
Abstract
The occurrence of dyspnoea in acute coronary syndrome (ACS) patients has always been considered a challenging diagnostic and therapeutic clinical scenario. P2Y12 platelet receptor inhibitors (i.e., clopidogrel, prasugrel and ticagrelor) are currently the cornerstone of treatment of ACS patients. Thus, in the last few years, the potential association between ACS and dyspnoea has also become more challenging with the increasing use of ticagrelor in these patients due to its beneficial effects on ischaemic event prevention and mortality, since ticagrelor can induce dyspnoea as a side effect. The present article is intended to review the current literature regarding dyspnoea occurrence in ACS patients, especially those treated with ticagrelor, and to propose ticagrelor-associated dyspnoea management recommendations based on current knowledge.
Introduction
The occurrence of dyspnoea in acute coronary syndrome (ACS) patients has always been considered a challenging diagnostic and therapeutic clinical scenario. P2Y12 platelet receptor inhibitors (i.e., clopidogrel, prasugrel and ticagrelor) are currently the cornerstone of treatment of ACS patients. Thus, in the last few years, the potential association between ACS and dyspnoea has become also more challenging with the increasing use of ticagrelor in these patients,1,2 due to its beneficial effects on ischaemic event prevention and mortality, since ticagrelor can induce dyspnoea as a side effect. 3 The present article is intended to review the current literature regarding dyspnoea in ACS patients, especially those treated with ticagrelor, and to propose ticagrelor-associated dyspnoea management recommendations based on current knowledge.
Epidemiology of dyspnoea in acute coronary syndrome patients
Dyspnoea is one of the most common and distressing symptoms experienced by patients and can result from a variety of conditions, including cardiac, pulmonary, renal and liver diseases, anaemia and metabolic abnormalities. A substantial proportion (at least 25%) of patients with ACS may present with dyspnoea as the predominant symptom. 4 Moreover, ACS patients may develop dyspnoea during the index hospitalization or in the following weeks due to the development of heart failure, lung infection, adverse reaction to beta-blockers, recurrent ischaemia, anaemia or other potential complications. Patients with ACS who present with dyspnoea as their principal symptom are less likely to be recognized as having a coronary event, less likely to receive evidence-based treatments and more likely to experience poor outcomes. 5 In the Prospective Registry Evaluating Myocardial Infarction: Events and Recovery (PREMIER), 6 1835 unselected patients who survived an acute myocardial infarction had 1-month dyspnoea assessment using the Rose Dyspnoea Scale. In this study, 863 (47%) patients reported experiencing dyspnoea, with 340 (19%) noting moderate to severe limitation due to dyspnoea. Dyspnoea scores at 1 month were associated with an increased risk of rehospitalization and mortality at long-term follow-up. Moreover, although risk adjustment attenuated this association, even after adjustment for all relevant clinical and sociodemographic factors, the relationship between dyspnoea and impaired quality of life scores remained robust. In a real-world setting, 17% of patients with ST-elevation acute myocardial infarction present with heart failure symptoms at admission and, despite optimal reperfusion, further patients may develop heart failure during hospitalization. 7 The CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines) Investigators reported that about 25% of patients with non-ST segment elevation (NSTE) ACS in contemporary practice in the United States present with signs of congestive heart failure or develop in-hospital heart failure. 8 Finally, data from the PLATelet inhibition and patient Outcome (PLATO) study 3 reported that a significant proportion (more than 20%) of enrolled patients had dyspnoea prior to ACS onset, and those reporting dyspnoea prior to the index event were more likely also to experience dyspnoea after randomization. Dyspnoea during the study period was more likely to occur in the elderly, obese or smokers, and in patients with a history of congestive heart failure, asthma, chronic obstructive pulmonary disease or renal disease, and thus in subjects with dyspnoea prior to enrolment. Again, dyspnoea post randomization in clopidogrel-treated patients was associated with a poor outcome, including increased mortality, as expected with the presence of comorbidities.
Dyspnoea with ticagrelor
Dyspnoea is a very common ticagrelor side effect (see Table 1). In phase 2 studies, ticagrelor was associated with a dose-dependent incidence of dyspnoea of 10 to 20%, compared with 0–6.4% in patients treated with clopidogrel.9,10 Ticagrelor-related dyspnoea is generally described as sudden and unexpected air hunger or unsatisfied inspiration. Its pattern may vary widely, from very brief episodes lasting minutes, generally starting in the first week of treatment, to sustained or intermittent episodes occurring over several weeks, with most episodes being reported as mild. 3 In the ONSET/OFFSET study, 11 only 18% of dyspnoea episodes occurring in patients treated with ticagrelor were reported as moderate (no severe dyspnoea was reported). In this study, only three (14%) episodes of dyspnoea in ticagrelor-treated patients were persistent and only three patients required drug discontinuation due to dyspnoea. Generally, ticagrelor-related dyspnoea is not associated with wheezing, orthopnoea, paroxysmal nocturnal dyspnoea, or chest tightness or pain. Moreover, it usually occurs at rest, and is typically not related to exertion and does not limit exercise capacity. The exact mechanism of ticagrelor-related dyspnoea has not been definitively proven. Current hypotheses include stimulation of pulmonary vagal C fibres by increased levels of extracellular adenosine due to ticagrelor’s known antagonism of adenosine reuptake via equilibrative nucleoside transporter-1 (ENT-1)3,11 or the inhibition of P2Y12 receptors located on C fibres of sensory neurons. 12 The reversible nature of sensory neuron P2Y12 receptor inhibition could play a role, since cangrelor and elinogrel (other similar reversible agents) also increase dyspnoea occurrence. 12
Comparison of dyspnoea incidence in patients treated with ticagrelor and clopidogrel.
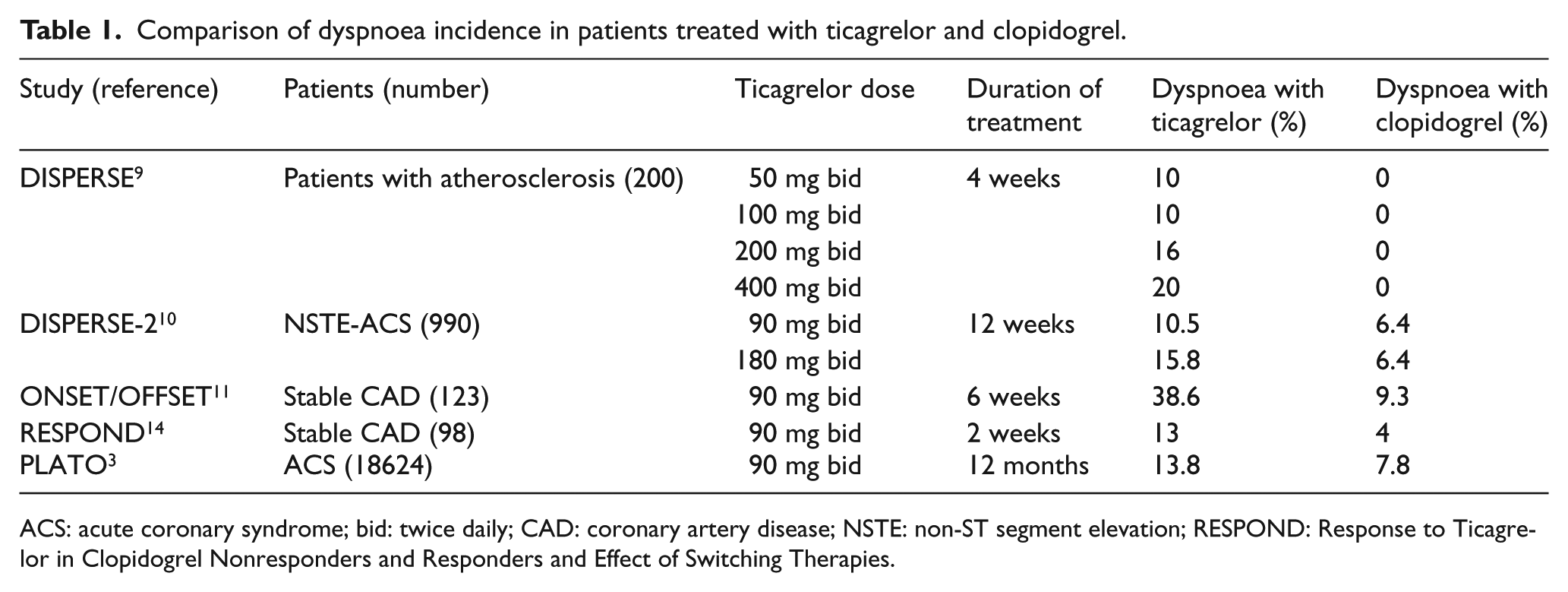
ACS: acute coronary syndrome; bid: twice daily; CAD: coronary artery disease; NSTE: non-ST segment elevation; RESPOND: Response to Ticagrelor in Clopidogrel Nonresponders and Responders and Effect of Switching Therapies.
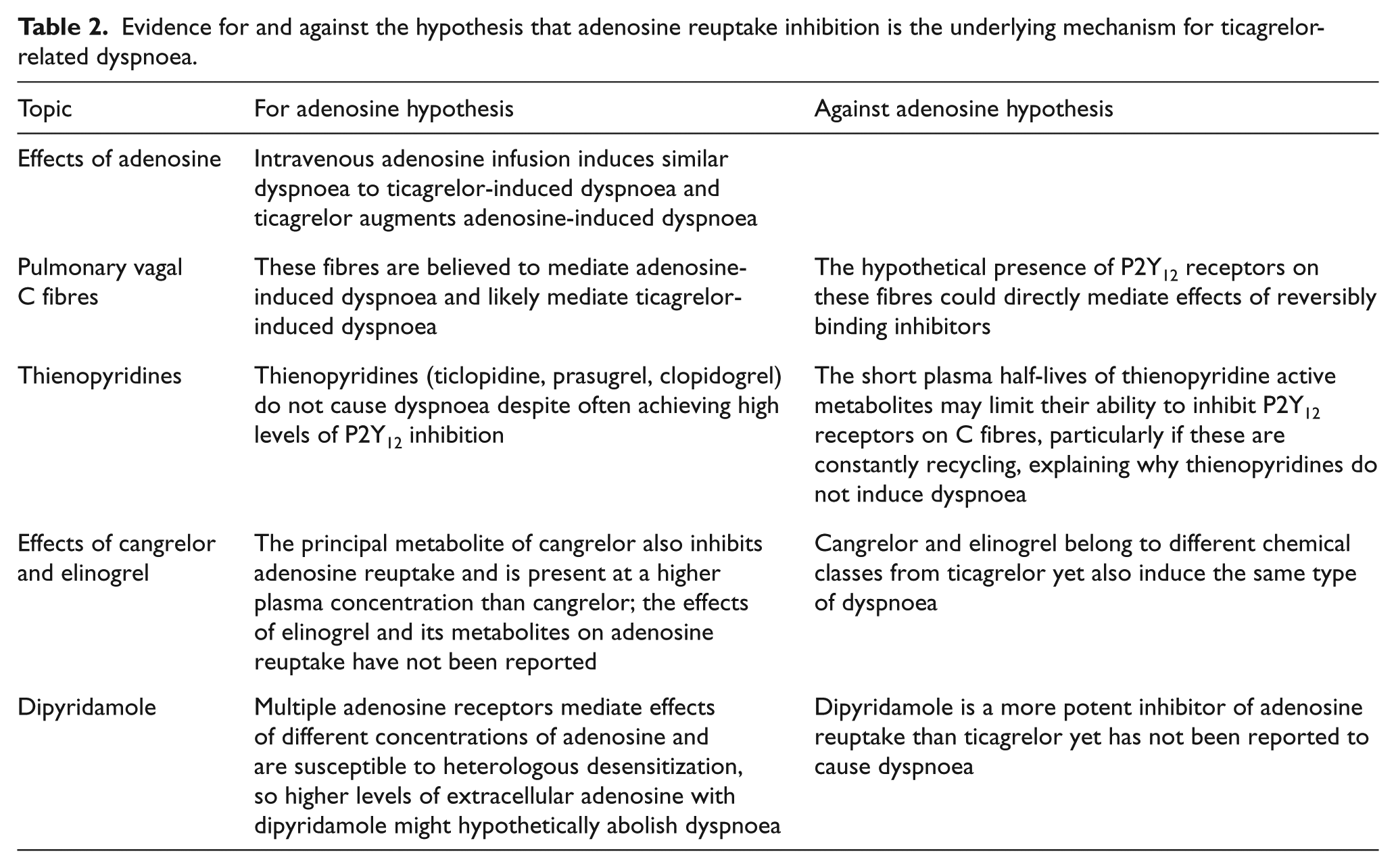
Current evidence for and against increased extracellular adenosine due to ENT-1 inhibition by ticagrelor as the underlying mechanism for ticagrelor-induced dyspnoea is presented in Table 2.
Evidence for and against the hypothesis that adenosine reuptake inhibition is the underlying mechanism for ticagrelor-related dyspnoea.
How to detect ticagrelor-related dyspnoea
It is important to note that, in the context of clinical practice where clinicians are not blinded to the prescribed medications, there may be a propensity to attribute dyspnoea to ticagrelor when in reality it is due to clinical factors, such as pulmonary congestion in a patient with new-onset heart failure after myocardial infarction. Moreover, anaemia, intercurrent pneumonia, worsening of pre-existing chronic pulmonary diseases, and metabolic abnormalities may also contribute to the development of dyspnoea. For proper management of patients, it is therefore crucial to consider all clinically plausible causes of dyspnoea before attributing it to the medication itself.
The evaluation of a patient with dyspnoea continues to be dependent on a thorough history and physical examination. For initial assessment of dyspnoea, it is pivotal to ask the patient whether the identical symptom was present before starting ticagrelor. If this is the case, the relationship between ticagrelor and dyspnoea becomes unlikely and alternative causes of dyspnoea should be considered and assessed. Then, it is very important to assess dyspnoea characteristics. Typical ticagrelor-related dyspnoea characteristics have been described in detail in the previous section. Frequently, the diagnosis of ticagrelor-related dyspnoea is based on exclusion. In addition to the patient’s interview, the exclusion of alternative dyspnoea causes may be performed by physical examination and other analyses and tests. The clinical examination, which can be easily performed during hospital stay and as an outpatient, is able to assess the likelihood of conditions such as heart failure or significant pulmonary disease associated with bronchospasm, emphysema and pneumonia. Simple blood sample examinations, especially during the initial phase of treatment occurring during hospitalization, are able to confirm heart failure (increased N-terminal of the prohormone brain natriuretic peptide (NT-pro-BNP)), anaemia (low red blood cell count) or respiratory failure (low oxygenation with or without hypercapnia). Despite the excess of dyspnoea in the ticagrelor group in PLATO, quality of life scores were no different between the ticagrelor and clopidogrel groups after adjustment for the improved life expectancy in the ticagrelor group. 13 It has been clearly documented that ticagrelor does not induce any adverse change in cardiac or pulmonary function that may cause dyspnoea either in patients with stable coronary artery disease or in patients with acute coronary syndromes.11,14 The assessment of left ventricular systolic and diastolic function, as well as valvular morphology and function, by transthoracic echocardiography provides further information and help in heart failure diagnosis of patients with ACS. Finally, chest X-ray and spirometry are useful tests to assess patients with dyspnoea and can be selectively used in difficult cases reporting dyspnoea after an ACS.
When to consider ticagrelor discontinuation
Ongoing studies have been designed to determine the main mechanism of ticagrelor-related dyspnoea. Other studies are also evaluating the possibility of pharmacologically treating this side effect in order to increase patient compliance: for example, using caffeine and other xanthine derivatives that oppose adenosine effects, hypothesizing a role of adenosine in the development of dyspnoea. However, until new data are available, currently the only way to manage persistent and intolerable ticagrelor-related dyspnoea is drug discontinuation.
In the case of an ACS patient treated with ticagrelor and reporting typical ticagrelor-related dyspnoea, after excluding alternative dyspnoea causes and pre-existing dyspnoea, we recommend taking some time to allow the possibility of spontaneous improvement in dyspnoea. In many cases, ticagrelor-related dyspnoea is transient and lasts a few hours or days, generally occurring within the first week of treatment. Thus, if the clinical conditions allow it, we can wait 3–4 days while observing the patient to understand whether the dyspnoea is transient or permanent. During this time period, alternative causes of dyspnoea can also emerge. In the case of permanent dyspnoea as a ticagrelor side effect, the following question should be considered: can the patient tolerate the dyspnoea, accepting the potential benefit in terms of reduced mortality risk? Ticagrelor-related dyspnoea is generally mild, sometime moderate and very occasionally severe. 3 In the majority of cases, patients tolerate the mild discomfort associated with the dyspnoea, and it is reasonable not to discontinue the drug, allowing the patient to continue to benefit from ticagrelor therapy and to have an optimal secondary prevention strategy. Only in the case of either persistent and intolerable ticagrelor-related dyspnoea or severe initial dyspnoea deemed likely to be provoked by ticagrelor should drug discontinuation be considered. Ticagrelor-related dyspnoea, if sustained during treatment, tends to resolve after the medication is discontinued, and there has been no evidence of any compromise to pulmonary or cardiac function that would lead to sustained dyspnoea after drug discontinuation. 11 In the case of drug discontinuation, if dyspnoea improvement occurs within a few days, compatible with ticagrelor clearance time, this clearly supports the diagnosis of ticagrelor-related dyspnoea. In Figure 1, we present a proposed algorithm for dyspnoea management in ACS patients treated with ticagrelor.
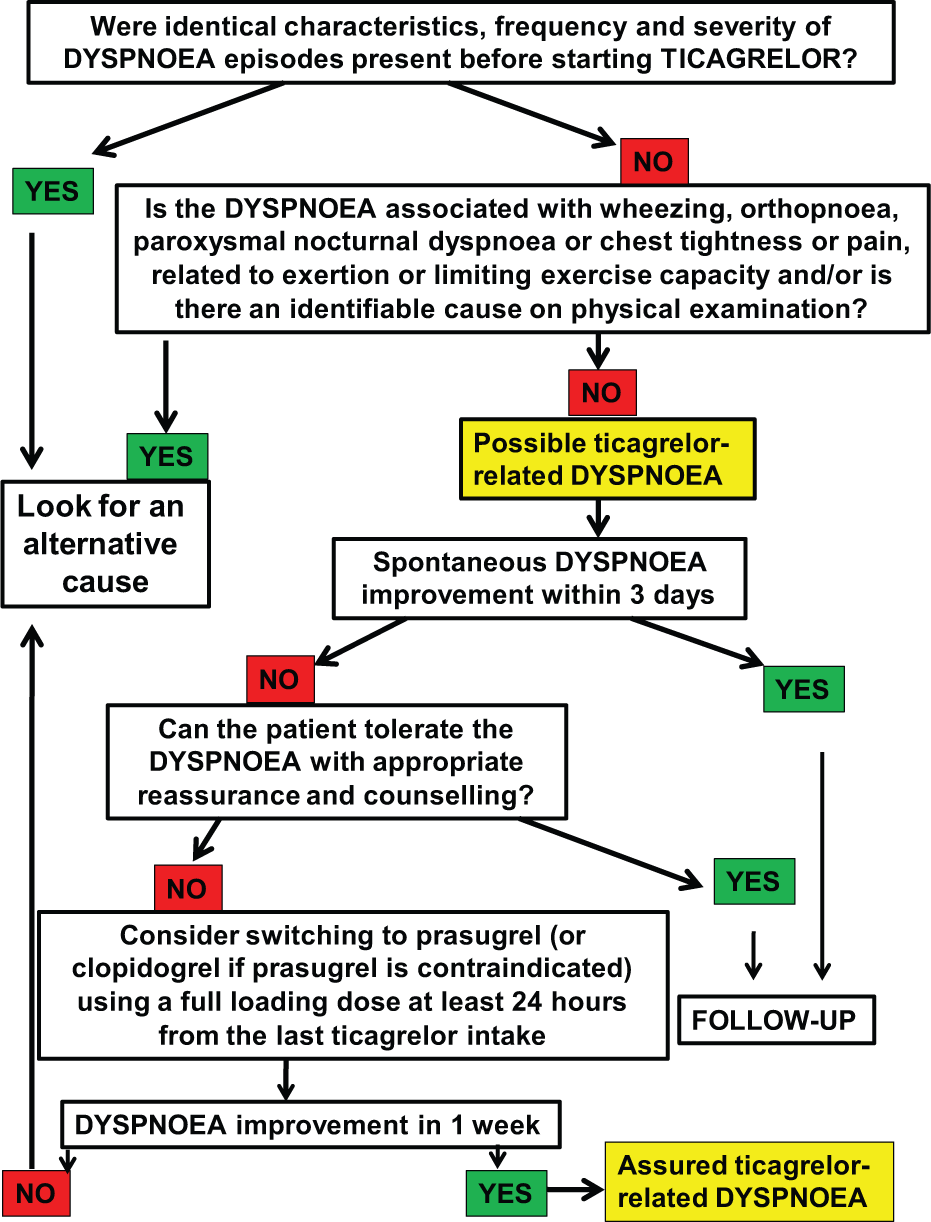
Dyspnoea diagnostic flow-chart.
Consequences of switching from ticagrelor to clopidogrel or prasugrel
The substantially lower mortality rates in ticagrelor-treated patients with dyspnoea compared with clopidogrel-treated patients with dyspnoea observed in the PLATO study 3 are consistent with three effects: first, the treatment benefit of ticagrelor compared with clopidogrel seen in the overall trial appears to be preserved in ticagrelor-treated patients with dyspnoea compared with those without dyspnoea; second, there is a favourable mortality prognosis in patients with ticagrelor-related dyspnoea compared with other causes of dyspnoea; and, third, high-risk patients such as those reporting dyspnoea need to be treated with the most effective pharmacological strategies. The fact that there was no evidence that the mortality benefit associated with ticagrelor in the PLATO trial was attenuated in the subgroup of patients with dyspnoea suggests that patients with tolerable dyspnoea should be encouraged to continue ticagrelor, while patients who cannot tolerate dyspnoea that is believed to be an adverse effect of the drug may be switched to either prasugrel or clopidogrel.
Switching patients with ticagrelor-related persistent and intolerable dyspnoea to clopidogrel may be an option. In the medical literature there are very few data regarding the strategy of switching ACS patients from ticagrelor to clopidogrel. Consequently, the clinical consequences of this procedure are poorly explored. Platelet function tests may be considered in selected patients at about 5 days after switching from ticagrelor to clopidogrel. Currently, the optimal length of a dual antiplatelet therapy after an ACS is unknown; however, in the PLATO study ticagrelor benefits over clopidogrel were evident in the first 30 days but clearly increased from 1 to 12 months, including in patients reporting dyspnoea. 3
We should keep in mind that, if a patient was initially selected for ticagrelor therapy due to a perceived high-risk profile, there are no meaningful reasons to downgrade the antiplatelet strategy to clopidogrel, except in the case of either a dangerous or an intolerable side effect or development of a contraindication to ticagrelor.
In the RESPOND study, 15 ticagrelor therapy was associated with greater platelet inhibition as compared with clopidogrel treatment in both ‘responders’ and ‘non-responders’ to clopidogrel, as defined by the pharmacodynamic response to a clopidogrel loading dose. Moreover, switching to clopidogrel therapy was associated with a reduction in drug-induced platelet inhibition. Finally, ticagrelor was extremely effective in reducing the prevalence of high residual platelet reactivity using previously defined cutoffs; nearly all patients during ticagrelor therapy, irrespective of clopidogrel response status, had platelet reactivity below the cutoffs associated with increased ischaemic risk. Thus, switching from a new and more potent antiplatelet agent such as ticagrelor (or prasugrel) to clopidogrel is ‘navigating in unknown waters’, 16 since it is currently unknown whether the subsequent increase in platelet reactivity soon after an acute coronary event might potentially lead to ischaemic events following recovery of platelet reactivity. As a matter of fact, switching patients perceived as being at high risk of bleeding from prasugrel to clopidogrel led to a 10-fold increase in average platelet aggregation, frankly unmasking poor responders to clopidogrel, 17 a subset of patients known to be at higher risk of thrombotic events, including coronary stent thrombosis. 18
Eventually, in the case of a non-haemorrhagic ticagrelor side-effect, such as dyspnoea, there is a greater rationale to switch many ACS patients to prasugrel as compared with downgrading to clopidogrel, assuming no contraindication to prasugrel. The Switching AntiPlatelet-2 (SWAP-2) trial was a pharmacodynamic study that addressed the issue of switching coronary artery disease patients from ticagrelor to prasugrel. 19 The study results suggested a pharmacodynamic interaction when switching from ticagrelor to prasugrel that is only partially mitigated when a prasugrel loading dose is used. In fact, during the early switching phase and up to 7 days of study treatment, prasugrel was associated with significantly higher platelet reactivity as compared with ticagrelor, consistent with observed differences in mean platelet reactivity between prasugrel and ticagrelor reported in other studies. The results of all switching pharmacodynamic studies should be confirmed by pharmacokinetic and, more importantly, by larger-scale clinical studies. However, a negative interaction between ticagrelor and either clopidogrel or prasugrel is highly probable: it is possible that occupancy of P2Y12 receptors by ticagrelor might prevent the active metabolites of clopidogrel or prasugrel from binding to the receptor during the early switching phase, as has been demonstrated for the reversibly binding P2Y12 inhibitor cangrelor. 20 Hypothetically, the prasugrel active metabolite may not be able to bind to the receptor until ticagrelor has dissociated. Ticagrelor might also induce a change in receptor conformation that temporarily precludes the clopidogrel or prasugrel active metabolite from binding. Given the SWAP-2 study results, it seems reasonable to start prasugrel at least 24 h after the last ticagrelor intake using a prasugrel loading dose. However, more data are needed to determine the optimal strategy and timing of switching to clopidogrel or prasugrel in the uncommon case in which ticagrelor should be discontinued due to a relevant, permanent and intolerable side effect.
Conclusions
Some facts should be considered in our clinical practice:
In a patient with new onset of dyspnoea, the history and physical examination remain the mainstays of diagnostic evaluation.
Assessing cause of dyspnoea may be difficult in ACS patients treated with ticagrelor.
Dyspnoea is a very common ticagrelor side effect (>10%), but a genuine need for drug discontinuation is rare.
ACS patients reporting dyspnoea have a high-risk profile and should be managed with the most effective treatment strategies.
Balancing side effects and therapeutic advantages of each single drug is needed.
Only in the case of persistent and intolerable ticagrelor-related dyspnoea should drug discontinuation be considered.
Footnotes
Conflict of interest
Guido Parodi reported receiving consulting or lecture fees from AstraZeneca, Bayer, Daiichi Sankyo/Eli Lilly and The Medicines Company. Robert F. Storey reported receiving consulting fees or honoraria from AstraZeneca, Accumetrics, Daiichi Sankyo, Eli Lilly, Medscape, Merck, Novartis, PlaqueTec, Roche, Regeneron, Sanofi Aventis and The Medicines Company, and institutional grants or support from AstraZeneca, Accumetrics, Daiichi Sankyo, Eli Lilly and Merck.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.