
Abstract
Introduction
Efforts were made to improve management of coronary disease as the fast-track system to the Coronary Unit. We aim to analyse case-fatality rates by acute coronary syndrome in Portugal from 2000 to 2016, mainly the impact of the fast-track system and the proportion of patients that activate the fast-track system.
Methods
We analysed monthly acute coronary syndrome case-fatality before and after the implementation of the fast-track system in 2007. Impact of the system was assessed through regression models for interrupted time-series. We calculated annual proportion of fast-track system admissions.
Results
After 2007 case-fatality by acute coronary syndrome decreased (β=−1.27, p-value < 0.01). The estimates obtained for ST Elevation Myocardial Infarction suggest a reduction of nearly 86 monthly deaths prevented after 2007. The highest percentage of patients admitted through the fast-track system was 35%.
Conclusions
Our results suggest fast-track system may have contributed to a decline in acute coronary syndrome case-fatality. However, more than half of patients were not admitted through the system. This should encourage health authorities to make efforts to ensure compliance.
Introduction
Cardiovascular disease (CVD) is the leading cause of death in Europe and the most common cause of death in Portugal. 1 It is estimated that by 2030, ischaemic heart disease will be the third leading cause of death worldwide. 2 Despite recent decreases in mortality rates in many countries, CVD is still responsible for almost half of all deaths in Europe, 3 constituting a major public health challenge in Western Europe. 4
Although coronary heart disease (CHD) mortality rates have been declining since the 1980s in Portugal, more steeply after the mid-1990s, particularly among women 5 and across the EU, there is evidence of a consistent pattern of recent plateaus in CHD mortality rates. 6
The observed reduction in CDV mortality in the last decades, albeit at a low rate, is the result of a set of changes from efforts made by most European countries in disease prevention, tackling mainly risk factors, and of the improvements in disease management and treatment.
Particularly in Portugal, several improvements in CHD management have been made, with improvements in the availability of drug treatments and, more importantly, in the easiest and fastest access to reperfusion and revascularisation interventions. 6
The evidence-based effectiveness of the health policies is increasing, and we have realised that a variety of policy- and practice-related measures will be necessary to effectively reduce CVD prevalence and mortality as well as to promote changes in the healthcare system.
Thus, it is important to assess the relative contribution of these underlying factors to the observed decline in CHD mortality in different settings to develop future health policies.
In Portugal, several policies have been implemented that could impact mortality rates by acute coronary syndrome (ACS), from polices more focusing on disease prevention to policies more directly targeting mortality, such as the recent implementation of a fast-track system (FTS) with direct admission to the Coronary Care Unit (CCU). There is, therefore, a growing consensus about the unmet need for health policy impact analysis. 7
As time is crucial in ACS, time is muscle, it is essential to create measures that can help reducing the time to treatment, thus reducing mortality and morbidity associated with ACS.
Although the FTS was implemented in Portugal to reduce the time to CCU, recent studies have shown a small proportion of patients activating the system. Therefore, we analysed the impact of a FTS to CCU (via verde coronária in Portuguese) in case-fatality rates by ACS in Portugal from 2000 to 2016, even when a small proportion of patients activated the system.
Material and methods
Data
Data were obtained from the Diagnosis Related Group National Database, which collects data from all admissions into Portuguese public hospitals (Mainland Portugal), storing data on primary diagnosis and some demographic variables such as sex and age, as well as the geographic region of the admission. 8
Approval to access data was obtained previously from the Minister of Health Office and the Portuguese Society of Cardiology.
All admission cases from 2002 to 2016 were extracted, and only participants aged 20 and over, with primary diagnosis of ACS coded in ICD 9 (international classification of disease, 9th revision) as 410.00-410.xx to identify admission diagnosis of acute myocardial infarction (AMI) and 4130 codes, to identify unstable angina (UA), were analysed.
A second population dataset was used from the National Registry of Acute Coronary Syndrome (NRACS), 9 and for our study, we extracted all data from 2002 to 2015. This dataset was used to obtain the proportion of ACS patients that were admitted into the hospital through the FTS. This proportion was computed by using the total number of ST Elevation Myocardial Infarction (STEMI) patients in the denominator and the number of STEMI patients that activated the FTS system in the numerator. We focused on STEMI patients once the system was mainly directed to STEMI as these are frequently more symptomatic 10 and the fast track is a patient-initiated process, thus patients with Non-ST Elevation Myocardial Infarction (NSTEMI) might be less likely to activate the FTS.
This dataset has the advantage of being integrated into the Euro Heart Survey platform and, consequently, uses the Cardiology Audit and Registration Data Standards system, which ensures that credible and comparable information is collected in several European countries over time as they use standardised information, both in terms of the definition and coding of variables and in the form of data measurement and collection. As the data are validated and standardised, this allows for the possibility of applying and validating analyses in other larger populations, thus obtaining more robust results. 11
The FTS was implemented in all regions of Portugal in 2007, providing seven years of data before the implementation of the regulation (January 2000–December 2007) and nine years of data after the regulation was implemented (January 2008–December 2016).
The unit of analysis was monthly deaths by ACS.
Fast track to CCU
The FTS was implemented in Portugal with the goal of creating a priority system and facilitated access to clinical, therapeutic, and complementary diagnostic resources. Direct admission into the CCU is essential not only to improve accessibility, but also to allow a more effective treatment, since the time between the onset of symptoms and treatment is, in the case of AMI, vital for the reduction of morbidity and mortality.
The system is initiated by the patients when calling the emergency number (112). The National Institute of Medical Emergency (INEM) initiates the diagnosis and treatment earlier while referring the person to a hospital unit specialising in ACS treatment. 12
Once when the INEM is activated (by patients through the emergency number) they have the capacity to prematurely, as soon they are in contact with the patient, do an electrocardiogram, and along with the symptoms assessment make a diagnosis. If the diagnosis is established it is then decided, along with the Urgent Care Counselling Centre (CODU), on the pre-hospital treatment as well as on the referral to hospitals, increasing the likelihood of therapeutic success. The CODU contacts the nearest hospital unit with a catheterisation laboratory, in order to take the necessary steps for the expedited admission and treatment of the patient. 13 Once the CODU is contacted, the nearest catheterisation laboratory is prepared for the patients and a team of specialists are ready to receive them, thus the time from symptom onset to revascularisation is minimised.
The system was first implemented as a pilot project in the Algarve region of the country in 2002, but only by 2007, it was implemented as a policy throughout Mainland Portugal. 14
Statistical analysis
The main outcome in our study was monthly case-fatality rate, later stratified by age and sex, which were obtained using data from ACS patients admitted into public hospitals in the country. All missing data were removed from all the analysis.
The ACS case-fatality rate was computed for each month by using the total of patients admitted into public hospital as the denominator and the number of ACS deaths as the numerator.
The impact of the breakpoint estimated for the impact of the fast-track implementation on ACS case-fatality rate was assessed through multiple linear regression models, using standard methods for interrupted time-series.15,16 We included one dichotomous variable that accounted for the main effect on ACS case-fatality rate of the estimated breakpoint and an interaction between the breakpoint estimated and the time, to evaluate changes over time following the breakpoint.
The model was implemented to test whether there was a significant change in the number of ACS case-fatality rates and if the fast track had any impact.
A month indicator covariable was introduced to adjust for seasonality in the outcome admissions.
All analyses were stratified by demographic variables such as sex and age, and further stratified by type of AMI, i.e. STEMI versus NSTEMI, removing UA patients. Age was grouped into two categories, < 65 and ≥ 65 years old. Autocorrelation between month estimates was incorporated adequately into the model, with the presence of short-term autocorrelation, applying a first-order autoregressive – AR(1) – structure to the residuals.
As not all hospitals in mainland Portugal have the capacity to adopt the FTS because of a lack of human and technical resources, we also compared case fatality trends for hospitals with the FTS in place versus hospitals with no such system. Generalised least squares regression was applied, with a dichotomous variable distinguishing hospitals with the FTS from those without such a system and a month indicator to account for seasonal variations.
We also calculated the total time from symptom onset to first medical contact (FMC). The time was then analysed through a generalised linear model, assuming a linear behaviour of time, using as covariates a dichotomous variable before and after the fast-track implementation, demographic variables (sex and age) and risk factors (smoking, hypertension, diabetes, dyslipidaemia, obesity). The variable representing the use of the FTS was a ‘yes’ or ‘no’ categorical variable, which included fast-track admission versus self-transportation and non-medical ambulance.
Although we are aware that there might be differences in case-fatality rates according to the day of the week, weekend versus week day, we did not adjust for that in our models since there are studies pointing to a steady reduction in CVD for both weekends and weekdays. 17 There are also studies showing that after accounting for mode of arrival at hospital, there are no differences in case-fatality rates between weekdays or weekends. 18
Using data from the NRACS, we computed the monthly proportion of patients with ACS, namely STEMI diagnosis, that were admitted into the hospital through the FTS, divided by the total number of patients admitted into the hospitals.
Statistical significance was assessed through p-values, assuming < 5% as significant, and 95% confidence intervals were calculated for each of the regression coefficients.
Models were fitted in R version 2.3.2 software.
Results
A total of 20,849 in-hospital deaths by ACS were registered in the country (Mainland Portugal) from 2000 to 2016, out of a total of 203,040 ACS admissions.
We assessed monthly case-fatality rates by ACS for the period of 2000–2016, and our results show a decline in the number of registered deaths for the period studied. After the year of the implementation of the FTS in 2007, the year used as a breakpoint in the model created (Figure 1), there was a steep decrease in case-fatality rate, although there were no significant differences from the rate observed in the period before, thus the rate of the decline has remained steady throughout the last 15 years.

Longitudinal trends for case-fatality rate by ACS (percentage) from January 2000 to December 2016. The vertical line marks the year 2007 for the full implementation of the FTS in the entire country. ACS: acute coronary syndrome.
There was a significant change in level, i.e. a significant drop in ACS case-fatality rate (β = −1.268, p-value: <0.01) after the FTS implementation, representing an abrupt intervention effect. 15
Although the change in trend was not significant, i.e. there was not a significant decrease in the slope after the fast-track implementation, the fact that there was a significant change in level denotes a clear change in ACS case-fatality rate after 2007; on the other hand, it also points out to the fact that the rates after have remained fairly similar to the rates of decline observed before the FTS.
We stratified the ACS case-fatality rate by sex, and the trends observed for the pre-system implementation and the post-system implementation were similar for both men and women (Figure 2, Table 1). For both men and women, there was a steep decrease after the system was implemented; however, as for the overall rate, the decreasing trends remained fairly steady. Although the immediate decrease was similar for men and women, the reduction in ACS case-fatality rate was more marked in women (β = −1.45, p-value = 0.01) than in men (β = 1.06, p-value = 0.01) (Figure 2, Table 1).

Stratified longitudinal trends for case-fatality rate by ACS (percentage) from January 2000 to December 2016. The vertical line marks the year 2007 for the full implementation of the FTS in the entire country. (a) Longitudinal trends for males, (b) longitudinal trends for females, (c) longitudinal trends for patients under 65, and (d) longitudinal trends for patients over 65. AMI: acute myocardial infarction; NSTEMI: Non-ST Elevation Myocardial Infarction; STEMI: ST Elevation Myocardial Infarction.
Results of segmented linear regression analyses to detect association between fast-track system and monthly case-fatality rate ACS and multivariate regression analysis between time from symptom onset and several predictors.

ACS: acute coronary syndrome; AMI: acute myocardial infarction; CI: confidence interval; NSTEMI: Non-ST Elevation Myocardial Infarction; STEMI: ST Elevation Myocardial Infarction.
β represents the coefficients of the regression.
aAll regression models were adjusted for seasonal effects.
Interestingly, the results for age stratification showed that for people under 65, there was an increasing trend in case fatality (β = 0.01, p-value = 0.01), although the change in trend was significant, it was in fact a minor increase, less than 0.05%.
However, for patients aged 65 and over, the case fatality trend was also significant (β = 0.02, p-value = 0.02). For younger participants, although the increase trend was significant, it was a minor increase of less than 0.05%.
The seasonal pattern observed was consistent with that reported elsewhere, 19 with higher rates of admission over winter and lower rates during the summer.
In addition, when studying the further stratified results by STEMI versus NSTEMI and removing patients with UA (Figure 3), there was an immediate significant decrease for STEMI case-fatality rate (Table 1) in 2007; no significant changes in case fatality trends were observed for NSTEMI after 2007. The estimates obtained for STEMI case-fatality rate suggest a reduction of nearly 86 monthly deaths prevented after 2007 (Table 1).
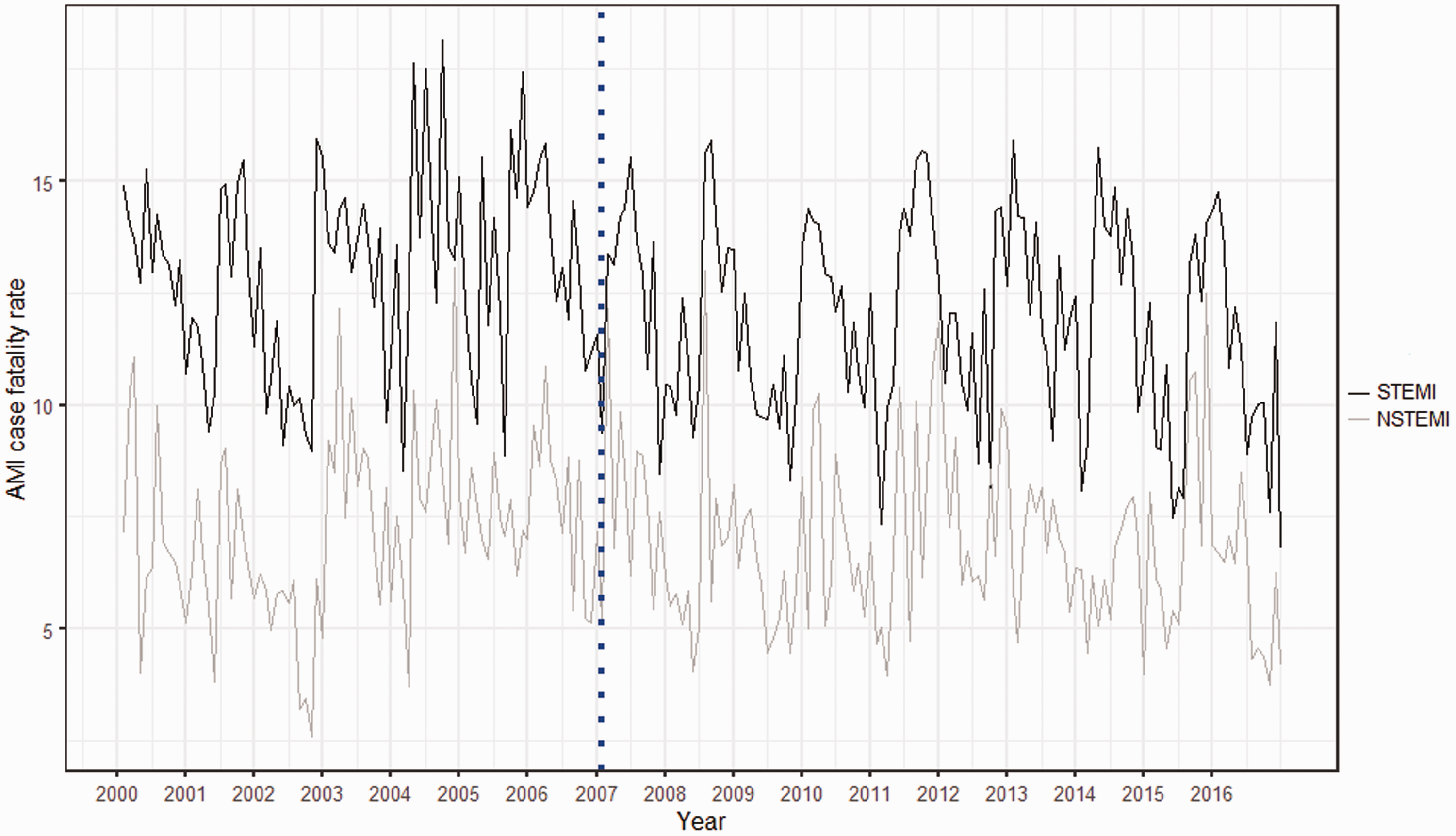
Longitudinal trends for case-fatality rate by ACS (percentage) from January 2000 to December 2016 for STEMI versus NSTEMI patients. The vertical line marks the year 2007 for the full implementation of the FTS in the entire country.
Analysis of the NRACS data allowed us to assess the actual proportion of patients that activated the FTS over time. Although the proportion of fast-track admission has been increasing over time it has only reached a maximum value of 38% in 2016, it has been a slow increase (Figure 4).

Percentage of annual STEMI patients admitted through the FTS.
Furthermore, we compared the ACS case-fatality rate between hospitals with a FTS implemented and hospitals with no such system, as a proxy to compare case-fatality rates, although we acknowledge the fact that hospitals with the FTS can still admit patients that reach the hospital by any other way of transportation. Our results indicate a significantly lower case-fatality rate for hospitals with the FTS implemented (β = −0.67, p-value < 0.01; Figure 5).

Comparison of longitudinal case fatality trends between hospitals with FTS versus hospitals without the FTS.
Mean time from symptom onset to FMC was also analysed. For patients admitted through the FTS, the mean time from symptom onset to FMC was 224.20 min, approximately 3 h, while for patients that were not admitted through this system, mean time from symptom onset to FMC was 354 min, approximately 6 h (Figure 6). When assessing the results from the multivariate regression (Table 1), time from symptom onset to FMC was significantly lower for participants admitted through the FTS, up to around 50 min less. Analysis of the demographics and risk factor covariates used in the model denoted that older people and women, as well as patients with diabetes and obesity, had longer delays. Surprisingly, smokers had lower times from symptom onset to FMC.

Time from symptom to FMC between patients that activated the FTS and patients who did not activate it. FMC: first medical contact.
Discussion
Trends in mortality by AMI have been decreasing steadily in Europe. In Portugal, mortality by ACS has been studied up to 2008 and showed around 3760 fewer deaths in 2008 compared to the expected number if the rates observed in 1995 had persisted. 5 More recently, a set of health policies tackling not only disease prevention, but also decrease in mortality, were implemented in the country, namely the FTS in 2007, the smoking ban in 2009, and a salt reduction regulation in mid-2010. Although in our study, we focused on the impact of the FTS on case-fatality rates, all these policies can affect CVD mortality.
Although CHD mortality rates in Portugal decreased by more than 25% between 1995 and 2008, we found a significant decrease immediately after the implementation of the FTS up to 2016. Although we cannot attribute this directly to the FTS, the reductions found up to 2008 were attributable to better care and treatments, explaining half of the overall decline in CHD deaths. Furthermore, by 2008, the fast-track system was already implemented, and also there was an increase in the number of centres with a catheterisation laboratory. Also, by 2008, approximately 42% of the decrease could be attributed to an improvement in major risk factors 5 ; therefore, regulations such as the smoking ban and mandatory salt reduction probably had a greater influence on mortality rates.
Our study also shows there was a steep decrease in case-fatality rate the year of the implementation of the fast track; however, the rate of decline observed after that was similar to the years previous to the policy. This is most likely to lower proportion of patients activating the system. On the other hand, there were no major changes in prescriptions for pharmacological treatments specifically for the year 2007 20 that could explain the decrease observed in case-fatality rate after this year.
The stratified results for STEMI versus NSTEMI showed that the significant decrease after 2007 was only observed for STEMI patients, this was expected as the FTS is focused mainly for these patients. The total prevented monthly deaths was around 86 deaths, although this number is not as high as other studied, namely a recent meta-analysis that showed reductions up to 30–40% in hospital mortality after the implementation of the FTS. 21 However, by 2016 only a total of 38% of the STEMI patients have activated the system, thus more than half of the patients are not beneficiating from the fast-track policy.
We found similar decreasing case-fatality rates for men and women, which has previously been observed in other studies where the rate of decrease in CHD mortality appeared to be stable across both sexes. 6
Surprisingly, our results for age stratification were not consistent with the overall case-fatality rate. Either for the youngest or older patients, we observed no immediate change in case-fatality rate after the FTS was implemented. For both groups, there were significant changes in trend; however, the trends observed were increasing. The prevalence of obesity and therefore diabetes 22 is in fact increasing in the country, which can be attenuating the reductions for the younger groups. This fact has also been observed in other studies6,23 where the increase of obesity led to lower decrements of mortality for the younger groups. A similar pattern was observed for the older group, which has already been found in other datasets and indicates that older persons benefit the least from the decline in CVD mortality. 23 Other studies have also reported a persistently high case-fatality rate among the elderly. 24
Furthermore, when we compared ACS case-fatality rates between hospitals with a FTS implemented and hospitals without such a system, the rates were significantly different, and lower case-fatality rates were observed for hospitals that had the FTS. Although the trends were decreasing for both groups, hospitals with versus hospitals without the system, the decrease was more accentuated in the group with the FTS. This kind of system allows earlier diagnosis and direct communication between the ambulance team and the CCU, bypassing the ER, thus minimising time to treatment, which leads to better prognosis and, consequently, less case-fatality rates.
Previous studies have shown that minimising time to treatment using the FTS can directly lead to diminished case-fatality rates.25,26
The observed mean time (3 h), even for patients admitted through the FTS, was longer than the recommended time, 27 which is 1.5–2 h after symptom onset.
These types of results have already been reported in other studies where the average delay time from symptom onset to FMC remained at around 2 h and did not decrease despite multiple public education campaigns. 28
A decrease of 50 min was observed for patients admitted through the FTS when compared to patients not admitted through this system, and similar reductions in time have been observed in other studies. 29
The variables affecting symptom onset to FMC were not surprising, as most were found in other studies and associated with longer delays.
Although there is clear evidence, in our study as well as in previous studies, of the effectiveness of a FTS, more than half of the patients are not using this system. As this is a patient-initiated process, even when proven to be the best way of admission if patients and the community at risk do not have either sufficient health literacy to acknowledge their symptoms or the process is not widespread enough, the impacts of these health policies will not reach full capacity.
Moreover, Portugal was one of the countries to participate in a global initiative that aims to improve the delivery of facilities by increasing timely access to primary percutaneous coronary intervention, thus reducing mortality and morbidity in STEMI patients. The project was responsible for the launch of a national public campaign to raise public awareness of the symptoms of MI, among other objectives.
The OCDE recently revealed that the use of primary PCI increased dramatically in countries that had been participating in the ‘Stent for Life’ initiative. In fact, one year after implementation of the initiative in Portugal, a positive impact was observed, with greater use of the 112 emergency call service and a smaller number of patients arriving by their own means at local hospitals without PCI facilities. 30 This suggests that health campaigns, such as the ‘stent for life’ campaign, can have an impact on the health community and the general community.
Limitations
Nonetheless, we recognise some limitations of the study. Like in any ecological study, it is not possible to directly prove the association between the implementation of the FTS and the reduction in case-fatality rate by ACS. In Portugal, considerable efforts have been made to improve patient care, thereby increasing patient awareness to symptoms and improving patient health. The implementation of a national smoking ban 31 and of a salt reduction regulation 32 might have affected the findings in our study, making this decrease in case-fatality rate a multifactor effect rather than a ‘one approach effect’. In addition, there are more factors, besides the public health campaigns mentioned above, that could impact case-fatality rates by ACS, such as novel pharmacological therapeutics, as well as change from a CK-based assay to a troponin assay, use of higher sensitivity troponin.
The fact that the decrease in case-fatality rate was observed right after 2007 supports our theory that FTS played a major role in this decrease, once the smoke ban and salt regulation were implemented after this year, also, pharmacological therapeutics have been steadily improving with no particular innovation in 2007 that helped justify the decrease in case-fatality rate by ACS.
In addition, we compared case-fatality rates between hospitals with a FTS and hospitals without such as system. Although we could not distinguish the patients admitted through this system, we found significant differences in case-fatality rates between hospitals with versus hospitals without this system.
One of the strengths of our study is the use of two well validated and standardised databases, allowing for an easy comparison with other international studies, mainly those developed in other European countries. As well as the availability of information on gender and age, this allowed us to assess the robustness of our findings among different subgroups. Also, the time-series method is preferred over the simpler pre- and post-proportion comparison method, because it does not take the pre-intervention trend into account and also allows to correct for autocorrelation. 33
Conclusions
Our study extends the existing literature on the patterns of ACS mortality over time and allows assessing whether the current strategies to reduce mortality by ACS, namely policy interventions, are successful. Furthermore, our study suggests that policies such as the FTS are related to a decline in ACS case fatality, supporting the importance of this policy type in achieving health gains.
Considering that CHD is the number one cause of death in the Western world and as such constitutes an immense public health problem, 34 even a small improvement in treatment and an increase in patient awareness can have important clinical, economic, and social gains. On the other hand, our study showed that although the proportion of patients activating the FTS is increasing, more than half of the patients are not using the system. This highlights the importance of continuous education to the general community in terms of guideline adherence, regarding the importance of rapid reperfusion therapy, which can directly affect case-fatality rates. Although it is a learning curve, since the FTS is a patient-initiated process and thus, although the system is available, not all patients resort to it, as more evidence arises for the effectiveness of this type of policy, more investment should be applied into the education of the population.
Our results encourage legislators and public health authorities to make efforts to ensure compliance with the FTS, leading to a patient’s timely access to treatment and allowing better prognosis, thus reducing mortality and morbidity by ACS.
Footnotes
Contributorship
DA – perfomed all statistical analysis and drafted the manuscript and is the guarantor of all data used.
CA and FP – reviwed and ammemened when necesary.
PS – Was responsible for giving inputs on the methoidological desing and revising the manuscript.
Acknowledgements
The authors thank the investigators of the NRACS, Sociedade Portuguesa de Cardiologia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The data used in the study were obtained with authorisation of the Portuguese Cardiology Society and the Directorate General of Health.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
DA.