
Abstract
Background
Lipoprotein(a) (Lp(a)) is an established casual risk factor for atherosclerotic cardiovascular disease. It remains unknown whether dietary fat modifies the association of Lp(a) with cardiovascular death.
Aim
To understand if dietary fat modifies the association between Lp(a) and cardiovascular death.
Methods
We utilized the Atherosclerotic Risk in Communities (ARIC) study and National Health and Nutrition Examination Survey (NHANES) III cohorts and used multivariate cox proportional hazard modeling to test the association between Lp(a), dietary fats, and cardiovascular death.
Results
The sample (n = 22,805) had average age 51.3 years and was mostly female (55.4%). Lp(a) ≥ 30 mg/dL was associated with CV death in both ARIC (1.36, p = 0.001) and NHANES (1.31, p = 0.03). In multivariate analysis, no categorical or individual fatty acids modified the association between Lp(a) and CV death.
Conclusion
There was no evidence that baseline dietary fat intake modified the association between Lp(a) and CV death.
Introduction
Lipoprotein(a) (Lp(a)) is an established risk factor for atherosclerotic cardiovascular disease (ASCVD).1,2 Increased Lp(a) levels are associated with increased cardiac and all-cause mortality.3,4 As at least 1-in-7 US adults has an elevated Lp(a) level, the potential population with increased risk for Lp(a)-associated cardiovascular (CV) disease is large. 5
Dietary intake is a major driver for developing ASCVD. 6 However, dietary intake, including fats, have only a small direct impact on Lp(a) levels (typically a few mg/dL change at most).7–10 Despite there being only a small impact of diet on Lp(a) levels, dietary approaches may help to mitigate the risk associated with Lp(a). In two large cohort studies it was found that those following healthier lifestyle patterns had much lower risk for ASCVD despite higher Lp(a) levels. In EPIC-Norfolk (n = 14,051), those with the top compared to bottom tertile of Life's Simple 7 score and Lp(a) ≥ 50 mg/dL had a HR of 0.33. 11 In the ATTICA study (n = 3052), those that had high adherence to a Mediterranean diet score had no additional risk associated with Lp(a). 12 It is unknown what drove these findings from a macronutrient standpoint, including whether types of dietary fat intake might explain the relationship between healthier lifestyle and reduced risk for cardiac death despite elevated Lp(a).
We utilized two large cohorts from the United States to investigate whether an association exists between Lp(a) and dietary fats with CV death, as well as whether dietary fat intake modifies the association between Lp(a) and CV death.
Methods
Data
We utilized the Atherosclerotic Risk in Communities (ARIC) study and National Health and Nutrition Examination Survey (NHANES) III databases. ARIC was a prospective, longitudinal investigation into the cardiac risk factors, health outcomes, and demographic patterning of atherosclerosis across four United States communities. ARIC enrolled men and women aged 35–84 years, beginning in 1987 from four US communities. NHANES III was conducted by the Center for Disease Control and Prevention and is a representative cross-sectional cohort of the US population collected between 1988 and 1994 from a multi-stage probability sample of about 40,000 non-institutionalized civilians.
We studied adults (aged ≥18 years) and used demographic, laboratory, medical history, and fatty acid intake. Fatty acid intake was derived from dietary recall. In ARIC this was a food-frequency questionnaire, which was based on daily intake of nutrients from 66 foods. 13 In NHANES this was 24-h dietary recall that are then reported based on the University of Minnesota Nutrition Coordinating Center nutrient database, which has information on over 80 nutrients and food components. 14 The study was exempt by the University of Michigan institutional review board (HUM00203926).
Statistical analysis
The primary outcome measure was CV death based on ICD-9/ICD-10 codes (390–398, 402, 404–429 and I00-I09, I11, I13, I20-I51, respectively). The main covariates of interest were Lp(a) and dietary fats. Dietary fats were explored as categories, and individual fatty acids by carbon chain length as continuous variables. Multivariate cox proportional hazard modeling was done to determine baseline dietary fat intake and Lp(a)'s association with CV death. Multivariate models accounted for factors known to impact risk for CV mortality, covariates included age, gender, race and ethnicity, history of smoking or tobacco (ever smoked at least 100 cigarettes or 20 pipes or cigars in life or current chewing tobacco or snuff), HDL-cholesterol, non-HDL-cholesterol, and history of hypertension diabetes, obesity (body mass index ≥30 kg/m2), myocardial infarction, and stroke. Non-HDL-C was calculated by subtracting HDL-C from Total Cholesterol and corrected for Lp(a) mass (non-HDL-C=Total Cholesterol–HDL-C–(Lp(a)x0.3)). We tested whether dietary fat intake modified the association between Lp(a) and CV death by applying an interaction term between these two covariates. ARIC and NHANES were analyzed individually. All p-values were two-sided. Analyses were adjusted for total caloric intake (as reported based on estimated from aforementioned nutrition data). Statistical significance was set at p < 0.05. Data were analyzed using Stata software, version 16 (StataCorp, LLC).
Results
Sample characteristics
The sample consisted of 22,805 individuals (average age 51.3 years) and was mostly female (55.4%). Lp(a) was ≥30 mg/dL in 16.4%. Complete demographic and medical comorbidity data are presented in Table 1. ARIC and NHANES contained up to 31.1 years and 29.3 years of patient follow-up respectively.
Demographic and medical comorbidity data of cohorts.
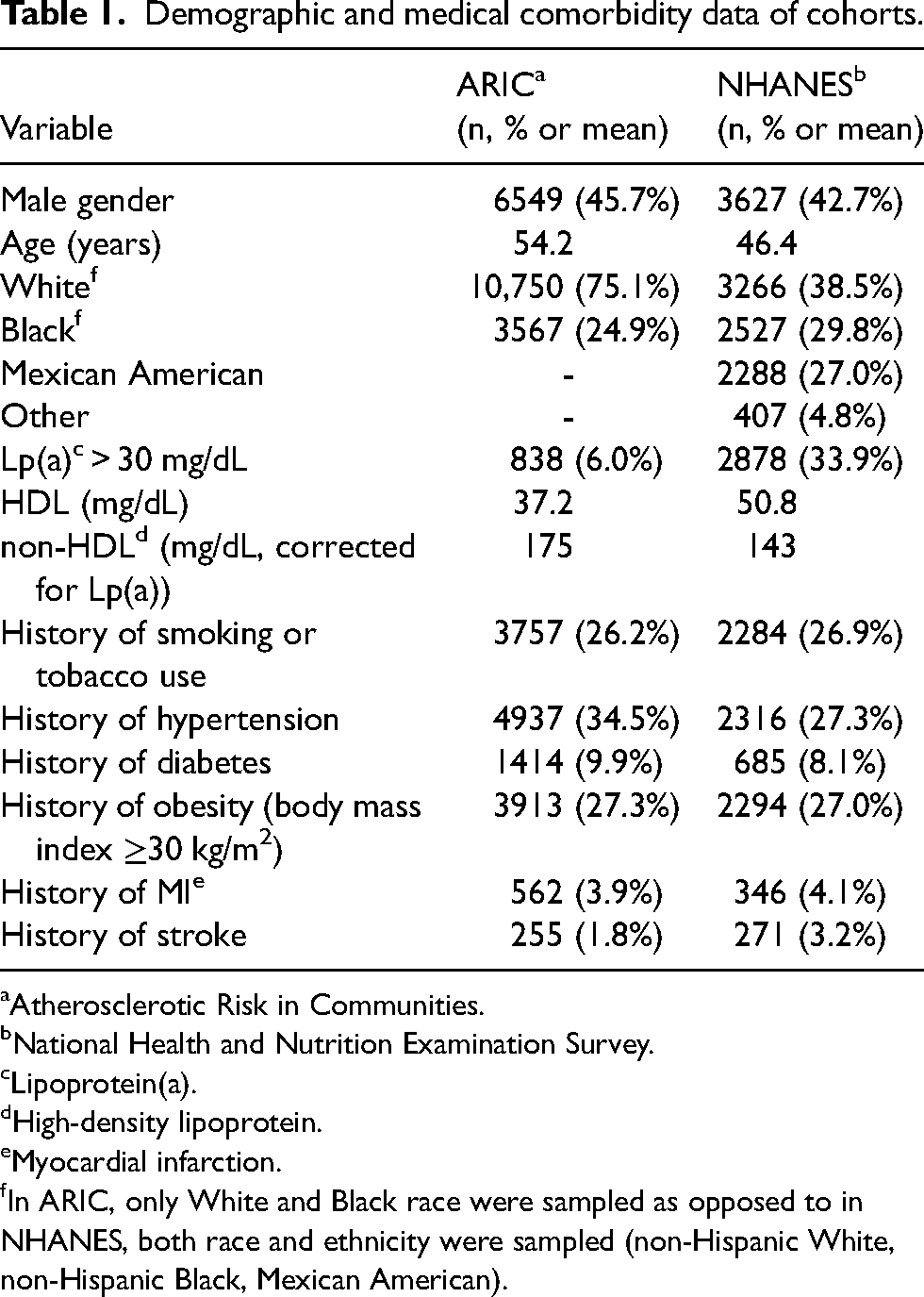
Atherosclerotic Risk in Communities.
National Health and Nutrition Examination Survey.
Lipoprotein(a).
High-density lipoprotein.
Myocardial infarction.
In ARIC, only White and Black race were sampled as opposed to in NHANES, both race and ethnicity were sampled (non-Hispanic White, non-Hispanic Black, Mexican American).
Association of covariates with CV death
Several covariates had associations with CV death in both datasets (Table 2). Factors associated with CV death in both datasets (hazard ratio (95% CI), p-value) were age (ARIC: 1.11 (1.10–1.12),<0.001, NHANES: 1.09 (1.09–1.09),<0.001), female gender (ARIC: 0.64 (0.57–0.72),<0.001, NHANES: 0.65 (0.55–0.76),<0.001), smoking history (ARIC: 2.16 (1.94–2.41),<0.001, NHANES: 1.37 (1.17–1.61),<0.001), history of hypertension (ARIC: 1.68 (1.51–1.87),<0.001, NHANES: 1.35 (1.17–1.56,<0.001), history of diabetes (ARIC: 2.37 (2.08–2.69),<0.001, NHANES: 2.00 (1.67–2.40),<0.001), history of MI (ARIC: 3.54 (3.04–4.13),<0.001, NHANES: 2.20 (1.82–2.67)<0.001), and history of stroke (ARIC: 2.16 (1.70–2.74),<0.001, NHANES: 1.69 (1.33–2.14),<0.001). There were some covariates that associated differently in the datasets. Total caloric intake (per 100 calories) associated with CV death in the ARIC (1.012 (1.005–1.021), 0.002), but not in NHANES (0.993 (0.984–1.002, 0.13). The same were also true for HDL (ARIC: 0.99, (0.98–0.99),<0.001, NHANES: 0.999, (0.994–1.004), 0.73), non-HDL (corrected for Lp(a)) (ARIC: 1.003, (1.002–1.004),<0.00, NHANES: 1.001, (0.999–1.004), 0.36), and obesity (ARIC: 1.40, (1.25–1.56),<0.001, NHANES: 1.11 (0.96–1.30), 0.16). A detailed overview of covariate associations with CV death is presented in Table 2.
Association between covariates and cardiovascular death in multivariable Cox proportional hazard analysis.

Bold type = p<0.05.
Atherosclerotic Risk in Communities.
National Health and Nutrition Examination Survey.
High-density lipoprotein.
Lipoprotein(a).
Myocardial infarction.
In ARIC, only White and Black race were sampled as opposed to in NHANES, both race and ethnicity were sampled (non-Hispanic White, non-Hispanic Black, Mexican American).
Association of Lp(a) and dietary fats with CV death
Lp(a) ≥ 30 mg/dL was associated with CV death in both ARIC (1.36 (1.13–1.64), p = 0.001) and NHANES (1.31(1.13–1.51), p = 0.03). While total fat (1.004 per gram (1.003–1.008), p = 0.03) and saturated fat (1.01 (1.005–1.022), p = 0.002) intake were associated with CV death in ARIC, this was not seen in NHANES (Table 3). There were numerous associations of individual fatty acids with CV death in ARIC but none in NHANES. In ARIC this included positive associations to CV death with medium- to long-chain saturated fatty acids (capric acid (C10:0, 1.32 (1.02–1.74), p = 0.04), lauric acid (C12:0, 1.35 (1.06–1.73), p = 0.02), myristic acid (C14:0, 1.08 (1.02–1.15), p = 0.01), palmitic acid (C16:0, 1.02 (1.01–1.04), p = 0.01), and stearic acid (C18:0, 1.05 (1.02–1.09), p < 0.001)) and the monounsaturated fat palmitoleic acid (C16:1, 1.13 (1.02–1.27), p = .03). There were negative associations in ARIC with the monounsaturated fat eicosenoic acid (C20:1, 0.62 (0.42–0.90), p = 0.01) and the polyunsaturated fats eicosapentaenoic acid (C20:5, 0.53 (0.30–0.92), p = 0.02) and docosahexaenoic acid (C22:6, 0.70 (0.52–0.96), p = 0.03). In the entire sample, stearic acid (C18:0, 1.03 (1.01–1.05), p = 0.01) was positively associated with CV death, whereas eicosenoic (C20:1, 0.64 (0.48–0.86), p = 0.003) and docosahexaenoic acid (C22:6; 0.75 (0.60–0.93), p = 0.01) were negatively associated.
Associations between dietary fat intake (per gram/day) and lipoprotein(a) with cardiovascular death in multivariable Cox proportional hazard analysis.

Bold type = p<0.05.
Atherosclerotic Risk in Communities.
National Health and Nutrition Examination Survey.
Liporotein(a).
Interaction of Lp(a) with dietary fats on association with CV death
In multivariate analysis, no categorical or individual fatty acids modified the association between Lp(a) and CV death in any of the individual ARIC or NHANES datasets (Table 4).
Association of interactions between dietary fat intake (per gram/day) and lipoprotein(a) with cardiovascular death.

Atherosclerotic Risk in Communities.
National Health and Nutrition Examination Survey.
Discussion
In both cohorts, Lp(a) associated with the long-term risk for CV death. Some types of fats/fat isomers were associated with long-term risk for CV death. However, the association between Lp(a) and CV death was not impacted by the baseline intake of any type of dietary fat. This suggests that dietary and lifestyle factors other than dietary fat drive the improved CV outcomes observed in other cohorts of individuals with elevated Lp(a).
Previous cohorts have demonstrated that the association between Lp(a) and CV outcomes may be modifiable based on lifestyle. In the ATTICA study, a higher Mediterranean diet score did not influence Lp(a) levels but did abolish the additional risk from Lp(a). 12 In the EPIC-Norfolk study (n = 14,051), those in the top compared to the bottom tertile of a CV health score with an elevated Lp(a) had a hazard ratio of 0.33 (95% CI 0.17–0.63) for death from coronary heart disease or stroke. 11 Thus, we anticipated that fatty acids could impact the relationship between Lp(a) and CV death. The most likely explanation for the absent modification effect of fatty acids is a more complex relationship between diet, Lp(a), and CV death. Lp(a) is known to be a preferential carrier of oxidized phospholipids (OxPL), which may explain the higher per-particle atherogenicity of Lp(a). 15 Furthermore, although data are mixed, there is a suggestion that Lp(a) is more atherogenic in the setting of elevated inflammatory markers (i.e. high-sensitivity C-Reactive Protein).16–21 It may well be that dietary fats alone are an insufficient driver of Lp(a)'s atherogenic inducing mechanisms (including via elevated high sensitivity C-Reactive Protein or OxPL). Future studies may require evaluating additional macronutrients, more complex dietary patterns, and additional biomarkers to understand diet's association between Lp(a) and CV disease.
Interesting associations were seen with individual fatty acids and CV death. Early data suggested that higher intake of saturated fat is associated with increased adverse CV outcomes.22,23 Some studies have demonstrated an inverse relationship.24–26 In ARIC, medium- to long-chain saturated fats associated with CV death. This was not seen in NHANES, although point estimates were mostly above 1.0. This may have been due to different sampling methods. One long-chain saturated fat, stearic acid, was positively associated with CV death in the both samples. This is consistent with some prior studies in which stearic acid and other medium- to long-chain saturated fatty acids associate with and increased risk for coronary disease. 27 Current understandings on the relationship between saturated fats and CV outcomes continue to evolve but remain incomplete on how to consider saturated fats’ impact on CV risk. Furthermore, CV risk could be related to other factors that in some studies may correlate with intake of saturated fats (e.g. animal versus plant food sources). Lastly, eicosenoic and docosahexaenoic acid were suggested to be protective for CV death. This is consistent with prior literature.28–30 Overall these observations suggest that long chain unsaturated fats are preferential in the diet versus medium- to long-chain saturated fats. This is in line with recent dietary guidelines to improve cardiovascular health, which recommendation to limit intake of fats from tropical oils and animal sources that tend to have a higher content of medium- to long-chain saturated fats. 31
Our study had limitations. Both cohorts contained data from cross-sectional baseline dietary intake. Food choices change over time and recurrent sampling may be needed to capture these changes. The two studies sampled diet with different methods and intervals. The cross-sectional and short sampling periods are major limitations to the data and may be insufficient to capture actual dietary habits or reflect longitudinal dietary intake. Future studies seeking to understand the association between dietary factors and Lp(a)-mediated risk should utilize longer periods or recurrent dietary recall. Additionally, we set the p-value for significance for interactions at 0.05 since we studied a large number of variables. However, it may be reasonable to set a p-value for interaction significance at 0.10.
Conclusion
We did not find evidence that dietary fat intake modifies the relationship between Lp(a) and CV mortality. However, the relationship between these variables is complex and may not have been fully captured in these datasets. While we await therapies to address elevated Lp(a), clinicians should continue to focus on treatment of traditional risk factors and promote healthy lifestyles that associate with lower risk for ASCVD. The impact of lifestyle factor (such as dietary patterns and exercise) on the association of Lp(a) with CVD should continue to be studied.
Footnotes
Author contributions
Conceptualization: EJB. Methodology: EJB. Formal analysis and investigation: CC and EJB. Interpretation: NP, CC, and EJB. Writing—original draft preparation: NP, CC, and EJB. Writing—review, editing, and final approval: NP, CC, and EJB.
Availability of data and materials
Data are available for access through two methods and are not sharable from the authors directly. ARIC are available via requests to BioLINCC, which requires a signed agreement. NHANES data are freely available for download from the CDC website. The authors are agreeable to sharing Stata coding for the analysis when requested.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EJB has received consulting fees from New Amsterdam Pharmaceuticals.
Ethical approval
This study was reviewed and deemed exempt by the University of Michigan institutional review board (HUM00203926).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.