
Abstract
Objective
We aimed to estimate the level of physical activity undertaken by health care professionals and the proportion that achieved a daily target of 10,000 steps.
Design
This was a prospective cohort study.
Setting
Participants were recruited in Wellington Regional Hospital, a tertiary hospital in New Zealand.
Participants
Neurology, Cardiology, and Endocrinology staff were invited to participate.
Main outcome measures
Pedometer-measured step counts were recorded over seven days and the proportion that achieved a daily target of 10,000 steps was calculated.
Results
We included 50 staff in the study. The mean daily step count was 10,620 (standard deviation = 3141) with a median daily step count of 10,606 (interquartile range = 7791–12,469). Sixty-five per cent of the staff achieved 10,000 steps per day.
Conclusion
This cohort was more active compared to other pedometer-based studies in health care professionals. The daily target of 10,000 steps per day was achieved at a higher proportion than reported in international studies and the general New Zealand.
Introduction
Physical inactivity is associated with coronary heart disease, hypertension, obesity, diabetes, and malignancies. 1 The New Zealand (NZ) Ministry of Health, consistent with the recommendations of international organisations, recommends individuals perform a minimum of 150 min of moderate aerobic activity, or 60 min of vigorous aerobic activity, per week. 2 This level of physical activity is equivalent to 10,000 daily steps,3–5 and this activity level reduces blood pressure and weight.6,7 Other health benefits of physical activity include a reduction in the rate of type 2 diabetes, cardiovascular disease, anxiety, depression, and osteoporosis. A 25% decrease in physical inactivity could prevent over 1.3 million deaths per year worldwide. 1 Health care professionals can play an important role in promoting physical activity for local communities, and the levels of physical activity undertaken by health care professionals are associated with their counselling behaviour.8,9 However, little is known about the level of physical activity of health care professionals in NZ.
The aim of this prospective cohort study was to estimate the level of physical activity undertaken by health care professionals and the proportion of health care professionals that achieved a daily target of 10,000 steps. We wished to focus on health care professionals working in clinical areas where primary and secondary prevention of vascular events were a significant clinical issue (i.e. areas where they were likely to be involved in giving advice about physical activity).
Materials and methods
The setting for the study was a 400-bed tertiary hospital in Wellington, NZ. All staff working in Neurology, Cardiology, and Endocrinology Departments were invited to participate through emails and presentations at staff meetings. The number of potentially eligible staff was approximately 220. Basic data collected by questionnaire included age, sex, height, weight, smoking status, occupation, and specialty group. Participants were also asked whether they exercised regularly, defined as a minimum of 150 min of moderate aerobic activity, or 60 min of vigorous aerobic activity, per week. Activity was measured using Omron HJ-203 pedometer (Omron Electronics Ltd, Auckland NZ), which participants were asked to wear around the neck attached to a lanyard, or clip it to their pants pocket, for seven consecutive days while awake, and to avoid activities that involved water. Pedometer readings were not concealed from the participants. The seven-day period was chosen to incorporate weekdays and weekends. After seven days, daily step counts were recorded for analysis. The pedometer counted and recorded daily steps for seven days automatically without participant input and with no ability for the participant to manipulate the step count.
The primary outcome variable was the proportion of health care professionals that achieved an average pedometer-measured step target of 10,000 steps over the duration of wearing the pedometer. Secondary outcomes were the number of steps, and whether these were associated with age, sex, occupational group or specialty, body mass index (BMI), smoking status, or self-reported exercise status before the study. The study aimed to achieve a sample size of 50 participants to give a 95% confidence interval for a proportion of plus or minus 15%.
The confidence interval for the estimate of the proportion of participants that achieved an average of 10,000 steps was by the Clopper–Pearson method. The secondary associations were assessed using a mixed linear model to account for repeated measurements on the same individuals with the number of steps as the response variable.
SAS version 9.4 was used.
The study protocol was assessed by the Capital and Coast District Health Board Research Office as meeting the criteria for expedited review of an observational study. A formal ethical review was not deemed necessary as it was considered outside the scope of the Health and Disability Ethics Committee. This study complied with the guidelines of the New Zealand National Ethics Advisory Committee including provision of written information and informed consent.
Results
Between September and December 2015, a total of 50 participants were recruited; however, one participant lost the pedometer and so 49 participants had pedometer data. The participants are described in Table 1.
Participant description.

BMI: body mass index; IQR: interquartile range; Max: maximum; Min: minimum; SD: standard deviation.
Unless stated.
A description of the pedometer data is shown in Table 2. One participant completed five rather than seven days of measurement.
Description of pedometer data.
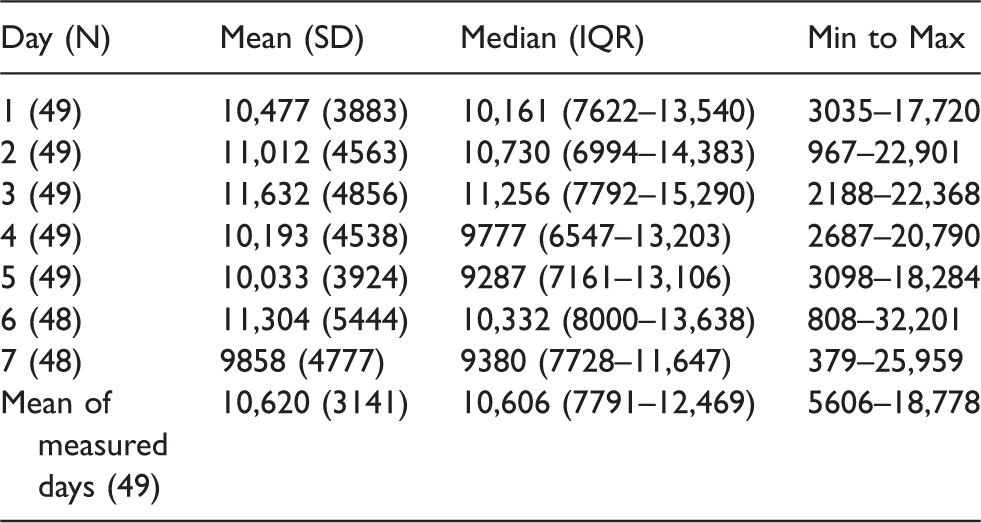
IQR: interquartile range; Max: maximum; Min: minimum; SD: standard deviation.
The proportion of participants who had an average of 10,000 steps a day was 32/49 (65.3%) with an exact 95% confidence interval of 50.4–78.3%. There was no evidence that the number of steps was associated with age, sex, occupational group or specialty, or BMI (P > 0.35 for all, details not shown). Self-reported regular exercise was associated with the average number of steps taken. The mean (SD) steps for participants reporting regular exercise (N = 31) was 11,645 (2930) and for those not reporting regular exercise (N = 18), 8827 (2727). Based on the full mixed linear model, the estimated difference (95% confidence interval) between those who exercised and not was 2833 (1136–4529), p = 0.002. In all 25/31 (81%) of those who self-reported, regular exercise achieved over an average of 10,000 steps in the week of measurement.
Discussion
Our study found that two-thirds of participants achieved the 10,000 daily step target on average during the week of measurement and about 80% of those who self-reported regular exercise were achieving this target. This cohort was more active compared to other pedometer-based studies in health care professionals. Rye et al. 10 measured mean daily step count in 55 medical residents and 62 medical students at work and leisure over three days and reported that only 35% of residents and 52% of students achieved the 10,000 daily target. Owoeye et al. 11 reported that only 20% of 180 health care professionals met the target. Other studies measuring step counts during work hours in anaesthetists, 12 emergency medicine residents, 13 cardiovascular specialists, 14 internalists, and general surgeons 15 found that none of these groups achieved an average step count at work of over 10,000. Some studies have identified obstacles to exercising for health care professionals including fatigue, lack of time, and family commitments. 12 This cohort was also more active compared to the general NZ population. The NZ Health Survey 2013/2014 reports that 51% adults were physically active for more than 150 min/week. 16
We did not find any association between daily step count and other measured variables. Rye et al. reported a modest negative correlation between mean daily step count and BMI. They also found that step counts tended to decrease as medical residents became more senior. 10 Owoeye et al. 11 and Goosen et al. 15 reported that step counts of health care professionals negatively associated with increased age, BMI, and body fat percentage. In the NZ general population, men (55%) were more likely to achieve physical activity recommendations than women (48%). 16
Limitations of this study were that participation was voluntary and those who were more interested in exercise may have participated which could bias the results in favour of activity. The sample size was modest so that for the secondary analyses, we likely lacked statistical power to detect associations seen in other studies. While pedometers are well validated for use in research to measure physical activity 17 and are accurate with ambulatory activity, they are less sensitive to other activities such as cycling and weightlifting. 18 Therefore, this study may have underestimated actual activity levels as some participants also partook in these activities. Based on results from other studies,8,9 physically active health care professionals were more likely to address inactivity with their patients so it seemed likely that, as many of the participants in this cohort were active, they were more likely to counsel activity. Only one participant reported tobacco smoking.
Our study highlighted that using pedometers to measure physical activity was feasible and inexpensive. For this study, the study researcher was able to complete data collection from 50 participants in less than 12 weeks whilst working full-time as a resident medical officer without explicit extra funding and with only 10 available pedometers.
Pedometers can act as an environmental cue and feedback tool. Wearing a pedometer could raise health consciousness and focus the attention of staff members on their own activity levels. This may make them more knowledgeable about activity level prescription including the use of pedometers. A NZ-based randomised controlled trial of 330 low-active adults aged 65 and above reported that pedometer use resulted in greater increase in leisure walking compared to standard time-based physical activity prescription. 19 A systematic review of 26 studies also found that pedometer users increased their physical activity by 26.9% over baseline. 20
Conclusion
The mean daily step count of health care professionals in a tertiary hospital in NZ was 10,620 and 65% of the health care professionals achieved the minimum recommended level of physical activity. This was a higher proportion than reported in international studies and the general NZ.
Footnotes
Acknowledgements
We are grateful to all the staff who had voluntarily accepted to take part in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
None.
Guarantor
LC was the guarantor for this study.
Contributorship
LC and HM were responsible for the study design and data collection. MW assisted with data analysis. LC drafted the manuscript, which was revised by HM and MW. All authors approved the final version of the manuscript.