
Abstract
Objective:
The objective of this study is to develop an update of the evidence-based guidelines for the management of pain in older people.
Design:
Review of evidence since 2010 using a systematic and consensus approach is performed.
Results:
Recognition of the type of pain and routine assessment of pain should inform the use of specific environmental, behavioural and pharmacological interventions. Individualised care plans and analgesic protocols for specific clinical situations, patients and health care settings can be developed from these guidelines.
Conclusion:
Management of pain must be considered as an important component of the health care provided to all people, regardless of their chronological age or severity of illness. By clearly outlining areas where evidence is not available, these guidelines may also stimulate further research. To use the recommended therapeutic approaches, clinicians must be familiar with adverse effects of treatment and the potential for drug interactions.
Key points
Always consider the use of non-pharmacological strategies such as physiotherapy, cognitive behavioural approaches, TENS and acupuncture, to reduce or eliminate the need for medicines.
Physiological changes in older people increase the sensitivity to some analgesic drugs, which might necessitate appropriate dose titrations or replacement with an alternate medicine.
The incidence of side effects with drug therapy is higher in older people, particularly in the presence of co-morbidities and polypharmacy. These factors need to be carefully considered when introducing new medication to minimise the chance of drug–disease and drug–drug interactions.
Always consider the route of administration. Although the oral route is preferred, as it is convenient and the least invasive, topical treatments may have similar efficacy to other routes with fewer adverse events.
Timing of medicine administration is important. Consider rapidly acting formulations with shorter half-lives for severe, episodic pain. This may need to be balanced with more regular background analgesia for patients who experience continuous pain and modified release formulations may improve adherence.
Only start or change one medicine at a time. Start with a low dose, use a slow dose titration and allow sufficiently long intervals to allow the assessment of effect. Treatment should be monitored regularly and, if required, adjusted to improve effectiveness and limit adverse events.
Combination therapy may be considered. Drugs with complementary mechanisms of action may have synergistic effects to provide greater pain relief with fewer side effects than higher doses of a single drug.
Introduction
Ageing is associated with increasing risk of functional impairment and incidence of disease. With these factors, older people carry an additional potential burden of experiencing chronic pain.
The aim of this project was to update the 2013 Guidelines for the Management of Pain in Older People 1 developed by the British Geriatrics Society and The British Pain Society.
The objectives were
To describe the population and current prevalence.
To address current international guidelines.
To identify literature regarding attitudes and beliefs held by health professionals and informal carers.
To identify evidence regarding pharmacological and non-pharmacological management.
To identify evidence regarding palliative pain (pain associated with life-threatening illness) for this population.
Review and consensus methodology
A team of health professionals and experts in pain management, comprising representatives from epidemiology, geriatric medicine, pain medicine, nursing, physiotherapy, occupational therapy, psychology, pharmacology and service users, was formed to initiate a systematic review and provide an update on the 2013 publication. 1 The team included members of the British Geriatric Society, British Pain Society and Royal College of Nursing.
Search areas and terms to develop and complement the search undertaken in the previous guidelines as completed in 2010 were established. Key terms associated with each area were considered for an initial generic search of published literature. This initial search was undertaken with the assistance of an information scientist, and a database of potential evidence was established using the bibliographic software Refworks (ProQuest, Michigan, USA).
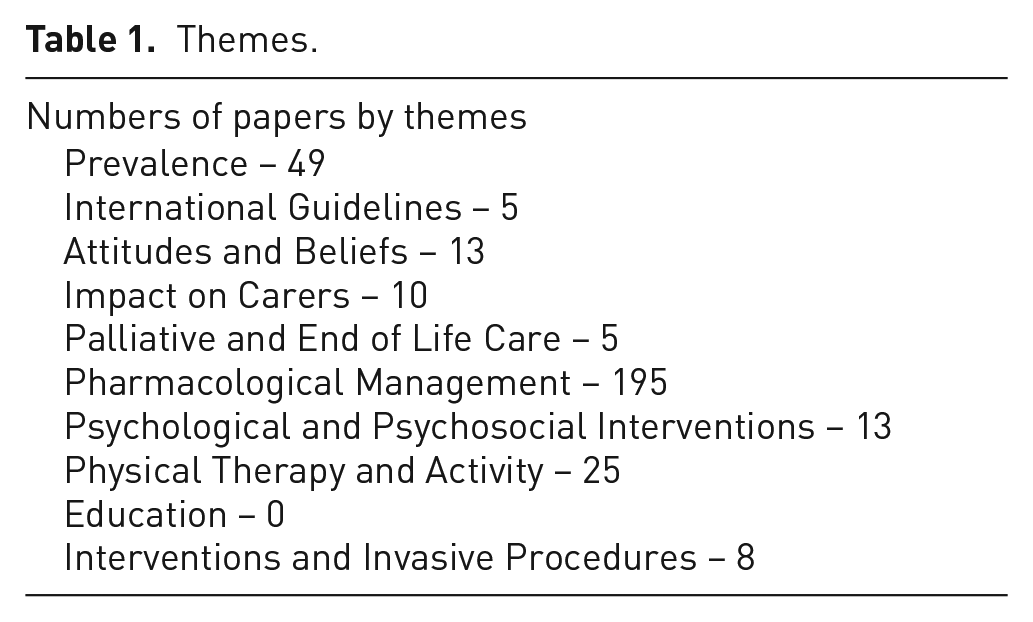
Thematic groups were established to review the lists of available literature associated with particular areas of expertise. Thematic areas included (1) Pain Prevalence, (2) International Guidelines, (3) Attitudes and Beliefs, (4) Impact on Carers, (5) Palliative and End of Life Care, (6) Pharmacological Management, (7) Psychological and Psychosocial Interventions, (8) Physical Therapy and Activity, (9) Education and (10) Interventions and Invasive Procedures (Table 1).
Themes.
Methods
A systematic search strategy (Table 2) was undertaken using both Boolean search and proximity operators in May 2018 including papers published between 2009 (the date of the last review) and March 2018 (inclusive). Reference lists of papers and review articles were also searched for possible inclusions. The process of development of this article followed the reporting guidelines identified by Moher et al. 2 and the quality of included papers was assessed using the Scottish Intercollegiate Guidelines Network methodological grading system. 3 Thus, each paper was assigned a quality score and peer reviewed for appropriate incorporation into matrices of papers.
Search strategy.
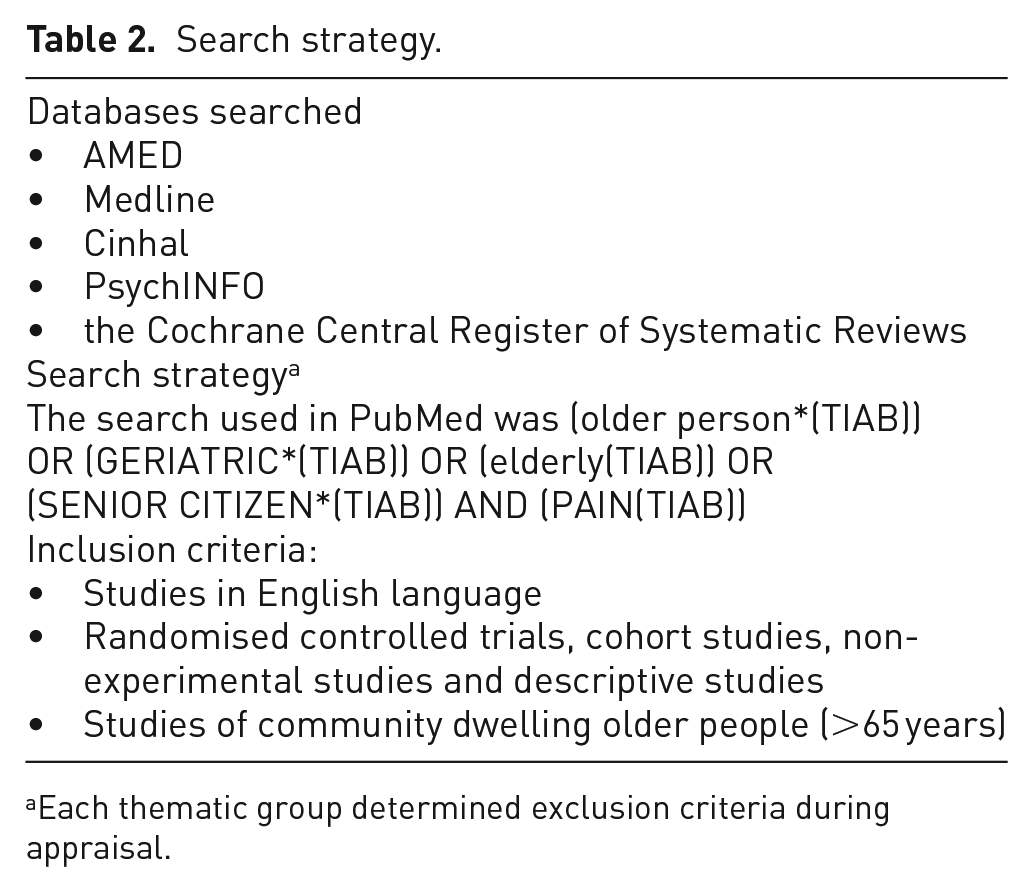
Each thematic group determined exclusion criteria during appraisal.
Results
Pain prevalence
The results were very similar to those found in the 2013 guidelines. 1 The 2013 report noted that the prevalence of pain was higher within residential care settings and we note similar findings suggesting very little has changed since. There is inconsistency in terms of age, diagnosis and terminology. Similar methodological challenges were also noted to those in the previous guidelines. A few new findings published since 2013 were identified within this review. Older people aged above 75 years, in the last 2 years of their lives and those in the last 4 months of life experienced increased pain. 4 Ageing and disability, including obesity and dementia, are associated with an increased prevalence of chronic pain.5–9
Summary
While there are a number of studies reporting the prevalence of chronic pain in this population, acknowledging that the phenomenon exists, under-treatment remains rife.
International guidelines
There remain few published current guidelines relating to pain in older people which are current. English language guidelines for pain management of older adults have been recently developed in the USA and Australia.10–13 A summary of the previous 2013 guidelines concluded that many interventions and pharmacological treatments require further research in older adult populations also that the evidence-base for non-pharmacological methods should also be advanced. 11
As mentioned in the previous guidance, in 2009, the American Geriatric Society (2009) updated their guidelines for the management of persistent pain in older adults and subsequent supplementary documents were published in 2011. 10 This update and supplementary documents discuss drug and non-pharmacological management, additional methods for assessing pain in the cognitively impaired and age-related physiological changes which should be considered when considering pharmacological treatment options. More recently in 2018, the Australian Pain Society updated their guidelines on the management of pain for older adults’ livings in residential settings. 13 This update includes sections on end-of-life pain management and nutrition, and it directed at all healthcare staff involved in the assessment and management of pain in older populations.
Other guidelines which are not age discriminative are available to offer recommendations for the management of specific conditions, for example, neuropathic pain, 14 end-of-life pain management15,16 and non-cancer chronic pain.17–19
Summary
The evidence-base to inform guidelines is still limited, resulting in recommendations informed by expert opinion, not high-quality evidence.
Attitudes and beliefs
Since the previous guidelines, research in the area has increased; this reveals a growing recognition of the significance of the older adults’ perspective in the assessment of pain and planning of pain management within this population.
Stoicism, or the belief that pain should be accepted or hidden from others, was a consistent theme within the previous report. Older adults continue to accept their chronic pain with stoicism and demonstrate fear-avoidance beliefs, which prevent them from help-seeking, leading to treatment avoidance and poor engagement with treatment recommendations.20,21
There is an intertwined relationship between pain beliefs and functional and psychological impairments caused by chronic pain. The fear-avoidance model of pain continues to be valid and relevant to the consideration of pain in older people.22,23 Beliefs can influence acceptance of pain control methods, certain pain beliefs exacerbate disability and cause escalation of chronicity.20,24–28
Recognition of the impact that attitudes and belief may have has led to the development of education and training programmes. Utilising education and training programmes, to implement the principles of CBT, can demonstrate sustainable gains in the reduction of maladaptive attitudes and beliefs.28–31 However, more work is needed to see how such programmes can be successfully integrated into healthcare care.
The previous review discussed the role of spousal beliefs and attitudes and how these can impact upon a significant other’s pain experience; no papers were found further exploring this issue. However, it is clear that healthcare providers must consider older adults own attitudes and beliefs, in addition to their psychological state, when addressing pain in this population.10,29,30
Summary
This section of the review and its recommendations echoes those made previously; however, there has been a significant increase in papers identified suggesting a growing recognition of the importance of the patient experience and perspective.
Impact on informal caregivers
The effect of caring for a person experiencing chronic pain was not explicitly considered previously. Informal carers frequently adopt supportive roles in pain management in terms of communication, being an advocate, assessing pain, managing side effects and finding solutions.32,33 Once patients are unable to self-report pain, carers can act as proxies in pain assessment which may be more accurate than health care professional assessment due to their personal knowledge of the care for person.34–36 However, assessing pain can be challenging for carers due to the complexities associated with the presence of co-existing symptoms and the impact of a high-carer burden associated with the demands of the caring role.32,36
Educational and family-centred interventions have had limited benefits in supporting carers in their pain management roles.37–39 However, a more integrated approach involving co-existing and evolving care between formal and informal health systems has been suggested. As such, formal and informal carers should combine their knowledge to manage the person more effectively.
Summary
The relationships between health care professionals and caregivers are clearly important as a means to improve pain management for older adults.
Palliative and end of life care
The previous report noted the absence of randomised controlled trials (RCTs) related to best practice in palliative care (non-cancer). Similarly, studies focused exclusively on people aged above 65 years related to palliative pain care management are scarce and the available evidence-base lacks high-quality RCT findings.40–44
Summary
No evidence relating to the palliative and end-of-life care pain management of co-morbid or other long-term conditions, such as chronic obstructive pulmonary disease (COPD), heart failure or dementia in older adults, were identified. Further evidence is required to inform good clinical practice and palliative care pain management for older adults with these conditions.
Pharmacological management
As with the previous version of guidelines, few studies investigating the effects of analgesic drugs specifically in older people were found. Physiological factors generally reflect the heterogeneity of the ageing population. 45
Paracetamol
The previous review advised paracetamol as a first-line pharmacological treatment, particularly for musculoskeletal pain. Despite continued recommendations for first-line use for paracetamol, there is little evidence for the benefit of short-term use.14,16,46,47 The majority of studies of the effects of paracetamol on chronic pain excluded people aged above 65 years, recent research suggests the limited benefit in chronic pain 48 and risk of adverse events for older people. 49
Paracetamol can be considered for short-term treatment but should be used with caution for long-term treatment for older patients with chronic pain. The efficacy of paracetamol in chronic pain is poor and there is emerging evidence that long-term use can be associated with significant adverse events.
Non-steroidal anti-inflammatory drugs (NSAIDs)
NSAIDs should be avoided for the management of chronic pain in older people due to numerous side effects, cautions and contraindications in older people; awareness of their possible harmful effects has increased and caution regarding their use has been expressed by different professional bodies. 50 A short course of NSAIDs can be considered on an individual basis, if the risk–benefit ratio is favourable, using the lowest effective dose for the shortest possible time.
Opioids
In the previous guidelines, evidence for long-term efficacy of opioids was limited and this remains unchanged. 51 However, in randomised clinical trials of short duration, opioids may be of some benefit. Regular review for efficacy and tolerability is essential. In older people, potential side effects including constipation, excessive sedation, delirium, falls and fractures are reported.
Recently, there has been greater caution in the recommendations and use of opioids for the management of chronic pain. 52 Although opioids continue to be beneficial in acute pain and at the end of life, there is limited evidence of benefit for many types of long-term pain such as osteoarthritis and low back pain.51,52 Where used, doses should be kept low and intermittent rather than regular. There are numerous opioids available and the choice will depend on pain intensity and co-morbidities for an individual person.
Adjuvant drugs
Adjuvant analgesic drugs have been recommended for the management of neuropathic pain in older people. 1 As in the previous guidelines, various types of antidepressants (including tricyclic antidepressants and selective serotonin norepinephrine reuptake inhibitors) or anti-epileptic medicines have possible benefits for people with neuropathic pain, but associated side effects may limit their use. Hence, caution is generally advised in older adults due to central nervous system side effects and as such these drugs should be introduced gradually and carefully monitored.
Topical therapies
The role of topical analgesics in the management of localised pain has been noted. Professional bodies have produced guidelines, on the use of topical NSAIDs, such as ketoprofen and diclofenac, as first-line choice in the treatment of osteoarthritis 53 and may be a safer alternative to oral NSAIDs in older adults. Topical capsaicin and lidocaine should only be considered as second-line treatments for neuropathic pain because of their limited efficacy in localised neuropathic pain.
Transdermal drugs can be very effective for pain treatment, however, in those aged above 85 years (the older) or frail patients with significant subcutaneous tissue loss, absorption can vary making it more difficult to predict efficacy. 54
Summary
The general pharmacological principles have not changed since the previous version of these guidelines. A large proportion of the results were informed by expert opinion, most of which were extrapolated from studies of adults aged 18–65 years.
Psychological and psychosocial interventions
A Cochrane review undertaken in 2011 55 considered the potential for psychological interventions for pain management in heterogeneous adult populations and noted that cognitive behavioural therapy (CBT) has a small effect in adult populations.
Summary
As reported in the previous guidelines, the evidence for behavioural interventions was limited. 1
Physical activity
In terms of physical activity, it is well documented that exercise is beneficial for the management of chronic pain. But as reported in the 2013 guidelines, there has still been limited research in terms of exercise specific to older adults. The quality of the evidence was considered to be low, mainly hampered by the small size of studies, and the findings were not conclusive. 56
Summary
From the limited evidence, we are able to conclude that exercise should be tailored to the needs of the individual regardless of age and should involve strengthening, endurance and flexibility exercises as an important role in self-management. But understanding motivation and barriers to exercise is an important factor and should be supported with education to aid understanding of the rationale behind the exercise.
Education
A systematic review of RCTs of educational intervention for adults with persistent pain concluded that the evidence-base for effects of education was of limited quantity and quality and that there was insufficient evidence of benefits of education on its own on pain or disability. 56
Summary
While awaiting specific evidence about adults aged above 65 years with persistent pain, it is sensible to recommend that education is offered alongside other pain management approaches to enhance its effect.
Interventions and invasive procedures
Summary
As per the 2013 guidelines, there remain limited studies relating to invasive procedures or interventions for pain in older people. Until further larger studies become available, no firm recommendations could be made.
Limitations
These updated guidelines have focused on the management of chronic pain in older people. Some of the recommendations, especially those related to pharmacology and interventions, may also be applicable to other types of pain.
Though the initial search and teams took a rigorous and systematic approach to the evidence-base, some studies from grey sources or non-English language publications may have been omitted.
Few studies make older people a discrete area of study and some recommendations are informed by the only available data, that is, a younger adult population. More robust and targeted research related to older people, in particular, is needed.
Good communication and assessment practices are fundamental to inform the assessment of pain and consequent management strategies. In producing these revised guidelines alongside the revised assessment of pain document, 57 we aim to promote and inform the practice of evidence-based pain management and good overall care.
Given the heterogeneity of the ageing UK population, an individualised and holistic approach to chronic pain management is advocated.
In conclusion, many of the recommendations from the previous guidelines largely still apply. While there have been more studies carried out exclusively in older people with chronic pain, these are still few in number and of variable quality. Hence, further good quality research is required in most areas related to the management of older people’s chronic pain.
Footnotes
Appendix 1
Search as applied in Medline with results on 30 May 2018.
Acknowledgements
The development of these guidelines was supported with funding from BUPA. The authors thank the British Pain Society, British Geriatrics Society and BUPA.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: A BUPA grant funded the main guideline development activity for this study.
Guarantor
M.D. is the guarantor of this study.