
Abstract
Objectives
Postoperative pleural effusion (PE) is common after pediatric cardiac surgery, and if prolonged can lead to the deterioration of the general condition due to malnutrition and result in death. This study aims at identifying the prognostic factors of prolonged PE after pediatric cardiac surgery.
Participants
Participants included patients who had prolonged PE after cardiac surgery in national center for child and health development between October 2014 and October 2017.
Main outcome measures
Baseline characteristics and procedure details were compared between the two groups to determine the predictor of prolonged PE. White blood cell count, platelet count, neutrophil-to-lymphocyte ratio, hemoglobin level, serum total protein level, serum albumin level, blood fibrinogen level, serum creatinine level, etc. were examined.
Results
Twenty patients were included. Between the two groups, no significant differences in baseline characteristics, such as age, weight, and sex were found, and significant differences were observed only in the NLR change ratio (effective group, 5.1 [4.1–8.0] versus ineffective group, 11.9 [9.9–14.1]; P = 0.01).
Conclusions
NLR change ratio is a potential prognostic factor of prolonged PE, including chylothorax, after pediatric cardiac surgery.
Keywords
Introduction
The incidence of chylothorax after pediatric heart surgery is reported to be 2%–5%.1–3 It is a common complication and if prolonged, may results in long hospital stays, high medical costs, and high mortality due to malnutrition. There is no established treatment strategy as different healthcare facilities use different strategies.1,4 Treatment is classified into three categories: nutritional, medical, and interventional therapy. Nutritional therapy is defined as fasting with parenteral nutrition. Medical therapy includes administration of steroids, 1 factor XIII concentrate, 5 octreotide, 6 or etilefrine.7,8 Interventional therapy is indicated when conservative approaches of nutritional and medical therapy are unsuccessful. Interventional treatments, including thoracic duct ligation, lymphaticovenular anastomosis, and lymphangiography, 9 are so invasive and therefore not considered as first-line therapy. If the predictor of prolonged pleural effusion (PE) is clearly determined, the choice of interventional treatment can be easily and appropriately made before the deterioration of the general condition of the patient. Prolonged postoperative PE, if not necessarily chylothorax, is often seen clinically. Because PEs are commonly seen after cardiac surgery, PEs that are not chylothorax have not been investigated a lot. However, if the normal PE was prolonged, the general condition may worsen because of malnutrition. We believe with conviction that there is no significant difference in the clinical course between prolonged non-chylothorax and chylothorax. However, the incidence of prolonged PE after pediatric cardiovascular surgery is still unknown. The incidence of pediatric cardiac surgery in which the drain remained in place for more than 2 weeks was reported to be 27.4%–42.4%,10–12 but this is a summary of cases of total cavopulmonary connection (TCPC).
Common causes of PEs are increased hydrostatic pressure, enhanced vascular permeability, and decreased collagen osmolarity. 13 Previous studies have reported that increased hydrostatic right-sided pressure was a risk factor for PE,12,14 but some studies also reported that postoperative fluid balance was not a risk factor for the development of PE. 15 We hypothesized that enhanced vascular permeability due to systemic inflammation is one of important etiological factors. Although PE is often a symptom of chronic inflammatory diseases, such as connecting tissue, 16 there are few reports discussing the association between PE and systemic inflammatory response after cardiac surgery. Gupta et al. used interleukin 6 (IL-6) as a systemic inflammatory marker to evaluate the relationship between pleural fluid volume and inflammatory response, but the results showed only a weak correlation 17 ; however, anti-inflammatory steroids often used in PEs 1 suggest that a systemic inflammatory response may contribute to process PEs. Neutrophil-to-lymphocyte ratio (NLR) is a highly sensitive marker of inflammatory reactions and is known to be a prognostic factor of a wide range of cardiovascular diseases, including stable angina, 18 myocardial infarction, 19 and peripheral vascular disease. 20
The present study aims to investigate the predictors of the efficacy of medical therapy for postoperative prolonged PE. If predictors of treatment efficacy can be deciphered, their presence may contribute to the establishment of treatment strategies.
Methods
This study was a single-center retrospective observational cohort study that was started after obtaining permission from the ethics committee of National Center for Child Health and Development (NCCHD 2019–124). This study was also registered in the Japan Registry of Clinical Trials (jRCT1031200009). Patient consent was obtained by opt-out in this study and the study was conducted according to the Declaration of Helsinki.
This study was performed at NCCHD and included all patients aged ≤7 years who underwent cardiac surgery and developed prolonged postoperative PE between October 2014 and October 2017. In our institute, we defined prolonged PE as PE of >20 mL/kg/day after postoperative day 4 or >6 mL/kg/day after postoperative day 7. The reason for this is that historically, our hospital has believed that this standard should be used for medical interventions. Even if the values of triglyceride and lymphocytes are low in such prolonged PE, it was clinically considered to be chylothorax and treated. Therefore, all patients with prolonged PE were treated clinically as chylothorax. Patients with lymphatic injury at surgery, who underwent extracorporeal membrane oxygenation, who were with congenital chylothorax, who diagnosed with neonatal necrotizing enterocolitis, and who were with a history of allergy to octreotide or factor XIII concentrate were excluded from the study.
Patients with prolonged PE were treated according to the protocol shown in Figure 1. Oral intake was paused, and total parenteral nutrition was commenced instead. Infusion of octreotide (Sandostatin, Novartis Pharma, Basel, Switzerland) or factor XIII concentrate (Fibrogammin P, CSL Behling, Pennsylvania, United States) was administered. Medical treatment methods were assigned to each case by a random number generation program. Octreotide was administered intravenously at a dose of 2.0 mcg/kg/hour 21 and the factor XIII concentrate was administered intravenously at a dose of 40 IU/kg per day. 22 Octreotide was initially administered for 5 days and extended if it was deemed necessary to continue the administration. The administration period of the factor XIII preparation was specified as 5 days. If PE was less than 6 mL/kg, fat-restricted diet or medium-chain triglyceride milk was initiated. Fat-restricted diet was terminated if the drained PE after the initiation of the fat-restricted diet did not exceed 6 mL/kg. If the drained pleural fluid did not exceed 6 mL/kg after the termination of the fat-restricted diet, the chest tube was removed.

Flowchart of the management of prolonged pleural effusion. POD, postoperative day; TPN, total parenteral nutrition; MCT, medium-chain triglycerides.
The endpoint of the study was chest tube removal within 10 days after medical therapy. On the 10th day after medical therapy, the group of patients whose drain tubes were removed was defined as the effective group, and the group whose drain tubes were not removed was defined as the ineffective group. Patient data, including age, sex, body weight, type of procedure, operation time, central venous pressure (CVP) on the day of surgery, preoperative systolic blood pressure, preoperative heart rate, preoperative blood oxygen saturation, preoperative tracheal intubation, whether preoperative oxygen administration and hypoxia therapy were given to the patient, the number of days from surgery to the start of medical treatment, and whether there were postoperative inflammatory complications were compared between the two groups. Laboratory data obtained before surgery and before medical therapy were also collected. Factors such as white blood cell (WBC) count, platelet count, NLR, hemoglobin level, serum total protein (TP) level, serum albumin level, blood fibrinogen level, serum creatinine level, blood urea nitrogen (BUN) level, serum aspartate aminotransferase (AST) level, serum alanine transaminase (ALT) level and serum C-reactive protein (CRP) level, were also compared between the two groups. Normal WBC count, neutrophil count, lymphocyte count, and NLR are known to vary by age; therefore, changes in these variables were examined before surgery and before medical therapy. The NLR change ratio was calculated by dividing the NLR before medical treatment with the NLR before surgery. The WBC, neutrophil, and lymphocyte count change ratios were also calculated in the same way.
Statistical analysis of baseline characteristics and clinical data of the study population was performed. For continuous values, the non-parametric test was used because they were clearly not normally distributed. Baseline characteristics were expressed as medians with interquartile ranges for continuous variables and as numbers with percentages for categorical variables. Continuous data were analyzed using Mann–Whitney test, and categorical data were analyzed using Fisher's exact test. Correlation analysis was conducted by using Spearman's rank correlation coefficient. Two-sided P < 0.05 was considered to indicate statistically significant difference. The analyses were performed using Easy R software version 1.32 (The R foundation for statistical computing). 23
Results
Among the 366 patients under 7 years of age who underwent cardiac surgery between October 2014 and October 2017, prolonged PE was observed in 20 patients (5.5%). These 20 patients were enrolled in our study. The median age of patients was 11.9 months (3.9–22.2 months), and the median body weight was 8.4 kg (4.8–9.8 kg). Eleven patients had single-ventricle physiology, and medical therapy was started 5.5 (5–6) days after cardiac surgery. The surgeries performed on the 20 patients were as follows: TCPC (9 patients), arterial switch operation (4 patients), Norwood procedure and bidirectional cavopulmonary shunt (2 patients), tetralogy of Fallot repair (1 patient), double-outlet right ventricular repair (1 patient), complete atrioventricular septal defect repair (1 patient), Rastelli procedure (1 patient), and unifocalization of major aortopulmonary collateral artery and modified Blalock–Taussig shunt (1 patient). All surgeries were performed electively.
Table 1 shows the baseline characteristics and clinical data of the two groups. There were no significant differences between the two groups. Preoperative catheterization was performed in 9 patients in the effective group and 9 patients in the ineffective group. There was no significant difference in preoperative CVP between the two groups (effective group, 10 mmHg [5–10] versus ineffective group, 7 [7–10]; P = 1.0). There was no significant difference in postoperative CVP between 7 patients in the effective group and 9 patients in the ineffective group (effective group, 14 mmHg [7–15] versus ineffective group, 14 [11.5–14]; P = 1.0).
Baseline characteristics and clinical data.
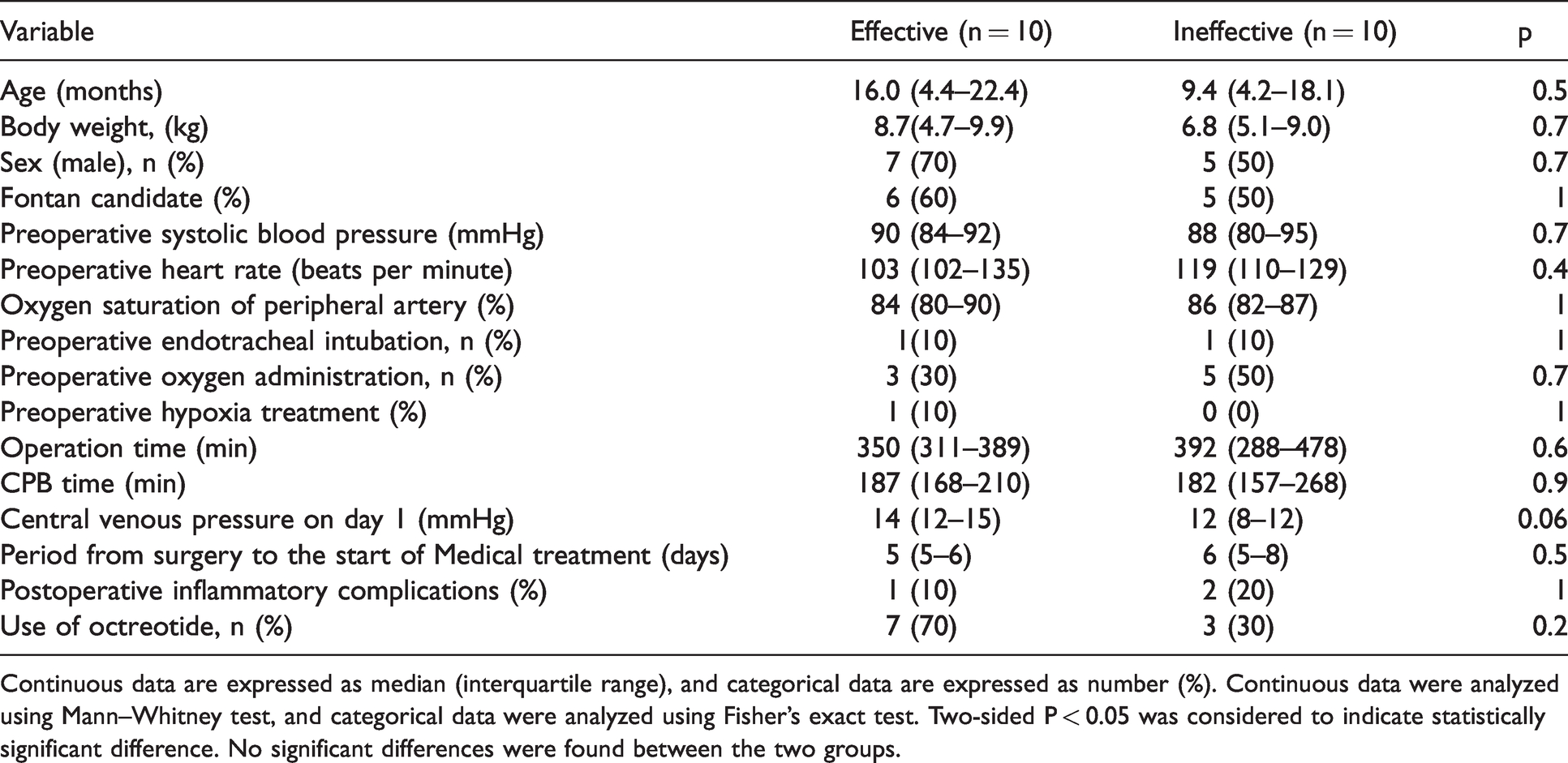
Continuous data are expressed as median (interquartile range), and categorical data are expressed as number (%). Continuous data were analyzed using Mann–Whitney test, and categorical data were analyzed using Fisher's exact test. Two-sided P < 0.05 was considered to indicate statistically significant difference. No significant differences were found between the two groups.
Table 2 shows the comparison of factors before surgery and before medical therapy between the two groups. Between the two groups, no significant differences in WBC count, neutrophil count, lymphocyte count, hemoglobin, platelet count, TP, albumin, fibrinogen, CRP, Creatinine, BUN, AST, and ALT level before surgery and before medical therapy were found; however, a significant difference in NLR change ratio was observed (P = 0.01).
Comparison of factors relating to systemic inflammation.

CRP: C-reactive protein; NLR: neutrophil-to-lymphocyte ratio; TP: total protein; BUN: blood urea nitrogen; AST: aspartate aminotransferase; ALT: alanine transaminase.
Continuous data are expressed as median (interquartile range). Data were analyzed using Mann–Whitney test. Two-sided P < 0.05 was considered to indicate statistically significant difference. Only postoperative/preoperative NLR was significantly different between the two groups.
The receiver operating characteristic curve for NLR change ratio in correlation with chest tube removal within 10 days after medical therapy is shown in Figure 2. The area under the curve for NLR change ratio was 0.82 (95% confidence interval, 0.608–1), and the cut-off value was 8.13. NLR change ratio was found to be predictive of chest tube removal within 10 days after medical therapy with 80.0% sensitivity and 80.0% specificity. We divided the population into two groups: those with NLR change ratios of 8 or more and those with less than 8. The log-rank test was used to determine the number of days after medical intervention for chest tube removal (Figure 3). The number of days after medical intervention for chest tube removal was significantly higher in the group with NLR change ratios of 8 or more than in the group with NLR change ratios less than 8 (P = 0.01).
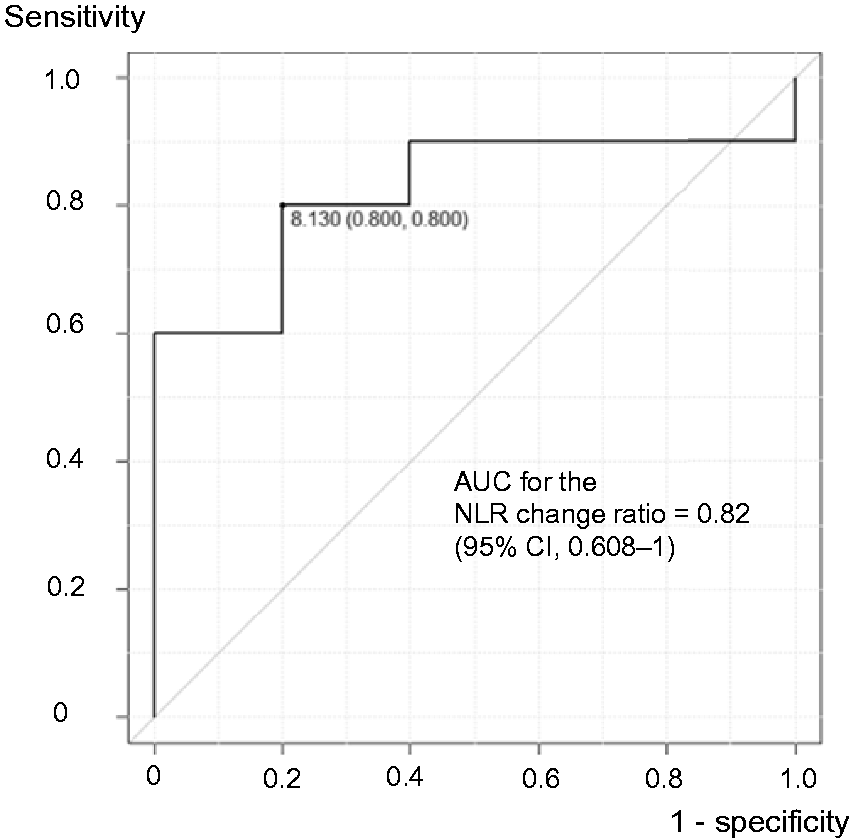
Receiver operating characteristic (ROC) curve for NLR change ratio in correlation with chest tube removal within 10 days after the start of medical therapy. The vertical axis depicts sensitivity, and the horizontal axis depicts specificity. The black line shows the ROC curve, and the area under curve is 0.82 (95% CI, 0.608–1). When the cut-off value is set to 8.13, the sensitivity and specificity are both 80%.

Rate of chest tube indwelling in patients with prolonged pleural effusion after pediatric cardiac surgery. The vertical axis represents the percentage of patients with a chest drain tube inserted in the total group. The horizontal axis represents the number of days since the medical treatment has started. The solid line shows the group of patients whose NLR change ratio is less than 8. The dashed line shows the group of patients with NLR change ratio of 8 or more.
The relationship between the NLR change ratio and hemoglobin, TP, albumin fibrinogen, CRP, BUN, and creatinine level was investigated (Table 3). However, no apparently significant correlation was found between the NLR change ratio and these parameters.
Correlation between NLR and each test data.

The correlation between NLR and each test data is expressed by Spearman’s rank correlation coefficient, which is denoted as ρ. Two-sided P < 0.05 was considered to indicate statistically significant difference. No correlation was found among these examined data.
Discussion
To the best of our knowledge, this is the first study that focuses on prolonged PEs in overall pediatric cardiac surgery. The definition of prolonged PE in this study is as described in the previous sections, and the definition in other studies 2 –3 is defined as a condition in which a drain is inserted for a period longer than this study. The reason for adopting that criterion is that, as mentioned earlier, this has historically been the criterion for therapeutic intervention for PEs in our hospital. This is a result of our efforts to intervene early, before the systemic condition worsens.
This study examines the prognostic factors of medical intervention for prolonged PE. However, there are similarities between the search for causes and the search for prognostic factors, because if the extent of the cause is severe, the effect of treatment is unlikely to be good. Common causes of PEs are thought to be increased hydrostatic pressure, enhanced capillary permeability, and decreased osmotic pressure of collagen. 13 However, there is no known cause of postoperative PE at present. It has been reported that the risk factor is the absence of fenestration and high preoperative pulmonary artery pressure in TCPC.10–12 It is also said to be related to hydrostatic pressure in the right heart system.12,14 However, some reports have shown no correlation between infusion load and incidence. 15 There was no association between preoperative and postoperative CVP on the responsiveness to medical therapy in this study.
In the present study it was hypothesized that decreased vascular permeability may be the cause of PE, and inflammatory biomarkers and their response after medical treatment were investigated. Regarding postoperative PE and biomarkers in pediatric cardiac surgery, Luo et al. reported that preoperative hemoglobin level, preoperative platelet level, preoperative AST, preoperative ALT, postoperative lymphocyte count, postoperative AST, and postoperative CRP were associated with postoperative prolonged PE. 10 Factors related to inflammatory response and collagen osmolality were examined in our study. Only the rate of change in NLR was found to be associated with PE, whereas nothing significant between the biomarkers as shown by Luo et al. was observed in the present study.
NLR value is obtained by dividing blood neutrophil count by blood lymphocyte count. There are many reports of NLR as a prognostic factor of cancer, peripheral artery disease, 20 and acute myocardial infarction. 19 NLR is also associated with postoperative atrial fibrillation after cardiac surgery. 24 NLR can easily be determined from the results of routine blood examination, and no special equipment is required. However, there is no established normal value of NLR. Patrice et al. reported that the normal range of NLR is 0.78–3.53, 25 but another study 26 reported that NLR varies across races. Although NLR has been found to be a prognostic predictor of various diseases, the set cut-off values differ between studies. Normal values in children probably vary with age; therefore, appropriately determining the cut-off values is difficult. Therefore, as shown in our study, NLR change ratio from baseline may be a more appropriate prognostic factor than just NLR. Elevated NLR change ratio of 8 or more was shown to be a potential prognostic factor of prolonged postoperative PE in this study. There is no established ideal strategy for refractory postoperative PE. The overall outcome of pleural fluid treatment could be improved if prognostic factors could be identified for medical treatment of PEs. Overall outcomes may improve if surgical or catheter intervention is performed at appropriate times based on ideal strategy.
NLR has been reported to be a prognostic factor of several pathological conditions.18–20 However, to the best of our knowledge, no report has clearly described the pathophysiological mechanism. This lack of understanding of the pathophysiological mechanism is a major problem when considering NLR. The mechanism underlying the development of prolonged PE after cardiac surgery also remains unclear. There is likely a positive correlation between NLR and the incidence of postoperative PE. One possibility is that nutritional impairment because of PE increases the NLR. Previous studies have shown that factors associated with low nutrition, such as low prothrombin time and low TP, are associated with prolonged PE. 10 Although the mechanism is still unknown, lymphocyte count is a common indicator of nutritional status in clinical practice. Therefore, if the patient is hypotrophic because of PE before initiating medical therapy, the NLR may be elevated. Therefore, NLR may be elevated if there is loss of nutrition because of PE.
We hypothesized that another possible involvement of interleukin 17 A (IL-17A) may be one of the reasons why NLR is a predictor of the efficacy of medical treatment for prolonged PE. IL-17A is mainly produced by CD4+ T cells called Th17 cells. IL-17A is a cytokine that increases neutrophil production through chemokines. As mentioned above, single ventricular circulation is known to be one of the risk factors of prolonged PE after pediatric cardiac surgery, and it has been reported that IL-17A levels are higher in patients with PE and single ventricular circulation than in patients with PE and biventricular circulation. 27 IL-17A is also known to enhance the permeability of blood vessels and the blood–brain barrier28,29 and may lead to prolonged PE and elevated NLR.
This is a hypothesis about the mechanism of NLR increase. However, although the mechanism of NLR elevation has been investigated in various situations, it has never been clearly identified. We believe that further research, including employing clinical and basic experiments, is necessary to clearly determine the underlying mechanism of prolonged PE.
The limitations of this study include its single-center design, its retrospective observational nature, and the small patient number. If multicenter studies with a larger number of patients are conducted, the accuracy of the decision-making process will increase and better strategies for prolonged postoperative PE after pediatric cardiac surgery can be designed by determining the normal values of NLR for each month of age.
Conclusion
NLR change ratio is a potential prognostic factor of refractory PE (including chylothorax) after pediatric cardiac surgery. Postoperative PEs in pediatric cardiac surgery may involve a variety of causes. Further research is needed to establish therapeutic strategies to improve outcomes and to elucidate of the mechanism of NLR elevation.
Footnotes
Acknowledgments
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of national center for child health and development provided ethical approval (NCCHD 2019-124).
Guarantor
KY
Contributorship
KY: Concept, design study, data analysis technique, data acquisition, article draft, revision and approval.
KM: Revision and approval.
TK: Revision, concept, supervise and approval.
TM: Supervise and approval.
MO: Supervise and approval.
YK: Supervise, concept and approval.