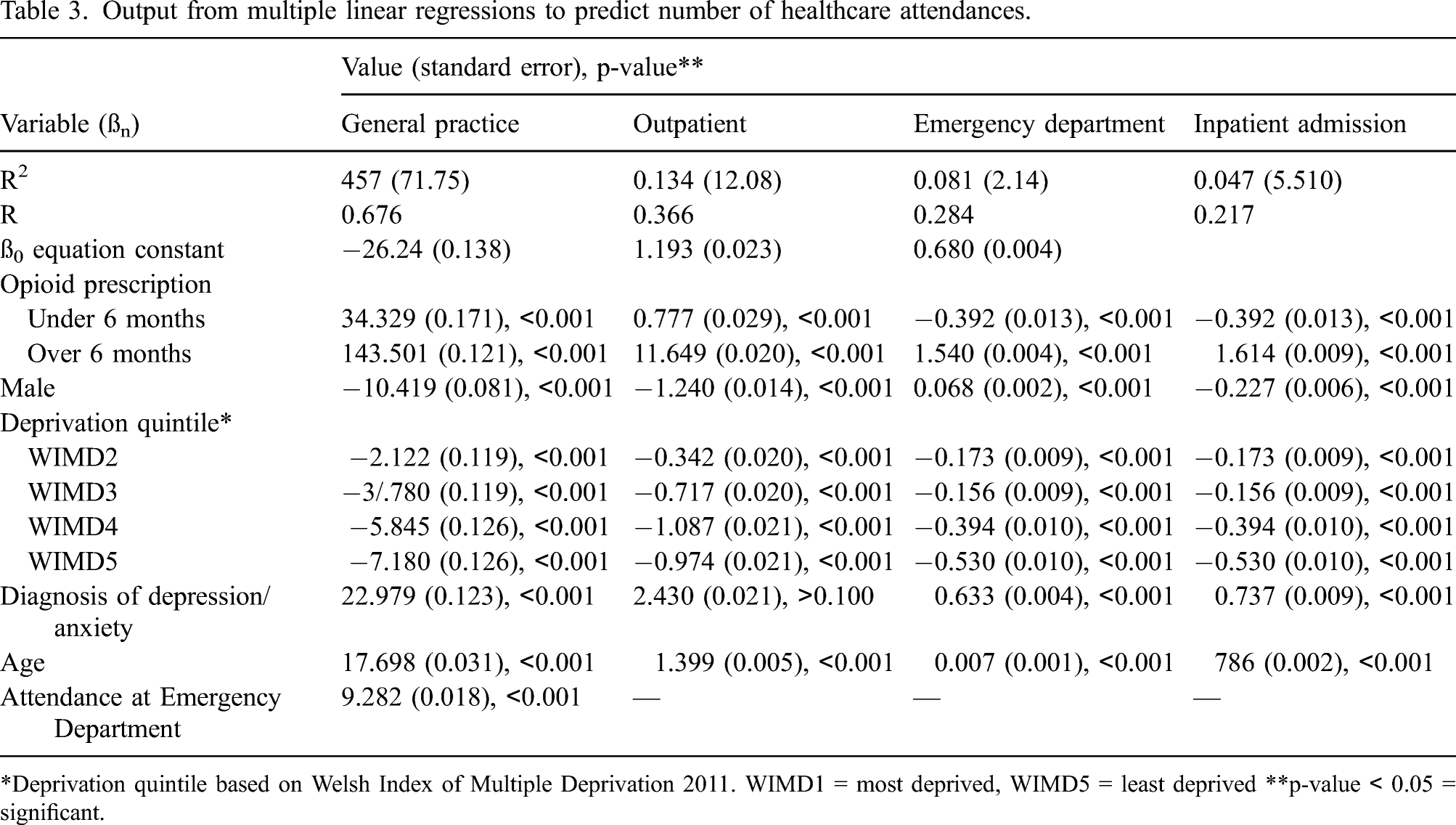
*Deprivation quintile based on Welsh Index of Multiple Deprivation 2011. WIMD1 = most deprived, WIMD5 = least deprived **p-value < 0.05 = significant.
Cost analysis
The average cost of healthcare utilisation was estimated to be £11,096.49 per person (pp) for the study period Average costings for healthcare utilisation comparing all subjects within the study, cases and controls. *p-value calculated from t-test (case-control), <0.05 = significant Bonferroni–Holm tests confirmed it was correct to reject the null hypothesis **Deprivation quintile based on Welsh Index of Multiple Deprivation 2011. WIMD1 = most deprived, WIMD5 = least deprived.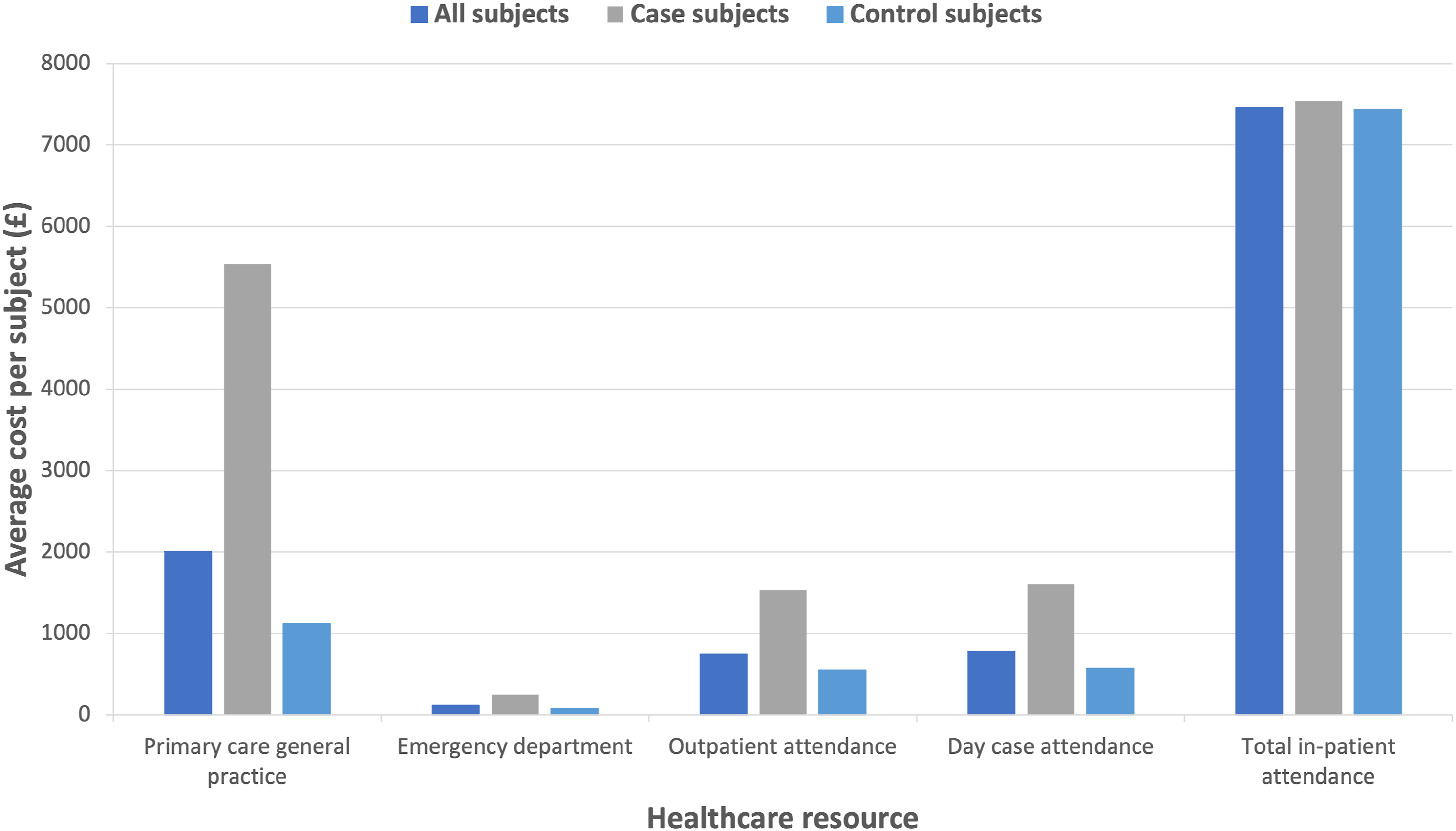
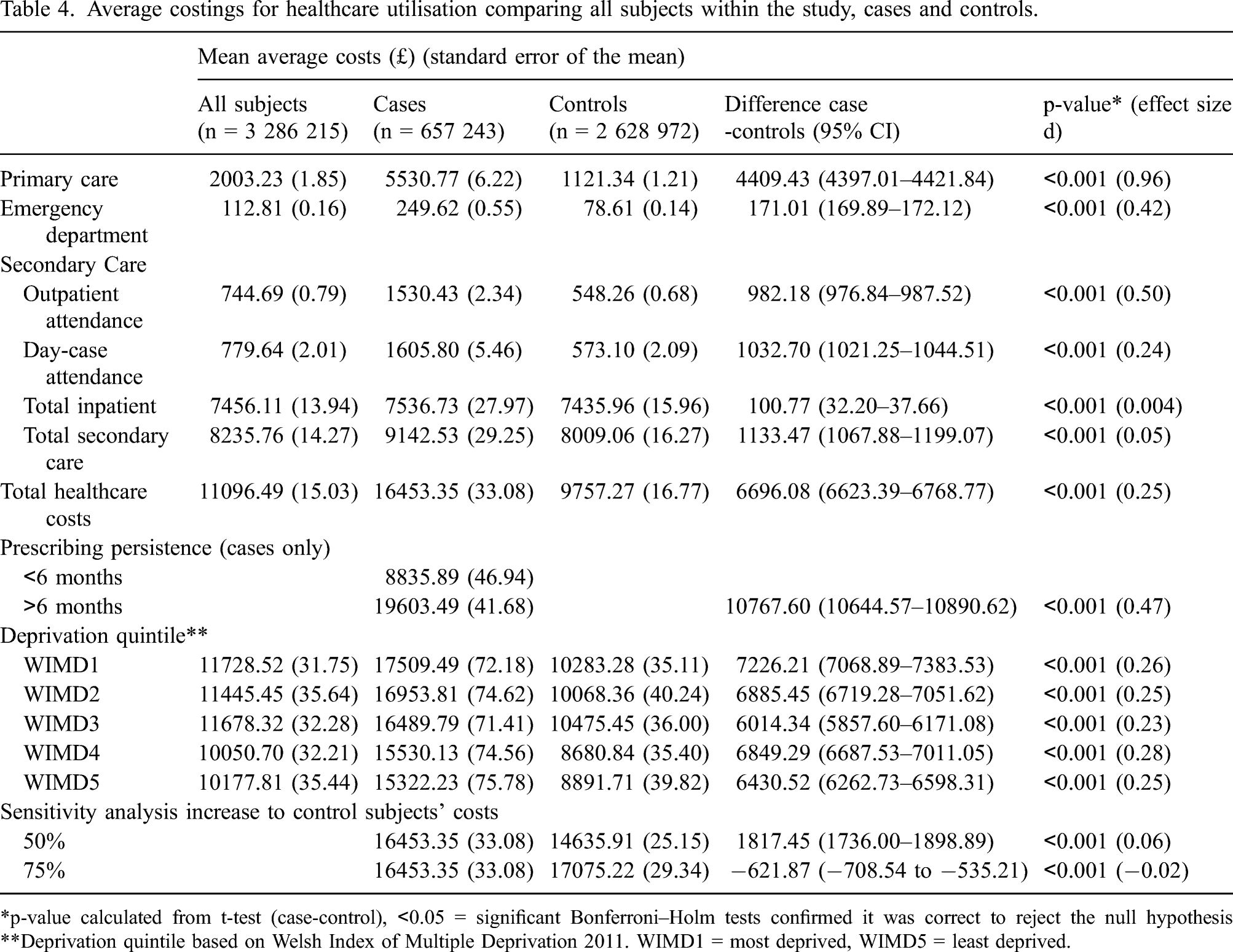
One-way sensitivity analysis confirmed an increase in healthcare utilisation and its consequent costs, of more than 1.5 times (50% increase) would be required in the control group, to become equivalent to the averages noted in case subjects
Discussion
Summary
We used a large dataset to examine differences in healthcare utilisation in two diagnostically matched cohorts, who either received, or did not receive, opioid analgesic prescriptions. Significantly more appointments for people prescribed opioids were noted in all healthcare sectors, when compared to people with similar medical history but not prescribed opioid analgesics. Prescribing persistence of more than 6 months was most strongly associated with increased healthcare utilisation and consequent costs. Receiving opioid prescriptions and living in areas of high socioeconomic deprivation appeared associated with greater healthcare utilisation than high levels of deprivation alone.
The cost analysis undertaken suggests that a large reduction in healthcare utilisation amongst individuals prescribed opioids would be required in order to bring costs in-line with people who are not prescribed opioid analgesics, despite similar conditions. These results are important given the high burden of opioid prescribing in Wales, 3 the UK more widely,2,5,54 and the concerns expressed about opioid-induced long-term harms.32,55–57
Comparison with existing literature
Increased healthcare utilisation following the initiation of opioids has been reported across the world.55–60 Healthcare use increased following the first prescription for opioid therapy, with costs further influenced by the drug prescribed in a German cohort. 55 Studies have found that whilst healthcare utilisation, and therefore costs, increase significantly following initiation, it appears to reduce with persistent prescribing, although not to pre-prescription levels.59,61 Chang and colleagues observed greater total healthcare costs for people receiving long-term opioids than people with a diagnosed opioid-use disorder {Chang:2018}.
2 US study reported twice as many healthcare interactions for chronic opioid use (>180 days) compared to acute use (less than 10 days), 62 which compares to our study, where long-term users had 3 times as many GP and OPD visits and twice as many visits to ED compared to short-term users. Thornton et al. (2018) showed similar increases in inpatient in the first 120 days after initiation for individuals who received at least 90 consecutive days of opioid analgesics (from 1.5% to 10.9% of those prescribed chronic opioids compared to 1.1%–5.4% of non-chronic prescribing). 58
Comparing costs between the United Kingdom and other countries can be hampered by differences in healthcare systems and the manner by which tariffs are determined. The increased healthcare utilisation and associated costs demonstrated in our study are, however, consistent with other studies’ findings among people prescribed opioid analgesics.59,61,62
Strengths and limitations
Our study is the first to examine the association of opioid analgesic prescribing and overall healthcare utilisation in Wales. The SAIL databank allows access to data for 78% of the Welsh population and our study included more than two million subjects, so is highly likely to be representative of the population.
Limitations were in part, due to restrictions in data availability and extraction. Matching of case and control subjects used a method advocated by SAIL 63 but was hampered by the disproportionate number of individuals with the diagnoses of interest also receiving opioid analgesic prescriptions. Further research is needed in Wales, to provide more detailed analysis, controlling for non-pain comorbidities, to accurately determine the impact of prescribed opioid use on the type of health care accessed.
Lists of read codes had to be scaled down to meet the workload capacity of the databank employees who undertake the data extraction and this likely led to underestimation of healthcare utilisation. For example, it was not possible to differentiate between the type of admission (e.g. elective, or non-elective) or the admission diagnosis recorded. Further research is needed to determine more accurate associations between opioid prescribing, investigations and all-cause healthcare utilisation.
The SAIL databank did not have access to community pharmacy dispensing data, which precluded medication costs in the analysis. Whilst we used a measure of prescription persistence described in other studies,43,58 we acknowledge timings of prescriptions do not confirm continued use by the individual and so are an estimate. Improved access to information on dose and quantity of opioid analgesics prescribed would provide a more accurate assessment of PP. Prescribing data suggests intention to treat but does not identify the dose or quantity of medicine prescribed nor confirms consumption. Quality of life measurements are not routinely recorded in practice, so further research is needed to develop cost-utility analyses.
Future research to examine the relationship between the duration of opioid use and the timing of changes in healthcare utilisation could provide insight into safe durations of opioid use, which would positively impact clinical guidance. In addition, it would be useful to identify if people who have stopped using opioid analgesics see a corresponding reduction in their use of healthcare services.
Conclusions
Our results show a likely association between the receipt of opioid analgesic prescriptions and increased healthcare utilisation and costs for people living with commonly occurring conditions such as back pain, osteoarthritis and fibromyalgia. Some individuals prescribed opioids may be more unwell than those who do not receive them, so further investigation of whether the use of opioid analgesics is potentiating underlying health conditions would be beneficial. Long-term and high-dose opioid analgesic use has been associated with higher levels of pain reporting and worse outcomes60,64,62 including self-reported poor general health, 60 depression35,65 and polypharmacy. 66 This is especially pertinent in Wales, a country where an estimated 23% of the population live in poverty, 67 61% are overweight or obese 68 and an average 26 prescriptions for any medicines are issued annually, per head of population compared to 19.9 prescriptions per head in England. 69
Given concerns about high levels of opioid use in the United Kingdom and internationally, consideration of the wider impact on people’s health that opioids may have is possibly as important as the well-publicised concerns about misuse and dependence. This could be especially pertinent in the wake of the COVID-19 pandemic, when people living with long-term, painful conditions might expect delays to treatment or intervention. Practitioners in all sectors of healthcare provision may find themselves under greater pressure to provide analgesic medicines, whilst individuals wait to be seen elsewhere. Additionally, some reported symptoms of long-COVID 68 are very similar to widespread pain conditions like fibromyalgia, which is known not to respond well to opioids in most cases69,70 but where opioids are often still given, perhaps due to the paucity of timely alternatives. 10 The decision to initiate opioid analgesics must be carefully weighed with potential risks of increasing healthcare need, rather than reducing it, unless regular review and limiting duration of use can be supported.
Supplemental Material
sj-pdf-1-bjp-10.1177_20494637211045898 – Supplemental Material for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015
Supplemental Material, sj-pdf-1-bjp-10.1177_20494637211045898 for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015 by Emma Davies, Ceri J Phillips, Mari Jones and Bernadette Sewell in British Journal of Pain
Supplemental Material
sj-pdf-2-bjp-10.1177_20494637211045898 – Supplemental Material for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015
Supplemental Material, sj-pdf-2-bjp-10.1177_20494637211045898 for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015 by Emma Davies, Ceri J Phillips, Mari Jones and Bernadette Sewell in British Journal of Pain
Supplemental Material
sj-pdf-3-bjp-10.1177_20494637211045898 – Supplemental Material for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015
Supplemental Material, sj-pdf-3-bjp-10.1177_20494637211045898 for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015 by Emma Davies, Ceri J Phillips, Mari Jones and Bernadette Sewell in British Journal of Pain
Supplemental Material
sj-pdf-4-bjp-10.1177_20494637211045898 – Supplemental Material for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015
Supplemental Material, sj-pdf-4-bjp-10.1177_20494637211045898 for Healthcare resource utilisation and cost analysis associated with opioid analgesic use for non-cancer pain: A case-control, retrospective study between 2005 and 2015 by Emma Davies, Ceri J Phillips, Mari Jones and Bernadette Sewell in British Journal of Pain
Footnotes
Acknowledgements
This study makes use of anonymised data generated by the Secure Anonymized Information Linkage (SAIL) system, which is part of the national e-health records research infrastructure for Wales. We would like to acknowledge all the data providers who make anonymised data available for research.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Pharmacy Research UK grant number PRUK-2016-PA1-A. ED’s PhD is partly supported by funding from Research Capacity Building Collaboration (RCBC Wales).
Ethical approval
Ethical approval (include full name of committee approving the research and if available mention reference number of that approval): Ethical approval was not sought for the present study because the SAIL databank provides anonymised person level data with means of identification removed prior to submission to the databank. The Information Governance Review Panel (IGRP) of SAIL quality assures all applications for access and considers ethical implications prior to study approval. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Guarantor
E.D
Contributorship
ED. conceived of and designed the study, collated the read codes used for data extraction, coded the extracted data, undertook the data analysis, drafted and revised the article. MJ, CP and BS oversaw the study design and data analysis and critically revised the article. All authors read and approved the final article.
Supplementary material
Supplementary Material is available for the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.