
Abstract
Introduction
Hypertension is a global challenge which accounts for high morbidity and mortality rates in the world. The availability of effective anti-hypertensive medications does not result in a good outcome in controlling blood pressure which points towards poor adherence. Thus, this study was conducted to assess the determinants of adherence to anti-hypertensive medication among hypertensive patients on follow-up in Hawassa Referral Hospital.
Methods
Institution-based case–control study was conducted on a sample of 289 clients from February to May 2018. Census was conducted on 1600 clients to select cases and controls. Then, systematic random sampling was used to select study subjects, and adherence was measured by Morisky medication adherence scale. The associations of variables were analyzed using bivariable followed by multivariable logistic regression analyses.
Results
The respondent’s adherence to medication was found to be 67% as measured by Morisky medication adherence scale. The multivariate logistic regression analysis showed that medication adherence was found to be better in younger age (<45) (AOR = 3.8), clients living in urban areas (AOR = 6.84), those clients who had good knowledge (AOR = 3.13), those with no co-morbidities (AOR = 3.14) and patients who controlled their blood pressure (<140/90) (AOR = 2.35).
Conclusions
The rate of medication adherence was found to be low, and hence educational interventions focusing on factors promoting adherence and patients’ health support should be implemented.
Introduction
According to the World Health Organization (WHO), hypertension (HTN) is defined as “a persistent raised systolic or diastolic blood pressure (BP) ≥ 140/90 mmHg in adults aged ≥18 years above”. 1 HTN is often called the “silent killer” because it often has no warning signs or symptoms, and many people do not realize they have it. 2 HTN is a modifiable cardiovascular risk factor, in which early detection, proper management and control of BP can avoid long-term complications by using appropriate treatment plan.3,4
Strong evidence from randomized controlled trials has revealed that the treatment of high BP significantly decreases cardiovascular disease (CVD)-associated morbidity and mortality. 5
However, poor adherence is one of the biggest obstacles in therapeutic control of high BP. 6 Failure to adhere to treatment causes medical and psychological complications of the disease, reduces patients’ quality of life and wastes healthcare resources. 7
In developing countries like Ethiopia, the burden of HTN is becoming critical and increased from time to time due to the expansion of urbanization, sedentary lifestyles, and low level of literacy rate. 8 Untreated or sub-optimally treated HTN could lead to increased risk of morbidity and mortality due to cardiovascular, cerebrovascular or renal diseases. The common reason for poor BP control among hypertensive patients is poor medication adherence. 9
Good adherence to anti-hypertensive medications is necessary in order to achieve BP control and improve outcome.10,11 As there are different factors affecting the adherence of patients to their medication, identifying and understanding the barriers affecting a patient’s ability to adhere to anti-hypertensive therapy will allow to design effective interventions against different barriers of medication use, adherence rates and patient outcomes. Thus, the purpose of this study was to assess the determinants of adherence to anti-hypertensive medication among hypertensive patients on follow-up in Hawassa Referral Hospital (HRH), Ethiopia, 2018.
Methods
Study setting, period and design
The study was conducted at HRH, in Hawassa town, located 219 km away from Addis Ababa, Ethiopia. The study was conducted from February to May 2018 by applying the institution-based un-matched case–control study design.
Eligibility criteria
All hypertensive patients with age 18 and above who have been on follow-up and receiving anti-hypertensive treatment at HRH chronic illness follow-up clinic for at least one month were included in the study.
Operational definition
Sample size determination and procedure
The sample size was computed by Epi-info version 7 by considering a ratio of non-adherent cases to adherent controls of 1:2, power 80, 95% confidence interval and adjusted odds ratio 2.18 with a proportion among cases 0.4 and among controls 0.35. 12
Accordingly, the maximum sample size was 289, among which 96 cases and 193 controls were used. The sample size formula for the method described in Kelsey was used. 13
Institution-based census was conducted on 1600 hypertensive patients on follow-up in HRH using MMAS-8 to select cases and controls (1072 controls and 528 cases). Out of these, the controls and cases were selected by systematic random sampling method with interval of K= 5.
Data collection procedure
Two trained Bachelor degree nurse professionals and one pharmacist collected data using structured questionnaire in two isolated chronic care units.
BP measurement
Three sitting BP measurements were taken in 2 min apart, 14 and the average of the three readings was used to determine the BP level.
Data quality assurance
The interviewer-administered structured questionnaire was translated into local language (Amharic) from its English version and then back to English. Data collection instrument and research procedures were pretested with 30 participants in Bombe Primary Hospital, and some modifications were made on the questionnaire based on the pretest. Training was given for data collectors. Data collectors were supervised while collecting the data by the principal investigator. Data were checked daily for completeness and consistency throughout the data collection period.
Data analysis
Data were checked for completeness, coded and entered into Epi Data Version 4.2, and then exported into SPSS version 25 for data analysis. The MMAS was used to assess the adherence status using ≥ 6 as adherent or < 6 as non-adherent score. Variables with a P-value of less than 0.25 in the bivariable logistic regression analysis were entered into the multivariable logistic regression model for final analysis. A P-value less than 0.05 was considered to determine the statistical significance of the association and odds ratio with a 95% confidence interval was used to determine the presence, strength and direction of association between covariates and the outcome variable.
Results
Socio-demographic characteristics
Participants enrolled in the study were 289 (96 cases and 193 controls) with a 100% response rate. Seventy percent of the respondents were males in both controls and cases. Among the controls, 75% of the respondents were urban residents. Majority of the cases (42.7%) do not read and write. In addition, two-thirds of the respondents were belonging to the age of ≥55 years (Table 1).
Socio-demographic characteristic of the respondents at HRH, 2018.
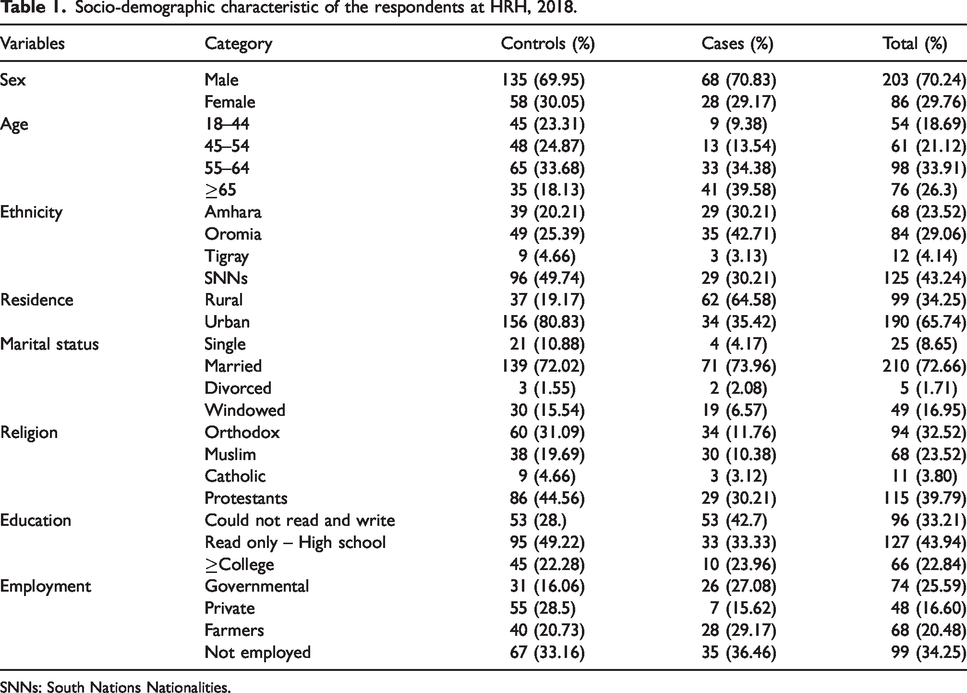
SNNs: South Nations Nationalities.
Respondents’ level of adherence to their anti-hypertensive therapy
Institution-based census conducted using MMAS-8 showed that about more than two-thirds (67%) of respondents were found to be adherent, whereas 528 (33%) were non-adherent to their medication treatment.
Clinical and medication characteristics of the respondents
Thirty-five and 86 respondents among cases and controls, respectively, had co-morbidities. Among the controls, 24% of the respondents had been taking one drug per day. Based on the BP measurement, 61% of the control clients presented with controlled BP, whereas two-thirds of respondents in the cases presented with uncontrolled BP. Among the controls, 15% of respondents have got free health service coverage given by the government (Table 2).
Response regarding medication and clinical characteristics at HRH, 2018.
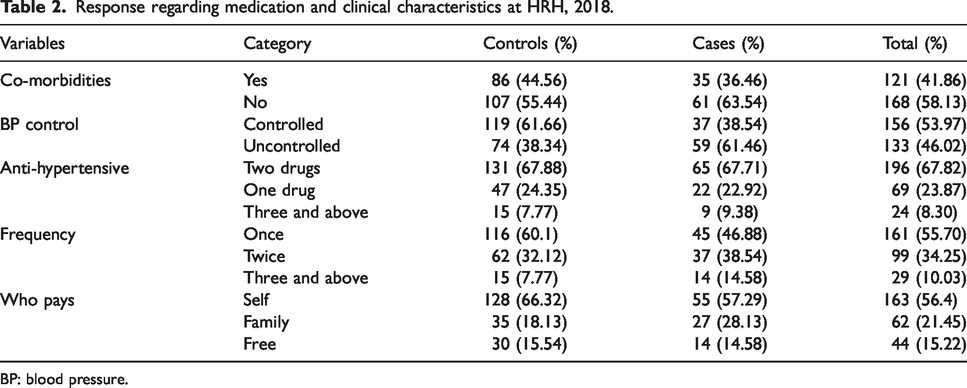
BP: blood pressure.
Knowledge about HTN
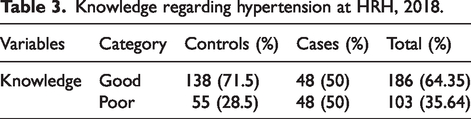
Among controls, 186 (64%) of the respondents have good knowledge about HTN disease and its treatment. Majority of respondents (71.5%) in the control group have good knowledge about HTN (Table 3).
Knowledge regarding hypertension at HRH, 2018.
Patient–provider relationship
Among controls, 133 (46.02%) of the respondents have good relationship with health workers. Twenty-nine (10.03%) of respondents had poor relation with their healthcare providers (Figure 1).

Patient–provider relationship status at HRH, 2018.
Respondents’ reason to their non-adherence behavior
The most common reason was forgetfulness (29.16%) followed by being busy (20.83%) and false perception that they are cured (16.6%) (Figure 2).

Percentage distribution of reasons for being non-adherent to their medication treatment at HRH, 2018.
Respondents’ response regarding life style modification
One hundred and eight (55%) study participants in the controls perform physical exercise. Sixteen percent of the respondents in the case group were smokers. Seventeen percent and 15 percent of the cases and controls were always using salt in their food (Table 4).
Response regarding life style modification at HRH, 2018.

Results of the bivariable and multivariable analyses
This study revealed that respondents of young age group (18–44) were three times more adherent as compared to elderly people (>65) (AOR = 3.80 (1.08, 13.31). Respondents living in urban area were six times more likely adherent than those living in rural area (AOR = 6.84 (3.05, 15.36). Those who have good knowledge were three times more likely adherent than whose knowledge was poor (AOR = 3.13 (11.43–6.82) and those with no co-morbidity were three times more likely adherent than clients with co-morbidity. Those clients who controlled their BP were two times more likely adherent than those not controlling their BP (AOR = 2.35 (1.15, 4.81) (Table 5).
Bivariable and multivariable analysis results at HRH, 2018.
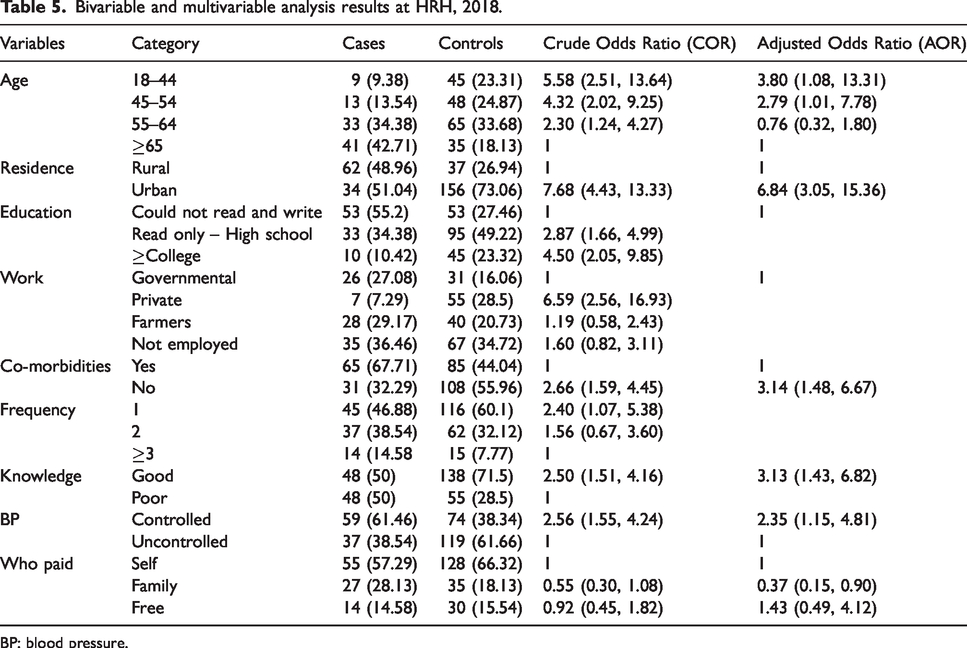
BP: blood pressure.
Discussion
Ensuring patients’ adherence to anti-HTN medications to prevent complications of HTN remains a major challenge to public health in many developing countries. Poor adherence to treatment is a reason for uncontrolled HTN, serious complications and wastage of healthcare resource.6,15 This study tried to identify factors associated with adherence to anti-hypertensive treatment.
The current study found that the majority of hypertensive patients had low levels of medication adherence in line with the local study conducted in referral hospitals of North West Ethiopia, 15 Adama 16 among patients with HTN. Various international studies in Malaysia (53.4%), 17 Egypt (74.1%) 18 and Uganda 19 have also documented similar poor adherence. The finding of the present study showed a lower percentage of adherence level than studies in Egypt (74.1%), 18 Pakistan (77%), 20 Sunderland (79%) 21 and the Western population (Scotland) reports (91%). 22 This might be due to better access and care to patients in these countries.
Patients' age was positively associated with the adherence score in other international studies.23–26 In this study, patients with age <44 years old were three times more likely adherent than elderly patients. According to some reports in line with this study, younger patients showed better adherence to pharmacological treatment, 27 while others stated that young age is a determinant of poorer adherence to hypertensive medication.12,25,26 Non-adherence in younger patients might be due to the lack of symptoms at early stages of the illness or more concerns about medication side effects.
In contrast, some researchers have also found better adherence among older patients, 23 in which patients in the age group of >40 but not > 60 and >65 were more adherent than younger age patients.23,24 The better adherence to treatment found in elderly patients has been explained by the presence of co-morbidities, which make the patients perceive themselves as very ill and take the prescribed treatment seriously, and elderly patients in the study area might have received better care by their caregivers.
In this study, a significant association was observed between patient residence and medication adherence. Hypertensive patients who lived in urban areas were six times more likely to adhere to their medications as compared to those who lived in rural areas. This is in line with a study conducted in Debre Tabor. 27 This might be due to the fact that rural residents lived too far away from the health facility and took more time reach the health facility for their medications. They might even forget to take their medication on time.
This study revealed that the presence of co-morbidities had significant impact on adherent behavior. Patients with no co-morbidities were more likely to adhere to their treatment than those with co-morbidities in line with a study done in North West Ethiopia. 28 However, a study done in Scotland showed no significant association between the number of co-morbidities and adherence. 29 The reason for this difference might be that co-morbidities in Scotland and Iran might be diagnosed early and treated well, but this might not be the practice in this study area.
Knowledge towards HTN and its treatment was found to be positively associated to the adherence behavior of patients. A similar study done in Gondar and Debre Tabor, Malaysia and China demonstrated that patients who had good knowledge of their diseases and treatment had a better adherence compared to those who do not.27,30 The possible justification might be that knowledge about HTN and its treatment creates a clear understanding and avoids confusion about the treatment and the disease.
Those with controlled BP were likely to be adherent and those adherents were also observed to have controlled HTN. This finding is in line with the study done in Gondar. 30 The reason might be the increase of patient satisfaction and creation of strong motivation towards the treatment secondary to the reported controlled BP.
Limitation of the study
As the study is institution based, participants might not be representative of the general population, and hence it might be difficult to generalize the findings to the population. Self-reporting was used as the only method of measuring adherence which could result in overestimation of adherence.
Conclusions
The rate of medication adherence was found to be low. Factors like age, residence, presence of co-morbidities, knowledge towards HTN and its treatment were seen to have an influence on the adherence behavior of patients. Therefore, patient support and management of comorbidities should be strengthened and provided to the hypertensive patients. In addition, health educational strategies that specially focus on medication adherence should be designed and provided to hypertensive patients and to the community in general.
Footnotes
Acknowledgements
The authors would like to express their heartfelt gratitude to data collectors who helped in data collection and also to the hypertensive clients who participated in the interview.
Availability of data and materials
The data are available in the public library of Debre Markos University in a form of graduate student thesis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
A formal ethical approval was obtained from Institutional Research Ethics Review Committee, College of Health Science, Debre Markos University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
YM.
Contributorship
AG designed and conducted all data collection procedures, analyzed and interpreted results. MT, AF and YM participated in proposal development and final paper write up. YM prepared the article. All authors read and approved the final version of the article.