
Abstract
Background
In Mexico less than half of the treated hypertensive patients reach blood pressure (BP) targets. Most hypertensive individuals rely on the standard medical care (SMC) to achieve the BP control goals; however, the efficacy of BP telemonitoring (BPT) to achieve BP targets has been poorly studied.
Aim
To compare the efficacy of BPT versus SMC to achieve BP goals in patients with uncontrolled hypertension.
Methods
A two-arm, open-label clinical trial was conducted in patients ≥18 years with uncontrolled hypertension. The participants were randomized to 2 arms (BPT vs SMC) and followed for 12 weeks. For the statistical analysis, the chi-squared test and covariance were used.
Results
One hundred and seventy-eight participants were included, BPT (n = 94) and SMC (n = 84), after 12 weeks of follow up, we observed a baseline-adjusted reduction in systolic BP with both BPT (−13.5 [1.3] mmHg) and the SMC (−5.9 [1.4] mmHg; p < 0.001) but a greater decrease with BPT (p < 0.001). Likewise, we found a baseline-adjusted reduction of diastolic BP with BPT (−6.9 [0.9] mmHg) and SMC (−2.7 [0.9] mmHg) (p = 0.007) with a more significant percentage change from baseline with BPT (−6.8% [1.0] vs 2.5% [1.1]; p = 0.007). In the BPT arm, a larger proportion of patients achieved the BP target versus SMC (30.5% vs 12.8%; p = 0.005).
Conclusion
BPT showed a greater proportion of patients achieving office BP control goals (<140/90 mmHg), compared to standard medical care.
Introduction
According to the last 2018 Health and Nutrition Survey (ENSANUT), 1 Mexico has a high prevalence of chronic diseases such as arterial hypertension and type 2 diabetes mellitus (T2DM), with estimated 15.2 million people (18.4%) and 8.6 million people (10.3%), having these conditions, respectively. This causes a great burden to the health system in Mexico. One of the main challenges of the medical community in the management of chronic diseases, such as hypertension, is to achieve the therapeutic goals required to reduce the risk of cardiovascular complications and target organ damage. ENSANUT also reports that 54.4% of treated hypertensive individuals don’t achieve therapeutic goals. 1 Some medical societies of hypertension, 2 cardiology, and diabetes, 3 propose home “self-monitoring” as a means to reach therapeutic targets.
Telemedicine emerges as an approach to treat and monitor chronic disease, it has shown to improve treatment compliance, clinical outcomes, and eating habits. 4 In the case of developing countries, in addition to helping reduce patient overload in health services, this form of healthcare would be especially useful in isolated communities, making access to healthcare possible. 5
The study was designed to identify the primary endpoint: the proportion of patients achieving office blood pressure (BP) control goals (<140/90 mmHg), and as a secondary endpoint, to compare the difference in BP reduction between groups. This was achieved with the use of an app-based BP telemonitoring (BPT) approach versus the standard medical care (SMC) in patients with uncontrolled office BP (≥140/90 mmHg). This app-based approach synced a smartphone with an automatic oscillometric BP monitor and allowed real-time BP recording transmission to a web-based platform that enabled physicians to monitor their patients. We hypothesized that hypertensive patients on BPT would undergo a greater BP reduction and a higher percentage of individuals would achieve BP targets compared to the SMC.
Subjects and methods
Study design
A two-arm, open-label clinical trial was conducted in participants ≥18 years, with uncontrolled hypertension to identify the proportion of patients achieving office BP control goals (<140/90 mmHg) and differences in systolic (SBP) and diastolic blood pressure (DBP) reduction when comparing the use of BPT versus SMC. The Research Ethics Committee of the University Center for Health Sciences of the University of Guadalajara approved the research protocol with the number: CI-03921. This study adhered to ethical guidelines established in the 1975 Declaration of Helsinki and its last amendment in Fortaleza, Brazil (2013) and under the 17th article observed in the General Health Law on Health Research.
Study participants
We included individuals ≥18 years old, men and women, with uncontrolled hypertension (≥140/90 mmHg, measured in the office), without T2DM, thyroid, liver, or kidney diseases, changes to medication in 3 months prior to the intervention and, alcohol or tobacco abuse, who attended medical consultation with physicians who belong to the GREHTA (Grupo de Expertos en Hipertensión Arterial) /ANCAM (Asociación Nacional de Cardiólogos de México) network for their BP treatment and monitoring. The GREHTA and ANCAM is a group of cardiologists and noncardiologist physicians certified in hypertension treatment. Patients were treated by their specialist doctors belonging to the GREHTA/ANCAM network.
The design, coordination, processing, and analysis of data were carried out at the Vascular Mechanics Laboratory of the Experimental and Clinical Therapeutics Institute (INTEC) of the Department of Physiology at the University of Guadalajara, México. Informed written consent was obtained from all the participants.
Intervention
BPT group
Once the informed consent to participate was signed, a complete clinical history was obtained, and BP levels were measured according to the 2018 ESC/ESH Guidelines for the management of arterial hypertension. 6 BP was measured with the validated Omron HEM-9200T 7 oscillometric sphygmomanometer.
Follow up was carried out with the Magentrack® web-based platform and mobile phone app, to sync with medical devices and receive information like BP, glycemia, and anthropometric parameters (body fat, body mass index). This enables the constant interaction between patients and health professionals who monitor health variables. With optimal use, it can reduce care costs, morbidity rates and improve adherence to treatment. Another benefit is that it emits alerts in real-time allowing emergency adjustments to treatment (when required). Data from measurements could be obtained from automatic synchronization or by manual upload. In addition, immediate alerts can be generated to establish attention priorities and consequently take pertinent actions that in our study were specifically related only to BP monitoring as detailed below.
At baseline, all the physicians registered the patients on the platform and synced the BP monitor. Study patients were trained personally by their doctors and given a pamphlet with instructions on how to use BP monitors and how to measure BP correctly at home according to the guidelines for home BP monitoring as highlighted by Parati et al. 8 All the patients underwent a learning curve ultimately allowing them to manage the device and app. A 1-week run-in period was carried out to guarantee the correct use of the application after which, randomization was carried out through the generation of random numbers by a computer. At home, BP measurements were sent to and recorded in the Magentrack servers where the physicians reviewed BP levels weekly. For the security of the study participants, the app was programmed to send alerts to the physician's mobile phone during follow up in case of BP levels were ≥140/90 mmHg or ≤100/60 mmHg and to give medical advice to the participants. No standardized treatment optimization strategies such as dose escalation, drug combination, or even drug switching were carried out by the physicians.
SMC group
The follow up of the control group consisted of usual medical visits to monitor and adjust treatment based on office BP levels. Office visits happened every 3 to 4 weeks and between visits, there was no communication between the study participants and their physicians.
Evaluation of BP monitoring usability
The Spanish-validated 9 questionnaire “Telemedicine Usability Questionnaire” (TUQ) developed by Parmanto et al. 10 was applied at the end of the study to evaluate the ease of BPT use and to identify its main usability problems.
Statistical analyses
Continuous numerical values are expressed as mean and standard deviation. A Chi-square test was used to compare categorical variables. To determine the effect of BPT versus standard care on BP levels, an analysis of covariance was performed. Baseline demographic and anthropometric characteristics were assessed and used as covariates if significantly associated with SBP and DBP difference after the intervention. RStudio® software version 1.3.1073 (Vienna, Austria) was used for statistical analysis, and GraphPad Prism® software version 8 (San Diego, CA, USA) for graphical representation. The statistical analysis was performed blinded. We considered a two-tailed p ≤ 0.05 as significant.
Sample size calculation
The primary endpoint sample size was calculated using data from a previous study by Piette et al. 6 that reported the achievement of BP goals in 57% of patients using BPT, compared to 32% in the control group (SMC). The sample size for Chi-square test resulted in a total of 170 individuals, including a 20% patient loss during the study, with a statistical power of 80% and an alpha of 5%. Sample size calculations were performed using GPower software v.3.1 (Heinrich Heine University, Dusseldorf, Germany).
Results
Two hundred and eleven participants were assessed for eligibility but only 188 individuals were not on BP target (<140/90 mmHg) at the time of the office visit. Of these, 94 were assigned to the BPT group and 84 to the SMC (i.e. control) group, as shown in the flowchart (Figure 1). The age, sex, weight, and baseline BP levels were similar between both groups (Table 1). The most used antihypertensive drugs were angiotensin receptor blockers, angiotensin-converting enzyme inhibitors, calcium channel antagonists, and beta-blockers, in order of frequency, respectively, in both groups.

Flow chart of participants enrolled in the study.
Demographic characteristics and blood pressure levels at baseline.
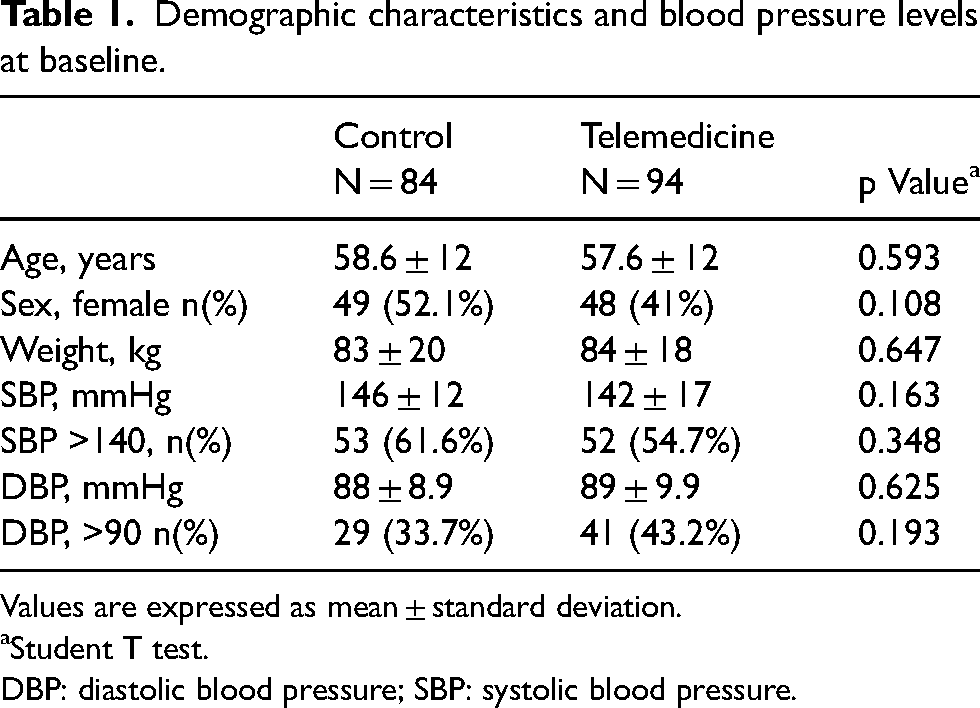
Values are expressed as mean ± standard deviation.
aStudent T test.
DBP: diastolic blood pressure; SBP: systolic blood pressure.
There was a statistical difference between baseline and final SBP and DBP after 12 weeks of follow up, hence, only baseline BP levels were accounted for as covariates. We found a significant reduction in adjusted and unadjusted reduction and percentage change in SBP and DBP in both the SMC and BPT groups. The absolute reduction in BP and percentage change were greater in the BPT group (both p < 0.01) (Figure 2). Likewise, the BPT group achieved a greater percentage of individuals at BP goals compared to SMC (+17.7%; p = 0.005) (Table 2). All patients in the BPT group reported it was easy to use the app, through the TUQ.

Percentage change adjusted to baseline BP levels in controls versus telemedicine. Error bars represent standard errors. BP: blood pressure; DBP: diastolic BP; SBP: systolic BP.
BP levels before and after 12 weeks between groups and BP target.

Values are expressed as mean ± standard deviation and estimated mean (standard error).
Adjusted percentage change and difference was performed with analysis of covariance with baseline systolic and diastolic levels as covariate, respectively.
aChi-square test.
ad.: adjusted; un.: unadjusted; BP: blood pressure; DBP: diastolicBP; SBP: systolic BP.
Discussion
Home BP monitoring is a pioneering field for research in telemonitoring or telemedicine. Since automated electronic BP monitors became available for blood pressure measurement at home, researchers started investigations to identify the possible effects of telemonitoring on BP control. 11
Over the past decades, the progressive improvement in both technical devices and software availability allowed rapid transmissions of high-quality data between individual patients and referring physicians even through large distances. This novel approach has been adopted with benefits in the clinical management of different cardiovascular diseases, including hypertension.12,13
In our study, we used an app-based BPT approach in patients with hypertension to demonstrate the benefit of a close interaction between the patient and the physicians, using BP measurement synced via Bluetooth with a mobile phone app. This established an easy and practical communication network between physicians and individuals with hypertension, which reflected in a significant reduction in SBP > 10 mmHg and DBP > 5 mmHg after 12 weeks of follow up.
Our results agree with the first randomized controlled trial on home BPT that was conducted on 267 patients recruited from communities in the United States followed for a period of 6 months. The conclusion of this study was that telemonitoring with an automated telephone transmission system improved treatment adherence and BP control with a reduction of 4.7/4.4 mmHg (SBP/DBP, respectively) compared to the SMC control group (p ≤ 0.02). 14
Friedman et al. 14 showed that participants in the telemonitoring group reported weekly self-measured BPs, adherence to antihypertensive medication regimens, and medication side-effects. This information was sent to their physicians regularly, and the main study outcome measures were changes in antihypertensive medication adherence. Several studies have been carried out and analyzed through a meta-analysis, as reported by Parati et al., 15 who mentions the different strategies, heterogeneity of groups, sample sizes, and their results in favor of telemedicine and its complementarity in routine clinical practice for BP control. In our study, an extra benefit was that physicians received an alert generated by the software when the BP levels exceeded the pre-established cut-off points, which enabled communication and attention to the patients when the physician considered it pertinent. We assume that the improvement in BP and the superiority in the achievement of goals in the BPT group, could be related to this and to the greater attention patients received. It is possible that the different alerts that were generated to remind the patient of administration schedules, dose and, BP recordings perhaps also increased self-care motivation and adherence to their antihypertensive treatment, although these assumptions are only hypotheses that could perhaps be verified in a follow-up study.
Second, SBP and DBP reduction in the BPT group was practically the double of that in the SMC group. It should be noted, as mentioned in the methodology, that patients in the control group did not receive BP measurement reminders or specific instructions via text messages from their physicians, unless there was a hypertensive emergency. By using the SMC group as a control, we aimed to reflect the traditional scenario of hypertensive patient management, where therapeutic decisions are made based only on office BP.
In agreement with our results, evidence from randomized studies16,17 suggests that home BPT, defined as home BP monitoring coupled with telematics data transmission to the physician and real-time feedback, improves BP control, treatment compliance, and may help in optimizing the patient's therapeutic regime.
Limitations
Although we know that the threshold for arterial hypertension diagnosis at home is ≥135/85 mmHg, the alerts generated by the app were issued considering the BP threshold taken at the office; therefore, this 5 mmHg gap for both SBP and DBP, underestimates the real percentage of patients out of the target at home.
The fact that the intervention in the BPT group was left to the treating physician’s criteria accounted for possible unfactored variability.
Another important limitation of our study is that characteristics like medical history, BP treatment, and body mass index (BMI) were not considered in the design of the protocol.
Conclusion
To our knowledge, this is the first study that demonstrates the efficacy of BPT in Mexico. BPT proved to be superior to SMC to reach therapeutic BP goals and decrease BP. All patients in the BPT group reported it was easy to use the app, through the TUQ.
Footnotes
Acknowledgements
We would like to thank all the members of the Magentrack company for offering the virtual platform and applications for mobile phones, that facilitated remote data acquisition and BP monitoring, as well as the training and assistance to both the researchers and patients who participated in this study; we would also like to thank OMRON Medical, México who provided the oscillometric BP monitors.
Statement
All the data provided in our manuscript and any underlying research materials related to our paper (for example data, samples, or additional information) can be accessed when needed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MEG.