
Abstract
Aims:
Coronary computed tomography angiography is increasingly employed in the emergency department for suspected acute coronary syndrome patients. The HEART score has been proposed for initial risk stratification in these patients. The aim of this study was to investigate the diagnostic value and efficiency of the HEART score before coronary computed tomography angiography.
Methods and results:
We included patients suspected of acute coronary syndrome who underwent coronary computed tomography angiography in the emergency department. Based on the HEART score, patients were stratified as low-risk (HEART≤3), intermediate-risk (HEART4–6) and high-risk (HEART≥7). We assessed coronary computed tomography angiography for the presence of significant coronary artery disease (>50% stenosis). The primary outcome, the level of major adverse cardiac events, was a composite endpoint of all-cause mortality, acute coronary syndrome or coronary revascularisation within 30 days. The study population consisted of 340 patients (mean age: 55.6±10.1 years, 44.7% women), major adverse cardiac events occurred in 45 (13.2%) patients. The incidence of major adverse cardiac events in patients stratified as low-risk (35.0%), intermediate-risk (56.8%) and high-risk (8.2%) was 3.4%, 12.4% and 60.7%, respectively. All four low-risk patients with major adverse cardiac events had a HEART score of three. An algorithm where coronary computed tomography angiography is reserved for patients with HEART 3–6 resulted in a sensitivity of 97.8%, specificity of 84.1%, negative predictive value of 99.6% and positive predictive value of 48.4%, while reducing the need for coronary computed tomography angiography by 22% (n=75).
Conclusion:
The predictive value of coronary computed tomography angiography for 30-day major adverse cardiac events in suspected acute coronary syndrome patients is good, and reserving coronary computed tomography angiography for HEART score 3–6 patients reduces the number of needed coronary computed tomography angiograms without affecting diagnostic accuracy.
Keywords
Introduction
Patients with symptoms of a possible acute coronary syndrome (ACS) are frequently seen at the emergency department (ED).1–3 Physicians strive to achieve an effective but safe diagnostic work-up, as misdiagnoses can have serious consequences.2–4 The HEART score, a clinical tool for rapid risk stratification, has been proposed to improve decision making in patients suspected of ACS.5–8 Based on history, electrocardiogram (ECG), age, risk factors and initial troponin levels, the HEART score provides the physician with recommendations for further management. Recent studies suggest that the HEART score permits safe discharge of a considerable number of patients, effectively reducing downstream testing. 7 At the same time, several randomised trials have shown that coronary computed tomography angiography (CCTA) allows safe and early discharge from the ED providing valuable prognostic information as well.5,9,10 However, CCTA is a costly test and requires radiation exposure to the patient. Combining the HEART score with CCTA may provide a more efficient diagnostic work-up, where CCTA can be reserved for a subset of patients. The aim of this study was to investigate the diagnostic value and efficiency of the HEART score before CCTA in patients suspected of ACS in the ED.
Methods
Patient population
We conducted a secondary analysis of two prospective studies of patients presenting to the ED with symptoms suggestive of ACS. The methods, including study designs, inclusion and exclusion criteria have previously been published.9,11 In the current analysis, we included patients who underwent CCTA of diagnostic image quality. Both studies were performed according to the principles of the Declaration of Helsinki, approved by the local institutional review boards and all patients provided written informed consent.
CCTA
Image acquisition was performed on 64-slice or newer computed tomography systems, using ECG-synchronised axial or spiral scan protocols combined with radiation minimising measures, depending on local practices, available technology, and patient characteristics. Results of CCTA were reported by certified radiologists with a minimum of two years of experience reading CCTA. The presence of coronary plaque and the degree of stenosis was assessed for each evaluable coronary segment. The degree of stenosis was quantified as: no stenosis, ≤50% stenosis (non-obstructive plaque) or >50% stenosis (obstructive plaque).
HEART score
The HEART score, a clinical risk tool for rapid risk stratification of patients with acute chest pain, was calculated for each patient. The score consists of five components: History, ECG, Age, Risk factors and Troponin. Each of these components may be scored with 0, 1 or 2 points with a maximum score of 10 points. 8 Detailed information on the composition of the HEART score and how each component is scored can be found in Supplemental Material Table S1. Information regarding all components were retrieved from hospital records from the day of index presentation. As suggested by the original authors, patients were also categorised as: low risk (HEART ≤3), intermediate risk (HEART 4–6) and high risk (HEART ≥7). 8
Clinical endpoints
The primary outcome was occurrence of major adverse cardiac events (MACEs) within 30 days by analogy with prior publications on the HEART score;12,13 a composite of all-cause mortality, ACS or coronary revascularisation (emergent or elective within 30 days). ACS was defined as acute myocardial infarction or unstable angina according to the universal definition of acute myocardial infarction.14,15 All clinical endpoints were adjudicated by two cardiologists who independently reviewed medical records of patients. The result of the CCTA was blinded to the cardiologists performing the event adjudication.
Statistical analysis
Continuous data are presented as mean±standard deviation (SD) or median (interquartile ranges), and categorical data are presented as proportions (percentages). Differences between independent groups were compared using analysis of variance or the Kruskal-Wallis test for continuous variables, and the Fisher’s exact test or the Pearson’s chi-square test for categorical variables. Parameters of diagnostic accuracy, i.e. sensitivity, specificity, negative predictive value (NPV) and positive predictive value (PPV) for the prediction of 30-day MACEs were calculated with their corresponding 95% confidence intervals using exact binomial confidence intervals. When evaluating the CCTA, >50% stenosis was considered a positive test. Areas under the curve (AUCs) were calculated and compared using the test of DeLong et al. 16 All statistical analyses were performed using MedCalc Statistical Software version 18.10 (MedCalc Software bvba, Ostend, Belgium) and SPSS version 24.0 (IBM, Armonk, New York, USA). All tests were two-tailed and a p-value <0.05 was considered statistically significant.
Results
Baseline characteristics and clinical endpoints
Of 500 patients included in the Better Evaluation of Acute Chest Pain with Computed Tomography Angiography (BEACON) trial, 229 patients underwent CCTA and had diagnostic image quality. 9 Additionally, 111 patients in the Rotterdam Acute Chest Pain cohort underwent CCTA of diagnostic image quality. 11 In total, 340 patients met eligibility and were included for the current study (Figure 1). The mean age was 56±10 years and the proportion of women was 44.7%. MACEs occurred in 45 (13.2%) patients within 30 days (Table 1). The adjudicated diagnosis of ACS was established in 42 (12.4%) patients: 27 (7.9%) had myocardial infarction and 15 (4.4%) had unstable angina pectoris. Coronary revascularisation was performed in 38 (11.2%) patients. Seven patients with an adjudicated diagnosis of ACS did not undergo revascularisation within 30 days; Of these, two were managed medically and underwent revascularisation after 30 days and five were found to have no significant stenosis on invasive coronary angiography (ICA). Additionally, three patients underwent elective percutaneous coronary intervention (PCI) for stable angina pectoris. Cardiac troponins were available in all patients. Troponins were measured with high-sensitive troponin assays in 180 (53%) patients, of whom 177 patients with the high-sensitive Troponin T assay (Roche diagnostics). In the remaining 160 (47%) patients cardiac troponins were measured with conventional troponin assays. Supplemental Material Table S2 lists all troponin assays used, their characteristics and the algorithm in which they were implemented.
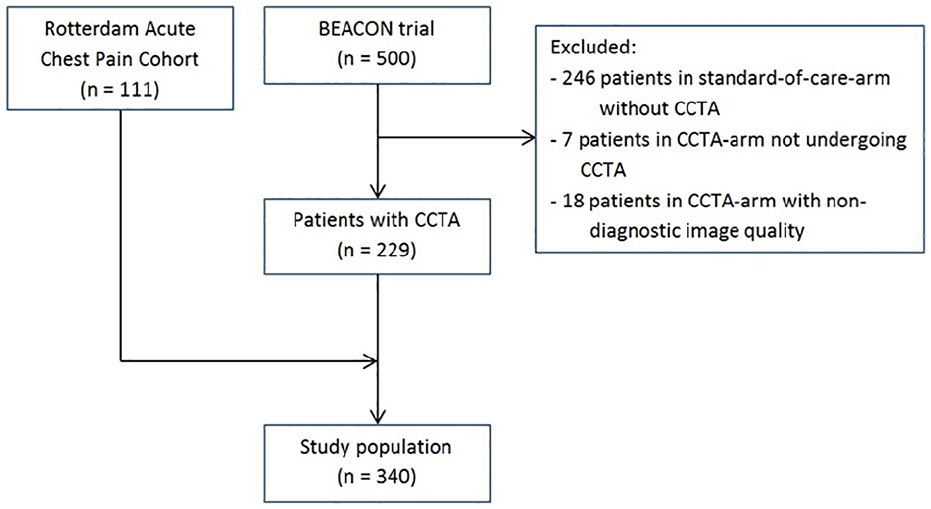
Flow diagram shows the enrolment process for the study population.
Baseline patient characteristics.
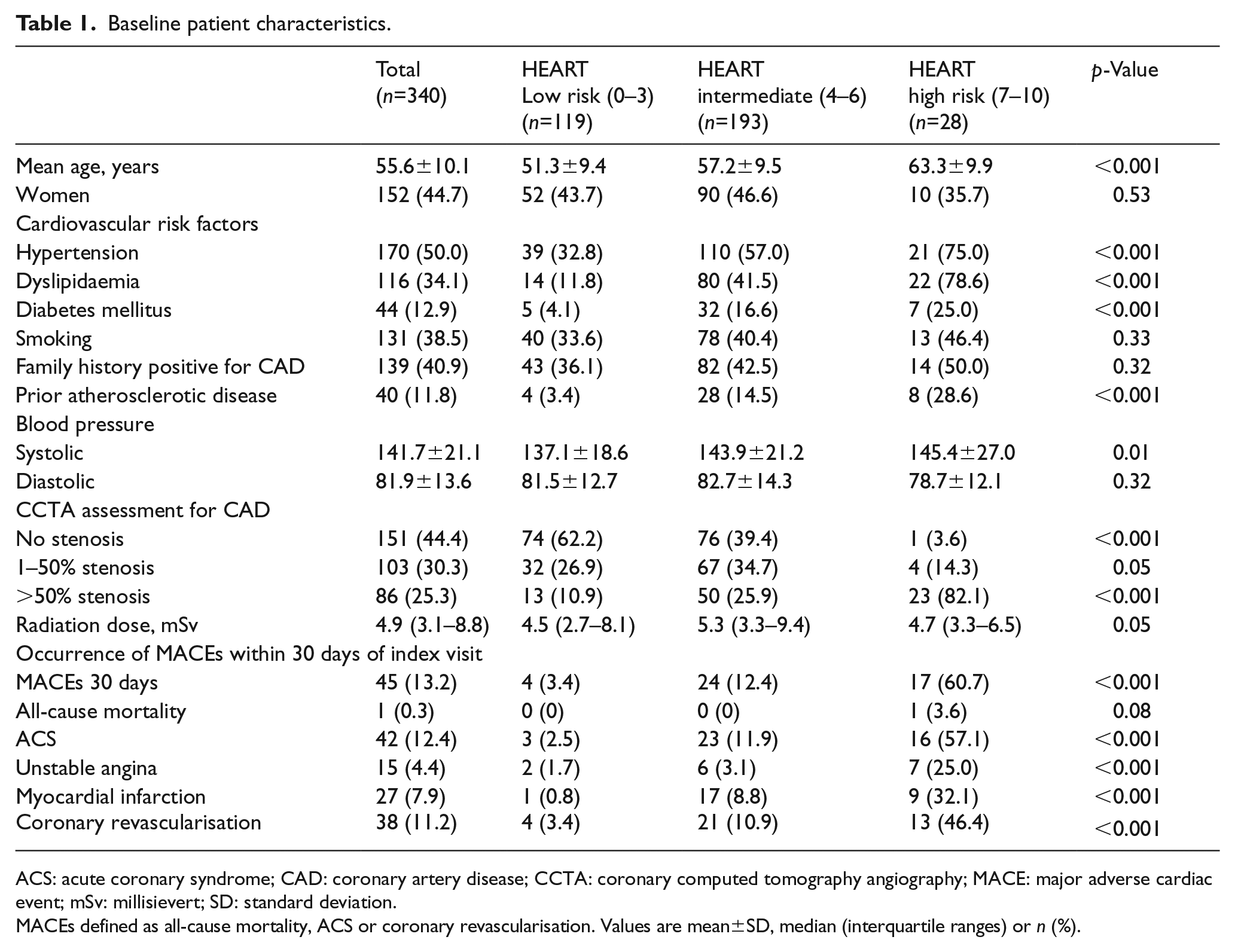
ACS: acute coronary syndrome; CAD: coronary artery disease; CCTA: coronary computed tomography angiography; MACE: major adverse cardiac event; mSv: millisievert; SD: standard deviation.
MACEs defined as all-cause mortality, ACS or coronary revascularisation. Values are mean±SD, median (interquartile ranges) or n (%).
CCTA
When assessed for coronary artery disease (CAD), 151 (44.4%) patients had no stenosis, 103 (30.3%) patients had 1–50% stenosis and 86 (25.3%) patients had >50% stenosis on CCTA (Table 1). The incidence of 30-day MACEs in patients with no stenosis, 1–50% stenosis and >50% stenosis was 0% (n=0), 1.9% (n=2) and 50% (n=43), respectively. Sensitivity, specificity, NPV and PPV of >50% stenosis on CCTA for the prediction of 30-day MACEs was 95.6% (84.9–99.5), 85.4% (80.9–89.2), 99.2% (97.0–99.8) and 50.0% (43.0–57.0), respectively. The AUC of >50% stenosis on CCTA for prediction of 30-day MACEs was 0.91 (0.87–0.93).
HEART score
The HEART score classified 119 (35.0%) patients as low-risk, 193 (56.8%) as intermediate-risk and 28 (8.2%) as high-risk. The incidence of 30-day MACEs in patients stratified as low-risk, intermediate-risk and high-risk was 3.4% (n=4), 12.4% (n=24), and 60.7% (n=17), respectively (Table 1). All patients (n=4) in the low-risk category with 30-day MACEs had a HEART score of three (Figure 2). Table 2 shows detailed characteristics of patients with a low HEART score (≤3) and MACEs within 30 days. All low-risk patients with 30-day MACEs had >50% stenosis on CCTA. Sensitivity, specificity, NPV and PPV of the HEART score for the prediction of 30-day MACEs at different cut-offs are shown in Table 3. The AUC of the HEART score for prediction of 30-day MACEs was 0.83 (0.78–0.87).
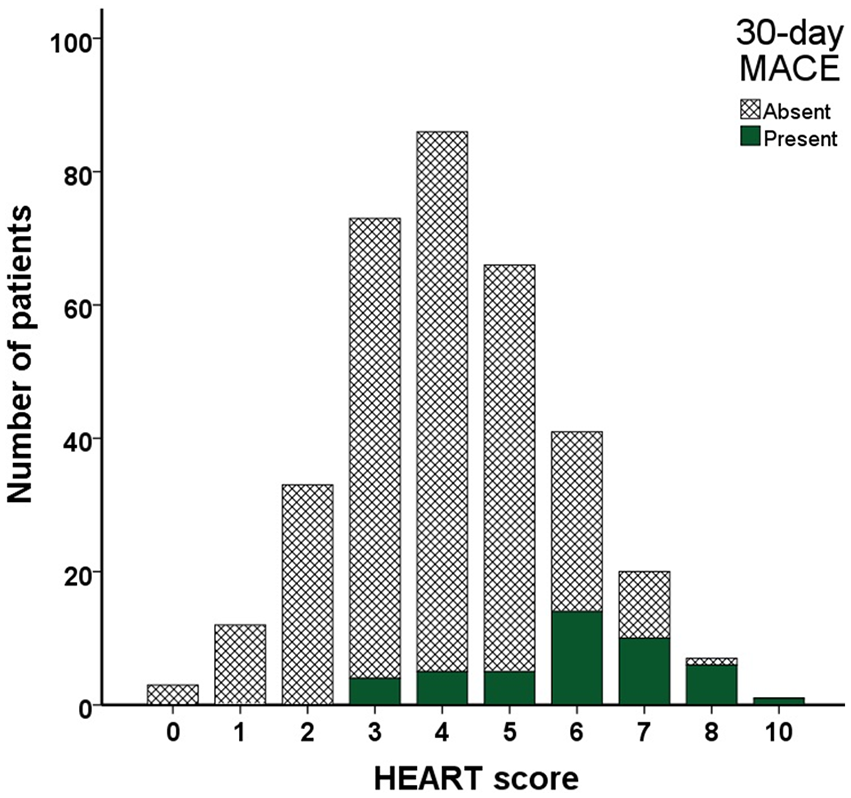
Frequency of 30-day major adverse cardiac events (MACEs) according to HEART score.
Detailed characteristics of patients with a low HEART score (≤3) or coronary computed tomography angiography (CCTA)≤50% stenosis and major adverse cardiac events (MACEs) within 30 days.
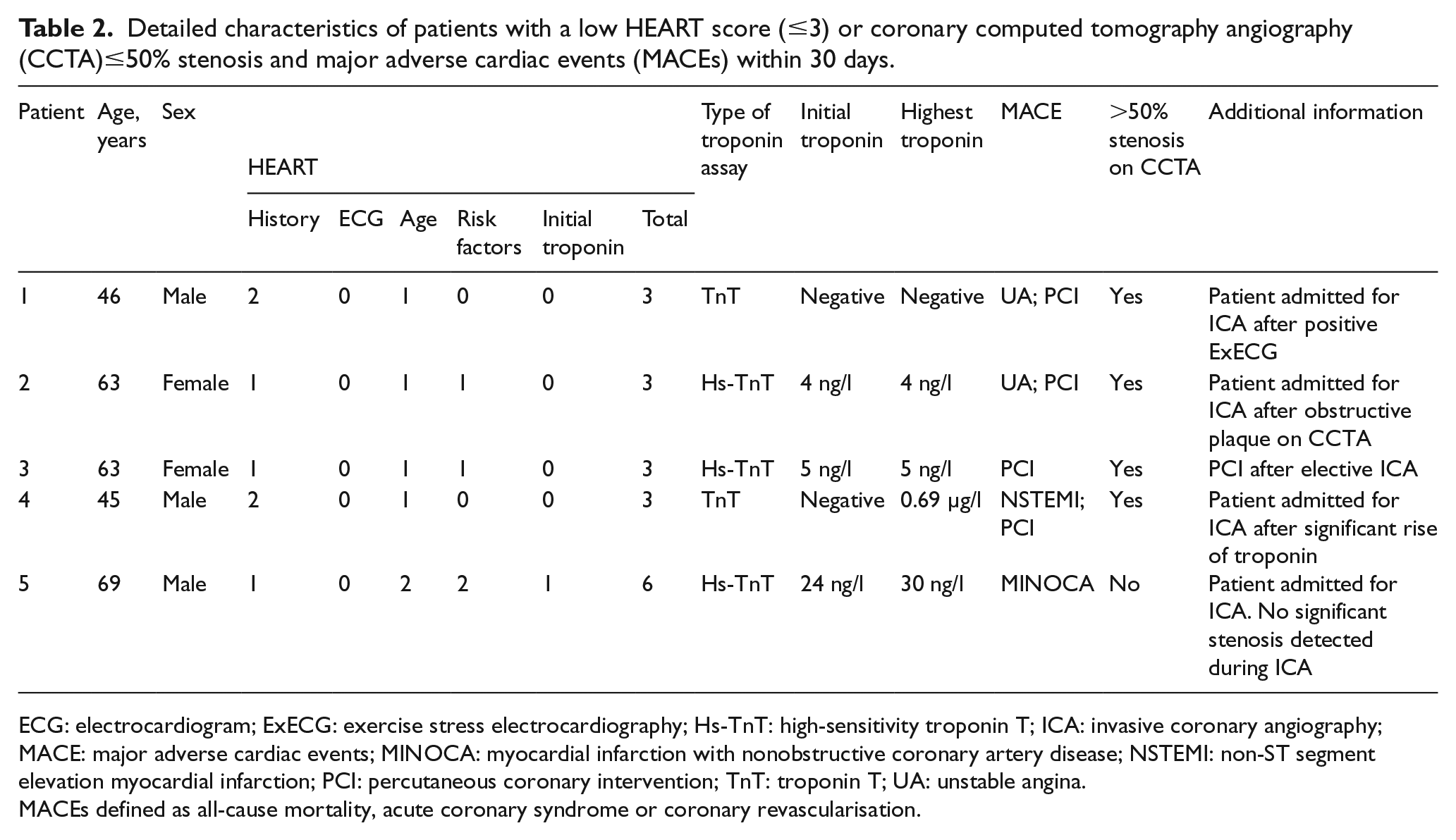
ECG: electrocardiogram; ExECG: exercise stress electrocardiography; Hs-TnT: high-sensitivity troponin T; ICA: invasive coronary angiography; MACE: major adverse cardiac events; MINOCA: myocardial infarction with nonobstructive coronary artery disease; NSTEMI: non-ST segment elevation myocardial infarction; PCI: percutaneous coronary intervention; TnT: troponin T; UA: unstable angina.
MACEs defined as all-cause mortality, acute coronary syndrome or coronary revascularisation.
Predictive value of the HEART score for 30-day major adverse cardiac events (MACEs) at various cut-offs.
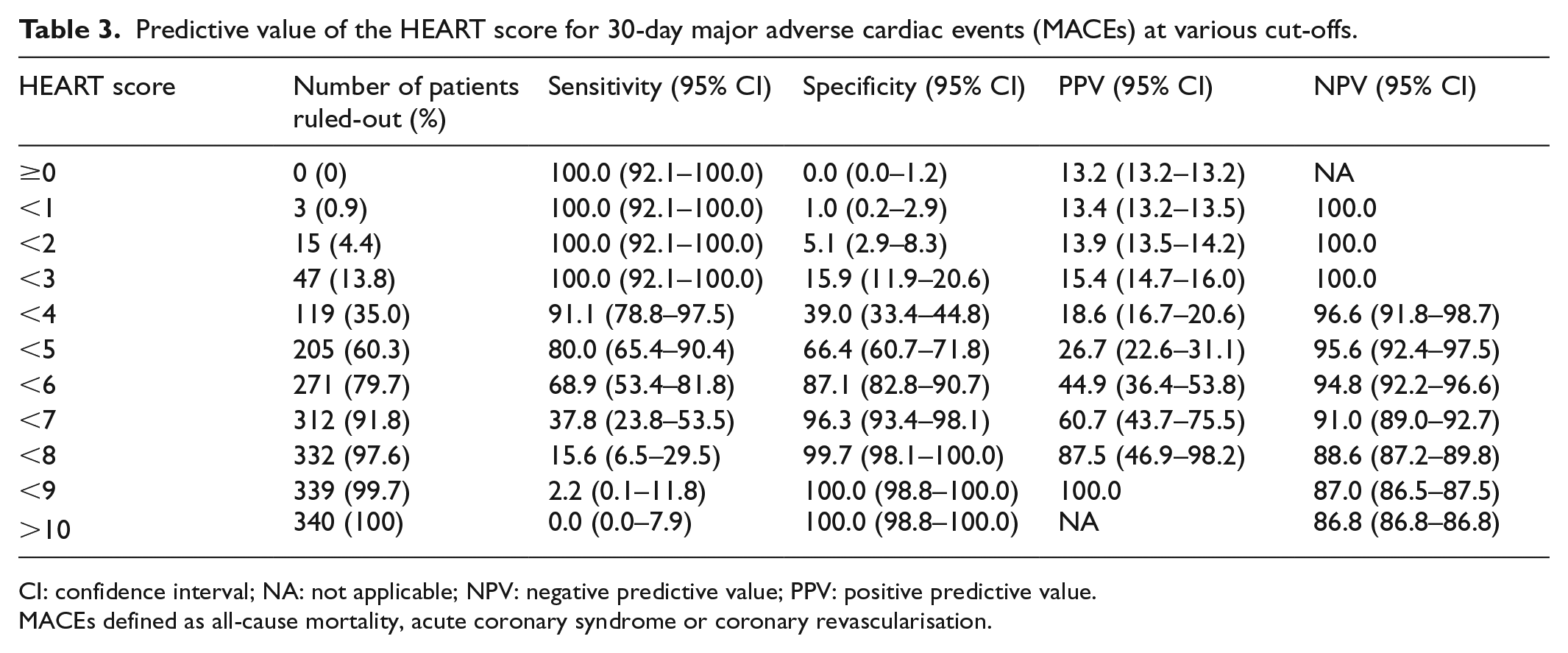
CI: confidence interval; NA: not applicable; NPV: negative predictive value; PPV: positive predictive value.
MACEs defined as all-cause mortality, acute coronary syndrome or coronary revascularisation.
HEART score and CCTA
The association between HEART risk categories and CCTA findings are shown in Table 1. In intermediate-risk patients, CCTA reclassified 143 (74.1%) patients to low-risk (<50% stenosis with a 30-day MACE rate 0.7%) and 50 (25.9%) patients to high-risk (>50% stenosis with a 30-day MACE rate 46%). One intermediate-risk patient (HEART score six) with non-obstructive plaque on CCTA had an adjudicated diagnosis of myocardial infarction, however this was considered a myocardial infarction with nonobstructive coronary arteries (MINOCA) with a minimal rise pattern in cardiac troponin and no significant stenosis on subsequent ICA (Table 2). The addition of CCTA to the HEART score was associated with a significant improvement of the diagnostic accuracy for 30-day MACEs (AUC 0.95 (0.92–0.97) vs 0.83 (0.78–0.87); p<0.001) (Figure 3). Sensitivity, specificity, NPV and PPV for the prediction of 30-day MACEs of an algorithm where CCTA is reserved for intermediate HEART scores (4–6) was 88.9% (76.0–96.3), 87.1% (82.8–90.7), 98.1% (95.7–99.2) and 51.3% (43.5–59.0), respectively. This algorithm reduces the need for CCTA by 43% (n=147). An algorithm where CCTA is reserved for HEART score 3–6 patients had a sensitivity, specificity, NPV and PPV for the prediction of 30-day MACEs of 97.8% (88.2–99.9), 84.1% (79.4–88.1), 99.6% (97.3–99.9) and 48.4% (41.8–55.0), respectively (Figure 4). This algorithm reduces the need for CCTA by 22% (n=75).
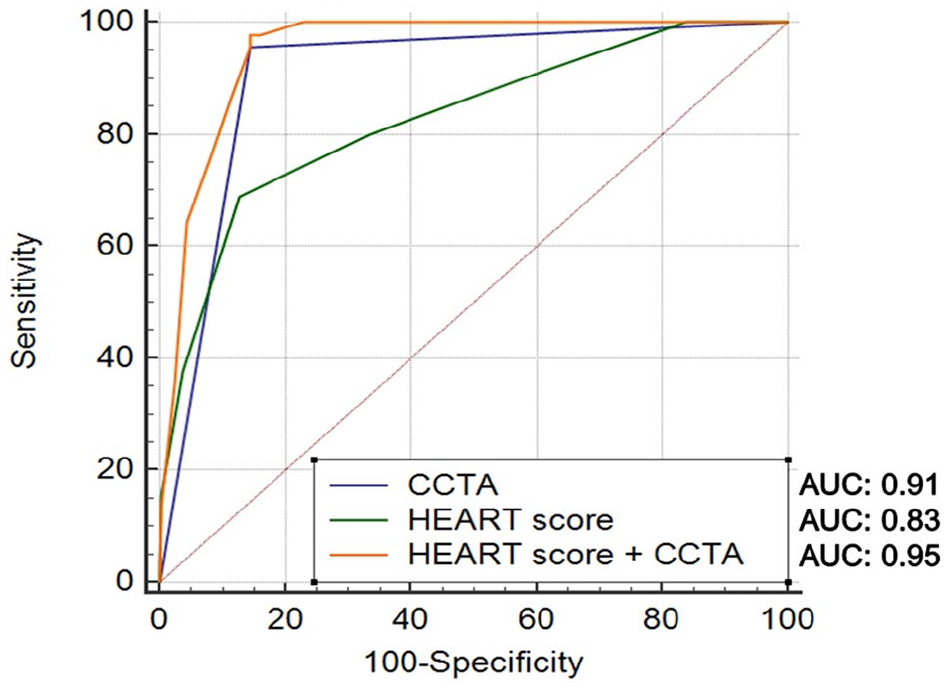
Predictive value of coronary computed tomography angiography (CCTA), HEART score and HEART score combined with CCTA for 30-day major adverse cardiac events (MACEs).
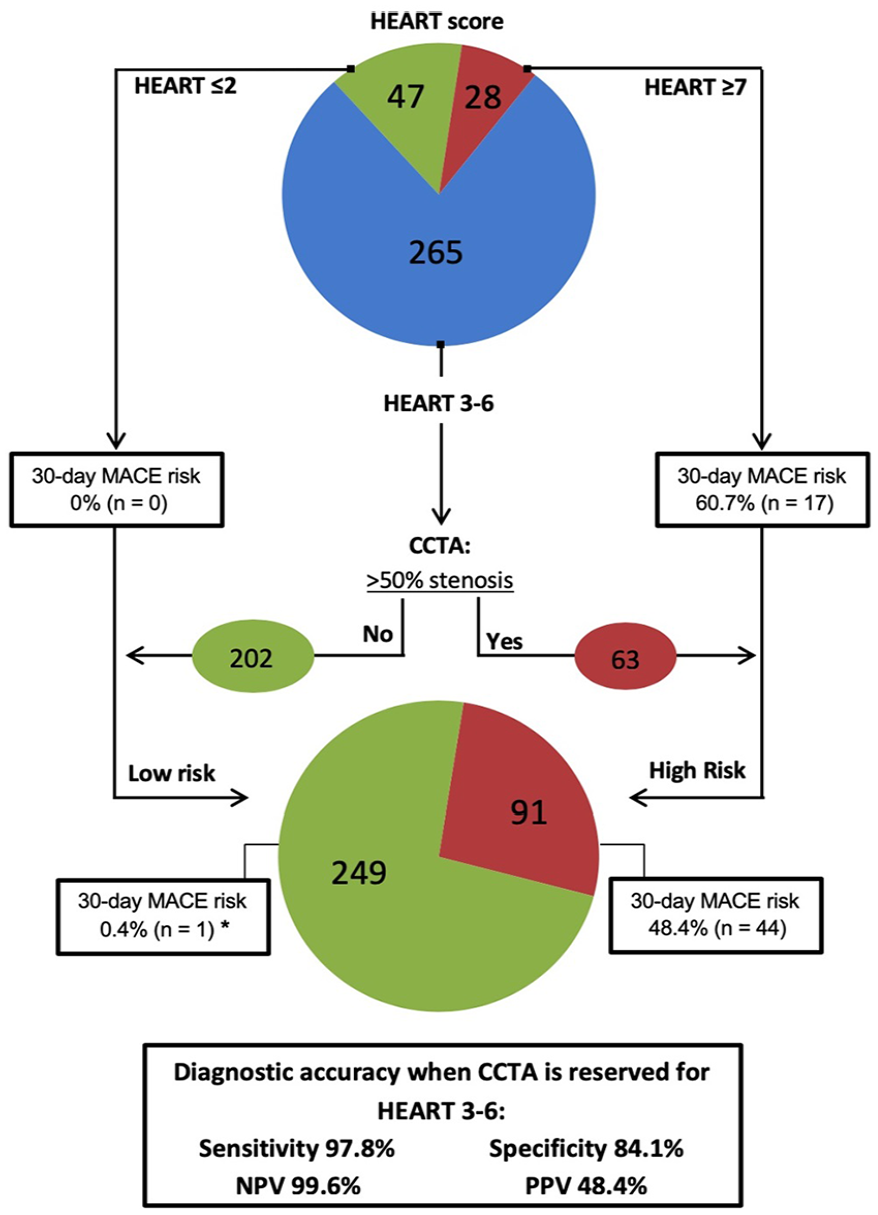
Predictive value of the HEART score combined with coronary computed tomography angiography (CCTA) assessment in HEART scores 3–6 for 30-day major adverse cardiac events (MACEs).
Discussion
In the current study, we investigated the predictive value and efficiency of the HEART score before CCTA for 30-day MACEs in suspected ACS patients in the ED and report several important findings. First, CCTA is a good predictor of 30-day MACEs in suspected ACS patients in the ED (AUC 0.91). Second, rule-out of 30-day MACEs based on the originally proposed low-risk HEART category (HEART score ≤3) is suboptimal (sensitivity 91.1% and NPV 96.6%). Third, addition of CCTA to the HEART score significantly improves the diagnostic accuracy for 30-day MACEs (AUC: 0.83 to 0.95; p<0.001). Finally, an algorithm where CCTA is reserved for patients with HEART score 3–6 reduces the need for CCTA by 22% (n=75) without compromising diagnostic accuracy or safety.
HEART score
In our study, the HEART score identified a large proportion (35%) of low-risk patients proposed for early discharge. However, the incidence of MACEs in low-risk patients was higher (3.4%) compared to previous reports, where the incidence ranged from 0.4–2.5%.8,12,13,17–19 Using the originally proposed score of ≤3 resulted in a generally unacceptable sensitivity and NPV in this population. 20 Notably, all four low-risk patients with 30-day MACEs had a score of three, of whom only one was diagnosed with non-ST segment elevation myocardial infarction (NSTEMI). Lowering the cut-off value for discharge to HEART scores ≤2 increased the diagnostic accuracy to acceptable levels in our study, something that has been proposed previously. 21 Further improvement of the diagnostic accuracy can probably be achieved by modifying the HEART score to incorporate serial troponin measurements.22–24
CCTA following HEART score
The addition of CCTA to the HEART score resulted in a substantial improvement in diagnostic accuracy, mainly by reclassifying intermediate-risk patients to their appropriate risk group. At the same time, using the HEART score to select patients that will benefit most from CCTA can result in a more efficient approach. Very low-risk HEART patients (score ≤2) did not experience 30-day MACEs in the current study and can be discharged safely from the ED, with further screening in an outpatient setting. High-risk HEART score patients, of whom 60.7% experienced 30-day MACEs in the current study, probably benefit most from an approach with early ICA. The algorithm HEART 3–6+CCTA reduced the number of needed coronary computed tomography angiograms while maintaining a high diagnostic accuracy and identifying a large proportion (73%) of patients who are eligible for safe and early discharge from the ED. In a similar fashion to the PRospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) minimal risk tool in suspected stable angina patients, which identifies individuals with low risk of CAD, the HEART score is able to reduce the need for non-invasive testing without comprising safety. 25
Limitations
The current study is a secondary analysis of patients suspected of ACS that underwent CCTA in the ED and should therefore be regarded as hypothesis generating. Our study population, which consisted mostly of low- to intermediate-risk patients, may not be representative of other populations of patients presenting with suspected ACS. The study population also consisted of patients in whom results of CCTA were used as part of their clinical work-up which in turn might have introduced a work-up bias. Furthermore, due to the heterogeneity of troponin assays implemented in current study, the results may be less applicable to individual troponin assays in clinical practice. In the current analysis, we were unable to investigate the diagnostic accuracy of the HEART pathway, an algorithm which incorporates serial troponin measurements into the HEART score, as serial troponin measurements were available in a minority of the patients. A disadvantage of CCTA is the exposure to radiation, however recent developments in scanner technology and dose-reducing protocols have led to a reduction in radiation exposure. 9 Furthermore, in the current analysis the HEART score helps reduce the number of coronary computed tomography angiograms performed, which also minimises the number of patients that are exposed to radiation.
Conclusion
The predictive value of CCTA for 30-day MACEs in suspected ACS patients is good and reserving CCTA for HEART score 3–6 patients reduces the number of needed coronary computed tomography angiograms without affecting diagnostic accuracy.
Supplemental Material
Supplemental_Material – Supplemental material for HEART score improves efficiency of coronary computed tomography angiography in patients suspected of acute coronary syndrome in the emergency department
Supplemental material, Supplemental_Material for HEART score improves efficiency of coronary computed tomography angiography in patients suspected of acute coronary syndrome in the emergency department by Murat Arslan, Jeroen Schaap, Pleunie PM Rood, Koen Nieman, Ricardo PJ Budde, Mohamed Attrach, Eric A Dubois and Admir Dedic in European Heart Journal: Acute Cardiovascular Care
Footnotes
Conflict of interest
KN reports unrestricted institutional research support from Siemens Healthineers, Bayer, GE and HeartFlow, outside the submitted work. All other authors declared no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Erasmus MC and a research grant from the Erasmus MC Thorax Foundation (project grant B4).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.