
Abstract
Background
Catheter-directed thrombolysis may prevent post-thrombotic syndrome in patients with ilio-femoral deep venous thrombosis. We performed a retrospective review of prospectively collected follow-up data to evaluate the results of catheter-directed thrombolysis at our institution.
Method
Patients admitted for venous thrombolysis were included in the study and their files screened for information regarding results and technical aspects of treatment and patient status on follow-up. A catheter was inserted under imaging guidance into the thrombosed vein. Through the catheter tissue plasminogen activator was administered. Daily catheter-based venographies were performed to monitor progression in thrombus resolution. After thrombolysis flow-limiting stenosis was stented. Patients started wearing compression stockings and were started on oral anticoagulant therapy. Follow-up visits with ultrasound, magnetic resonance venography and clinical assessment were scheduled at six weeks and three, six, 12 and 24 months.
Results
A total of 48 patients underwent catheter-directed thrombolysis, including 36 female patients. Median age was 28 years. Complete lysis of the thrombus was achieved in 43 cases and partial lysis in two cases and 26 stents were placed. No deaths or life-threatening bleeding events occurred. Thirty-two of the patients who achieved full lysis and were followed up remained patent at follow-up. At 12 months seven patients had symptoms of post-thrombotic syndrome.
Conclusion
Catheter-directed thrombolysis represents a safe and effective alternative to systemic anticoagulative treatment of deep venous thrombosis with rapid resolution of the thrombus and few complications. Long-term patency shows good validity and this study suggests that catheter-directed thrombolysis is effective in preventing post-thrombotic syndrome.
Introduction
Acute deep venous thrombosis (DVT) of the lower limb, defined as DVT with symptom duration less than two weeks, is a condition that can result in severe morbidity and mortality. Treatment of DVT has traditionally been based on oral anticoagulant treatment, early ambulation and the use of compression stockings. Oral vitamin K antagonists prevent progression of the thrombus and protect against pulmonary embolism, further thromboembolic episodes, and death.1,2 However, they do not promote rapid dissolution of the clot. This depends solely on the endogenous fibrinolytic system. Thus, they do not offer full protection against the development of post-thrombotic syndrome (PTS) which is one of the primary long-term complications to DVT.3,4
PTS is associated with decreased quality of life for the patient and a great socio-economic burden for society. Around 20–50% of patients treated with recommended oral anticoagulants and compression stockings will develop PTS.5–7 The development of PTS is believed to be related to residual thrombus and valvular damage leading to venous dysfunction and venous hypertension resulting in oedema, pain, skin discoloration, ulceration and venous claudication of varying extent. 3 Rapid dissolution of the thrombus reduces and in some cases prevents permanent valvular damage, venous obstruction and prevents long-term morbidity. The greatest risk of PTS is seen in patients with DVT involving the common femoral and iliac vein.8,9
Catheter-directed thrombolysis (CDT) has been introduced as a treatment option for selected patients with no previous history of DVT and a low risk of bleeding complications.8,10 CDT offers rapid resolution of the clot and reduces the incidence of long-term complications as reported in several studies.11–13 Since 2011, Kolding Hospital has been referral centre for patients in need of CDT in the Western part of Denmark. The objective of this study was to investigate the course of treatment and the outcome with regards to patency at cessation of treatment and patency and incidence of complications including PTS at follow-up.
Method
Patients in this study were identified by searching through the electronic patient records at the Department of Radiology for the period of interest. All patients admitted for venous thrombolysis were included in the study. According to a predefined plan, patient files were screened for patient characteristics, course of treatment and follow-up period.
Before being admitted to the Department of Vascular Surgery for thrombolysis, patients were evaluated with regards to the inclusion and exclusion criteria listed in Table 1. If the patient was eligible for CDT the referring department was instructed to start treating the patient with daily subcutaneous injections of low molecular weight heparin until the morning when CDT was initiated. The degree of thrombosis was verified with ultrasound scan and magnetic resonance (MR) scan.
Inclusion and exclusion criteria.

DVT: deep venous thrombosis; INR: international normalized ratio.
A multi-side-hole catheter (Unifuse Infusion Catheter, Angiodynamics, Latham, USA, Fountain Infusion systems, Merit Medical Systems Inc., Utah, USA or EKOS, BTG IM, Surrey, UK) was inserted under ultrasound guidance through the popliteal vein into the thrombosed vein segment. Through the inserted catheter a solution with 0.4 mg/kg/day recombinant tissue plasminogen activator alteplase (Actilyse, Boehringer-Ingelheim, Ingelheim am Rhein, Germany) and 200 IE/kg/day dalteparin (Fragmin, Pfizer, New York, USA) dissolved in 750 ml 0.9% saline was administered at an infusion rate of 30 ml/h. If the patient had bilateral DVT, a catheter was inserted in each leg with half the dosage administered on each leg. A caval filter (Optease Vena Cava Filter, Cordis, Florida, USA or Celect Vena Cava Filter, Cook Medical, Indiana, USA) was inserted if the thrombus extended more than 1 cm into the inferior caval vein. The patient was monitored with blood tests daily. If the activated partial thromboplastin time > 100 s or fibrinogen < 1 infusion was paused and replaced by saline infusion with new blood tests after 3 h after which treatment was resumed if blood tests allowed it. Daily catheter-based venographies were performed to monitor progression in thrombus resolution. Patients were treated till complete lysis or no further progression on venography with maximum duration of 120 h. Partial resolution was defined as contrast deficiencies due to residual thrombus on venography, whereas a homogenous distribution of contrast in the vein was shown when the thrombus was totally resolved. Not dissolved thrombus was defined as no changes in thrombus extension on venography despite thrombolytic therapy. The caval filter was removed on final venography if there was no longer thrombosis involving the inferior caval vein. If residual thrombosis remained a CT phlebography was planned two weeks later to verify resolution of the thrombus and the caval filter was then removed.
After thrombolysis, the stenosis was stented (Luminexx stent, Bard Peripheral Vascular Inc., Arizona, USA or Zilver Vein, Cook Medical, Indiana, USA) if the operator judged it to be flow limiting based on contrast X-ray imaging performed from several projections. In two cases where the patients had residual thrombosis adjunctive treatment with AngioJet (AngioJet Peripheral Thrombectomy System, Boston Scientific, Massachusetts, USA) thrombectomy where the thrombus was actively aspirated was performed. The pharmacomechanical method with the Trellis catheter (Trellis Infusion System, Covidien, Dublin, Ireland) where the thrombus is dissolved with alteplase and a mechanical dispersion wire and later aspirated was used in one case.
At discharge, patients started wearing compression stockings on the affected limb and were started on oral anticoagulant therapy with either warfarin (Marevan, Takeda Pharma, Osaka, Japan) or rivaroxaban (Xarelto, Bayer, Leverkusen, Germany) with expected duration of treatment varying dependent on each patient’s individual risk of recurrent thromboembolic episodes. When determining this risk we took into account the patient’s thrombophilia status and whether the DVT was provoked or non-provoked.
Follow-up visits with duplex ultrasound scan and clinical assessment were scheduled at six weeks and three, six, 12 and 24 months. Relevant clinical findings concerning PTS were noted in the files without standardised scoring systems being used to determine the severity of PTS. Furthermore, MR venography was performed at six, 12 and 24 months.
Patients who did not participate in follow-up visits were contacted by phone to determine whether they displayed signs or symptoms of PTS or if they had been diagnosed with re-thrombosis in another clinic.
Prior to treatment, patients were informed about the treatment and risk of complications and received treatment if they consented to this. Experimental protocol and informed consent were not approved by the Institutional Review Board since this study is retrospective based on patient files hence treatment was not given as part of a study protocol. According to Danish rules and regulations patient consent to publication of medical data is not needed in such instances.
Results
During the period September 2011–December 2013 a total of 48 patients with 50 affected limbs underwent 50 procedures. The baseline characteristics of the study population, the treatment course and the technical aspects of procedures are listed in Tables 2 and 3.
Patient characteristics at baseline.

DVT: deep venous thrombosis; IVF: in vitro fertilisation.
aMedian with interquartile range.
bGirl diagnosed with multifocal astrocytoma at eight months. Latest follow-up two months before thrombolysis showed no tumour progression.
Course of treatment and technical characteristics of the procedures.
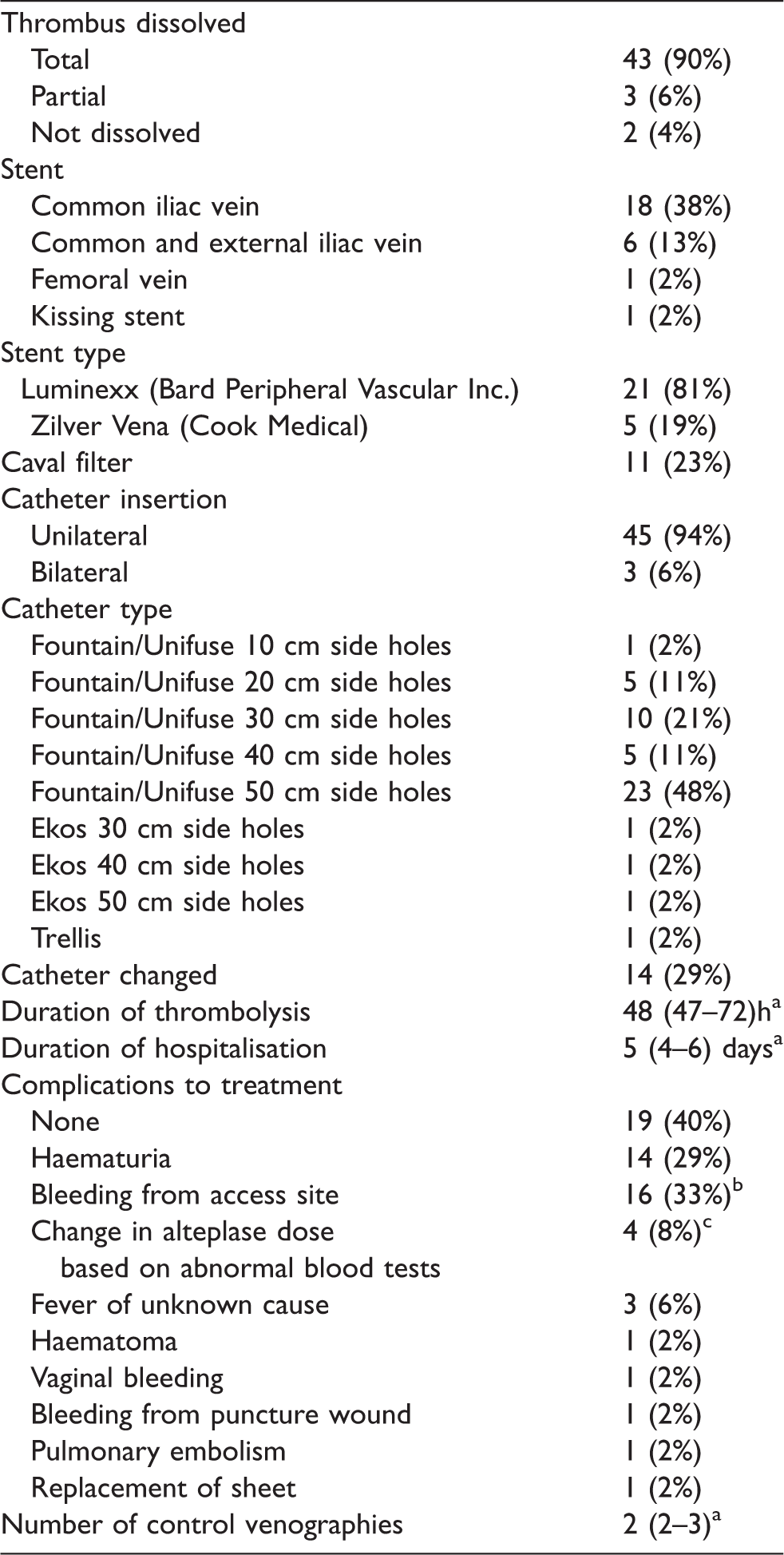
aMedian with interquartile range.
bFour did not result in change of alteplase dose.
cActivated partial thromboplastin time (APT)> 100 s or fibrinogen < 1.
Technical success
Complete lysis of the thrombus was achieved in 90% of the treated patients. The thrombus was partially dissolved in 6% and not dissolved in 4%. Treatment was stopped in one patient before complete lysis was achieved when she developed several bleeding complications with bleeding from the access site, vaginal bleeding and haematuria and was deemed unable to tolerate treatment. She developed further thrombosis after the treatment was stopped.
In another patient, treatment was stopped after five days when total lysis was not achieved. The patient had a chronically occluded caval vein and collateral veins.
Among the patients who did not achieve lysis of the thrombus, one patient was treated for five days with intermittent pauses in treatment due to bleeding from the access site and haematuria. After cessation of treatment, the patient developed further thrombosis despite oral anticoagulant treatment. In another patient treatment was stopped because the patient developed a puncture site haematoma on the side of the neck after insertion of a caval filter through the external jugular vein.
Complications
No deaths or life-threatening bleeding events occurred. There were no cases of septicaemia or other severe infections or infection of the access site. Among the three patients who developed fever two had elevated CRP and leucocytes and two received antibiotic treatment with good effect. The origin of infection was never identified. Patients were screened for urinary tract infection, pneumonia and infection of the access site. Both fever and elevated CRP and leucocytes can possibly be attributed to the inflammatory response initiated by the thrombus burden.
More than one complication was developed in 31% of the patients. In 4% of the patients complications led to cessation of treatment and in further 42% of the patients the complications resulted in reduced dosage or pause in treatment.
Patency and symptoms at follow-up
A total of 34 patients participated in the follow-up programme at one year. Another nine patients were contacted by telephone and five were lost to follow-up. Of the five patients lost to follow-up two were residents of the Faroe Islands. One patient did not show up for the scheduled controls and was therefore excluded from the programme. All five patients who were lost to follow-up had gained patency at discharge.
Patency was evaluated by MR venography or ultrasound scans in 33 patients, by clinical examination in three patients and by the patient’s own report in seven. Of the 38 patients in the follow-up group who had achieved full lysis of the clot, 33 remained patent at follow-up. Five patients re-thrombosed. One patient had bilateral DVT and re-thrombosed on her right side but eventually regained patency on oral anticoagulant therapy. The same patient developed a pulmonary embolism after discharge and developed swelling of her right leg at 24 moths. Another patient re-thrombosed the day after thrombolysis was terminated and started oral anticoagulant therapy. Of the patients contacted by telephone two re-thrombosed and no further information were available.
At one year follow-up one patient had developed partial thrombus of the infrarenal caval vein from a stent placed in the common iliac vein at initial treatment. The pelvic veins were patent and the patient was admitted for a second round of CDT and underwent treatment without complications.
The patient whose treatment was stopped due to several bleeding complications started oral anticoagulant therapy with warfarin and at six months follow-up the thrombosis had dissolved. However, the patient had PTS. At 12-month follow-up the two patients whose treatments were stopped after five days had developed total occlusion of the caval and iliac vein. Neither of them developed any symptoms of PTS. The patient who developed a haematoma of her neck was later readmitted and underwent a second round of thrombolysis which resulted in total lysis of the thrombus.
Complications reported at follow-up
Primary and assisted primary patencies are shown in Figure 1.
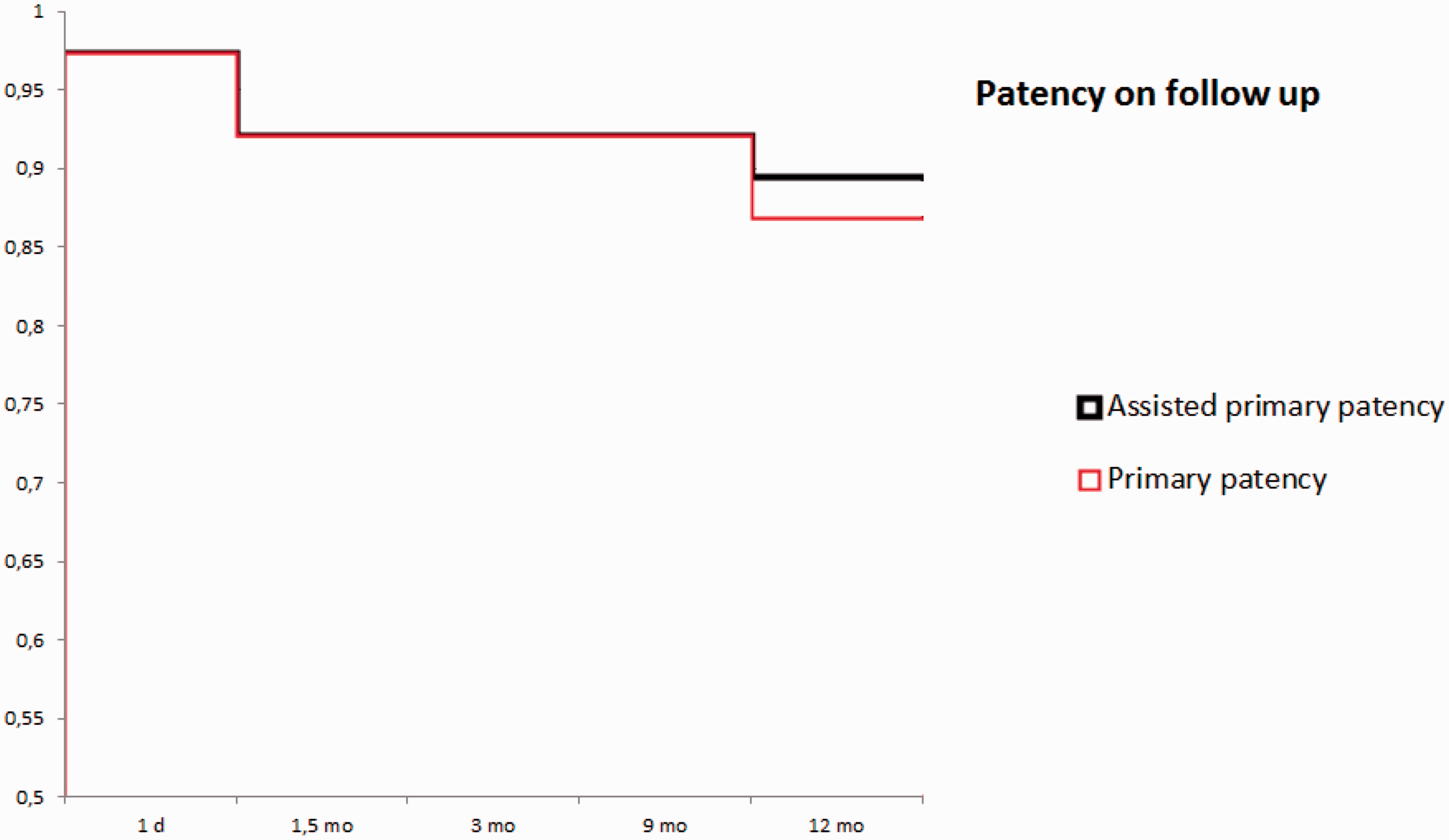
Kaplan–Meier curve showing primary and assisted primary patency at follow-up based on imaging with MR phlebography and ultrasound.
Two patients were referred to a vein clinic because of suspected PTS, one due to swelling of the leg and the other due to venous stasis, oedema and intermittent cyanosis of the leg, and a third patient was diagnosed with PTS at our institution. Another patient had persistent pain of her leg at 12-month follow-up which was deemed sequelae to the DVT although duplex ultrasound did not provide any explanation thereof. Furthermore, two patients complained about pain of the leg at one-year follow-up and two about oedema of the leg. A total of eight patients displayed symptoms of PTS.
Four months after initial thrombolysis one patient developed a thrombosis of the popliteal fossa which was more distally located than her initial DVT. This was despite oral anticoagulant therapy and no thrombophilia.
Pulmonary embolism was diagnosed in two patients shortly after initial discharge.
Discussion
The results of this study suggest that CDT is effective in treating acute ilio-femoral DVT with patency at 90% at the cessation of treatment. Furthermore, it suggests that CDT is a safe treatment option with only minor, non-life-threatening complications in this selected population. Long-term patency shows good validity and only few complications were reported on follow-up. When comparing with previously reported incidences of PTS in patients treated with anticoagulation and compression stockings alone this study further suggests that CDT is effective in preventing PTS. Incidence of PTS varies between 20 and 50%,5–7 when patients are treated with oral anticoagulation and compression stockings, which is a considerably higher incidence than reported in the present study.
The majority of our patients were treated with warfarin as anticoagulant therapy after discharge. Newer oral anticoagulants are thus far not used as standard therapy in our setting as seen in Table 4. Patients were screened for thrombophilia and they displayed a range of different abnormalities as listed in Table 5.
Anticoagulant therapy at follow-up.

Thrombophilia in the study population.

The success rate with regard to both short- and long-term patency corresponds with that reported by Bækgaard et al. 14 in their study of patients undergoing CDT at the hospital in Gentofte, Denmark. Enden et al. 15 in their two-year follow-up data from the CaVenT study reported total or partial lysis of the thrombus in 88.8% of patients which is comparable to the present results and with results reported by Bækgaard et al.
However, in the CaVenT study, a disappointingly high incidence of PTS of 37 (41.1%) of the patients undergoing CDT was found at 24 months compared to 55 (55.6%) of patients undergoing standard treatment with anticoagulation and compression stockings. The five-year follow-up data from the CaVenT study 16 show an overall 28% risk reduction on the development of PTS. Between the two- and five-year follow-up the incidence of PTS in the CDT group did not increase as opposed to the control group where it rose to 63 (70.8%) thus showing a persistent effect of CDT.
Bækgaard et al. reported that no skin changes, venous ulceration or claudication were seen in patients who had patent veins with normal valve function at follow-up. A total of 15 (14.9%) patients had slight oedema, reflux of the superficial veins or a slight feeling of heaviness in the affected limb. Status concerning symptoms of PTS among the patients with non-patent veins was not reported. The fact that symptoms of PTS were only recorded in eight (17%) patients out of 43 also suggests a considerably higher success rate in the present study than the one reported in the CaVenT study. The large difference between, on one hand the data from Gentofte and the present study, and, on the other hand, the CaVenT study, merits further discussion.
Patients enrolled in the CaVenT study were older with a mean age of 53.3 years (SD 15.7) and a larger percentage was men (74%). Patients with symptom duration up to 21 days were enrolled in the study, but the mean duration of symptoms in enrolled patients was merely 6.4 days (SD 4.4). Patients in the Gentofte study were similar to patients in the present study with regard to age and gender. No clear association between gender and age and the development of PTS has been described17–20 so this does not offer an immediate explanation of the observed differences although any association cannot be ruled out.
The CaVenT study also differs from the Gentofte study and the present study in their use of stenting with stenting being performed in 16.6% of patients compared to 56.6 and 54%, respectively. Treatment of underlying vascular abnormalities with stenting seems to be of importance for the long-term patency and thereby the development of PTS.8,21,22 This might partly explain the differences observed in long-term patency between these studies.
The preliminary results from the ATTRACT study show no preventive effect of CDT on the development of PTS. 23 These results might be due to the fact that not only patients with ilio-femoral DVT but also patients with more distally located DVT were included in the study. However, they also show that CDT seems to reduce the severity of symptoms of PTS still making it a relevant treatment option for ilio-femoral DVT. The final results are still pending and nothing certain is yet to be concluded.
In the present study each patient underwent daily venography at the Department of Radiology and required a median of three invasive procedures during their hospitalisation. Thus, CDT is an expensive and highly resource demanding treatment. Calculations to determine the cost-effectiveness of CDT have not been undertaken in this study. Taking into consideration that PTS is a severe condition with grave consequences for the patient and that the patients treated were fairly young it seems likely that in the long term cost-effectiveness is reasonable. The impairment of quality of life in patients with PTS parallels the quality of life in patients suffering from chronic obstructive pulmonary disease or severe heart disease.24,25 The patients have a relatively long life expectancy and preventing the development of chronic disease early in life will be of great importance for the patient and spare society a year-long socio-economic burden.
Limitations to study
The data for this study were collected retrospectively and thus has some short comings when it comes to follow-up visits. Not all patient files contained information about anticoagulant therapy or use of compression stockings. Furthermore, patients were not screened for PTS at follow-up according to a standardised scoring system such as the Villalta scoring system making it difficult to report on the severity of the symptoms they displayed. No information was available about the number of or characteristics of the patients who were referred for thrombolysis but were not treated because they met exclusion criteria. We did not have a matched cohort with patients receiving standard therapy with anticoagulants and compression stockings and are therefore not able to make any statistical comparisons between two groups.
Patients were treated for a median time of 48 h. This, however, includes the time where dosage of alteplase was reduced or treatment was paused due to complications and does therefore not represent the effective thrombolysis time. The amount of alteplase used during treatment has not been registered in the patient files and are therefore not reported.
Conclusion
In conclusion the current results add to the growing evidence that CDT is effective in treating ilio-femoral DVT and in preventing PTS in selected populations with DVT and a low risk of bleeding complications. Furthermore, only minor non-life-threatening complications were reported making it a safe treatment option.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study because the study is a descriptive and retrospective study based on patient files hence treatment was not given as part of a study protocol. According to Danish rules and regulations ethics approval is not needed in such instances.
Informed consent
Informed consent was not sought for the present study because the study is a descriptive and retrospective study based on patient files hence treatment was not given as part of a study protocol. According to Danish rules and regulations patient consent to publication of medical data is not needed in such instances. Prior to treatment, patients were informed about the treatment and risk of complications and received treatment if they consented to this.
Guarantor
Christina Pilgaard Madsen.
Contributorship
All authors were involved in study design. CM collected the data and drafted the manuscript. All authors revised the manuscript critically and approved the final manuscript.