
Abstract
Objective
To assess the effect of renal denervation (RDT) on micro- and macro-vascular function in patients with heart failure with preserved ejection fraction (HFpEF).
Design
A prospective, randomised, open-controlled trial with blinded end-point analysis.
Setting
A single-centre London teaching hospital.
Participants
Twenty-five patients with HFpEF who were recruited into the RDT-PEF trial.
Main outcome measures
Macro-vascular: 24-h ambulatory pulse pressure, aorta distensibilty (from cardiac magnetic resonance imaging (CMR), aorta pulse wave velocity (CMR), augmentation index (peripheral tonometry) and renal artery blood flow indices (renal MR). Micro-vascular: endothelial function (peripheral tonometry) and urine microalbuminuria.
Results
At baseline, 15 patients were normotensive, 9 were hypertensive and 1 was hypotensive. RDT did not lower any of the blood pressure indices. Though there was evidence of abnormal vascular function at rest, RDT did not affect these at 3 or 12 months follow-up.
Conclusions
RDT did not improve markers of macro- and micro-vascular function.
Keywords
Introduction
Heart failure with preserved ejection fraction (HFpEF) is a prevalent phenotype of heart failure for which no treatment has, as yet, been shown to improve prognosis. 1 Its underlying pathophysiology is multifactorial. Abnormal micro- and macro-vascular function have been observed in HFpEF and their presence is associated with increased cardiovascular events 2 as well as exercise intolerance.2,3
The sympathetic nervous system (SNS) is a modulator of arterial function. 4 Renal denervation (RDT) is a novel technique that has been shown to reduce central sympathetic outflow and hence may promote vascular remodelling. 5 The Renal DenervaTion in heart failure with Preserved Ejection Fraction (RDT-PEF) was conducted to investigate the effect of RDT upon symptoms, exercise function, left ventricular filling and cardiac remodelling in patients with HFpEF. 6 A vascular function substudy involving the same participants of the parent trial was prospectively designed to test the hypothesis that the vasculature might be a therapeutic target in HFpEF.
Methods
Trial design
The RDT-PEF trial was an investigator initiated, randomised, controlled, open-label trial with blinded endpoint analysis. 6 The primary endpoints of this study were symptomatic improvement (Minnesota Living with Heart Failure Questionnaire-MLWHFQ), exercise performance (peak oxygen uptake on exercise-peak VO2), B-type natriuretic peptide levels (BNP), left ventricular filling pressures assessed by E/e’ on echocardiogram, indexed left atrial volume (LAVi) on cardiac magnetic resonance (CMR) and indexed left ventricular mass index (LVMi). The rationale, design and results of the RDT-PEF trial have been published. 6
This vascular substudy was prospectively designed and received approval from the National Research Ethics Service (12/LO/1941). All patients gave informed consent to participate in the study.
Patients
Eligible patients were 18–85 years of age and were New York Heart Association class II/III. The recruited patients fulfilled the European Society of Cardiology Heart Failure 1 diagnostic guidelines for HFpEF and had either left ventricular hypertrophy or left atrial dilatation and either a raised natriuretic peptide level or tissue Doppler echocardiographic evidence of raised filling pressures. 6 Detailed criteria have been published. 6 Importantly, patients with atrial fibrillation were not excluded.
Study protocol
At the initial visit, all patients underwent 24-h ambulatory blood pressure monitoring (24-h ABPM), CMR to derive aortic distensibility and pulse wave velocity, digital tonometry to assess endothelial function and augmentation index (AI), renal magnetic resonance (MR) to calculate renal artery flow, resistive index and pulsatility index and finally a urine assay for albuminuria. The protocol was then repeated after 3 and 12 months (renal MR was repeated at 12 months only) following either renal denervation or on-going medical therapy. Assessments were performed blinded to allocation.
Renal denervation
Access to the renal artery was obtained via the femoral artery using an 80 cm 6 Fr guide catheter (RDC or IMA curve). The Symplicity™ single-electrode catheter was then advanced and positioned in the most distal aspect of the renal artery proximal to bifurcations, good vessel wall contact was obtained by deflecting the electrode tip and confirmed by an impedance of 250–300 Ω on the power generator. We then applied a minimum of four ablations to each main renal artery in a circumferential distribution as has been described elsewhere.6–8
24-h Ambulatory blood pressure monitor
A Spacelabs 90207 ambulatory blood pressure monitor was attached using an appropriately sized cuff to the non-dominant arm of the patient. It was attached for a period of 24 h and was analysed using automated and proprietary software. Twenty-four hour, day time (0800–2200) and night time (2200–0800) averages of blood pressure were obtained.
Aortic distensibility
This was derived from a MR axial dataset of the aorta at the level of the bifurcation of the main pulmonary artery. The maximum and minimal cross sectional areas of the ascending and descending aorta were calculated using Art-FUN (Laboratoire d’Imagerie Biomédicale, UPMC-CNRS-INSERM, France), an automated edge-detection software for assessment of arterial function. 9 Aortic strain was defined as: (max cross-sectional aorta area − min cross-sectional aorta area)/min cross-section aortic area. 10 Aortic distensibility (10−3 mmHg−1) was defined as: aortic strain/brachial artery pulse pressure. 10
Pulse wave velocity
Velocity encoded phase contrast sequences were acquired from a MR axial dataset of the aorta at the level of the bifurcation of the main pulmonary artery perpendicularly transecting both the ascending and descending aorta. A non-breath-hold sequence was used and 128 phases were captured during the cardiac cycle. The transit time of the propagation of the velocity waveform was calculated between the ascending and descending aorta using the Art-FUN software with the least squares minimisation approach using all data points on the systolic upslope of the aorta flows after peak flow normalisation.9,10 The aortic path length was calculated from the double-oblique view of the thoracic aorta. Pulse wave velocity (m/s) was derived as aortic path length divided by the transit time.
Endothelial function
This was assessed using the EndoPAT™ 2000 device (Itamar Medical, Israel). It recorded the arterial waveform at the fingertip (one probe on each arm). A rapid cuff inflator (E20, Hokanson, USA) was placed on upper right arm of each patient and set to inflate to a pressure of 200 mmHg or 50 mmHg above the patient’s systolic pressure (whichever was greater). A 6-min rest period was recorded, followed by 5 min when the cuff was inflated to occlude the right brachial artery, and finally 5 min of recovery with the cuff deflated (hyperaemic period). The proprietary software calculated the reactive hyperaemia index (RHI) and AI based upon these readings. AI was calculated as the difference between the second and first systolic peak of a pressure waveform expressed as a percentage of the pulse pressure.
Renal blood flow
Images were acquired using the Siemens Skyra (3.0 Tesla) MR scanner. Renal artery blood flow was assessed by applying a bespoke breath-hold spiral phase contrast sequence on a through-plane image of the proximal renal artery. 11 In patients with sinus rhythm retrospective cardiac gating was used to acquire data throughout the entire cardiac cycle while for patients with atrial fibrillation, prospective cardiac gating was used with imaging over approximately 2/3 of the cardiac cycle. Scan parameters were replicated for follow-up scans on an individual patient basis. 11 Resistive index was calculated as (peak systolic velocity − minimum systolic velocity)/peak systolic velocity. 11 Pulsatility index was calculated as (peak systolic velocity − minimum systolic velocity)/mean velocity. 11
For the majority of these variables, normal cut-off values have not been derived. Abnormal vascular function is associated with an increased pulse pressure, pulse wave velocity, AI, resistive index, pulsatility index, albuminuria and a decreased aortic distensibility and RHI.
Statistics
Data were assessed for normality both subjectively using histograms and statistically using the Shapiro–Wilk test. Parametric data are presented as mean ± standard deviation; between group comparisons were performed using the independent samples t-test and within group comparisons using the paired t-test. Non-parametric data are presented as median with interquartile range; between group comparisons were performed using the Mann–Whitney U test and within group comparisons using the paired Wilcoxon-signed rank. Correlation between the vascular parameters, the primary endpoints 6 and the safety endpoint of estimated glomerular filtration rate (eGFR) 6 was assessed using Spearman’s rho. P < 0.05 was used as the threshold for statistical significance and a P < 0.01 was used for the multiple correlation assessments. A prospective power calculation was not performed as this was a sub-study.
Result
Recruited patients
Baseline characteristics of the RDT-PEF population.

Data are presented as mean ± standard deviation or count (%).
BMI: body mass index; CVA: cerebrovascular accident; CHD: coronary heart disease; AF: atrial fibrillation; NYHA: New York Heart Association; A: ambulatory; SBP: systolic blood pressure; ACEi: angiotensin converting enzyme inhibitor; ARB: angiotensin receptor blocker; CC: calcium channel.
Ambulatory blood pressure monitoring
Change of average systolic (SBP) and diastolic (DBP) blood pressure in mmHg within the RDT-PEF trial at 3 and 12 months follow-up.
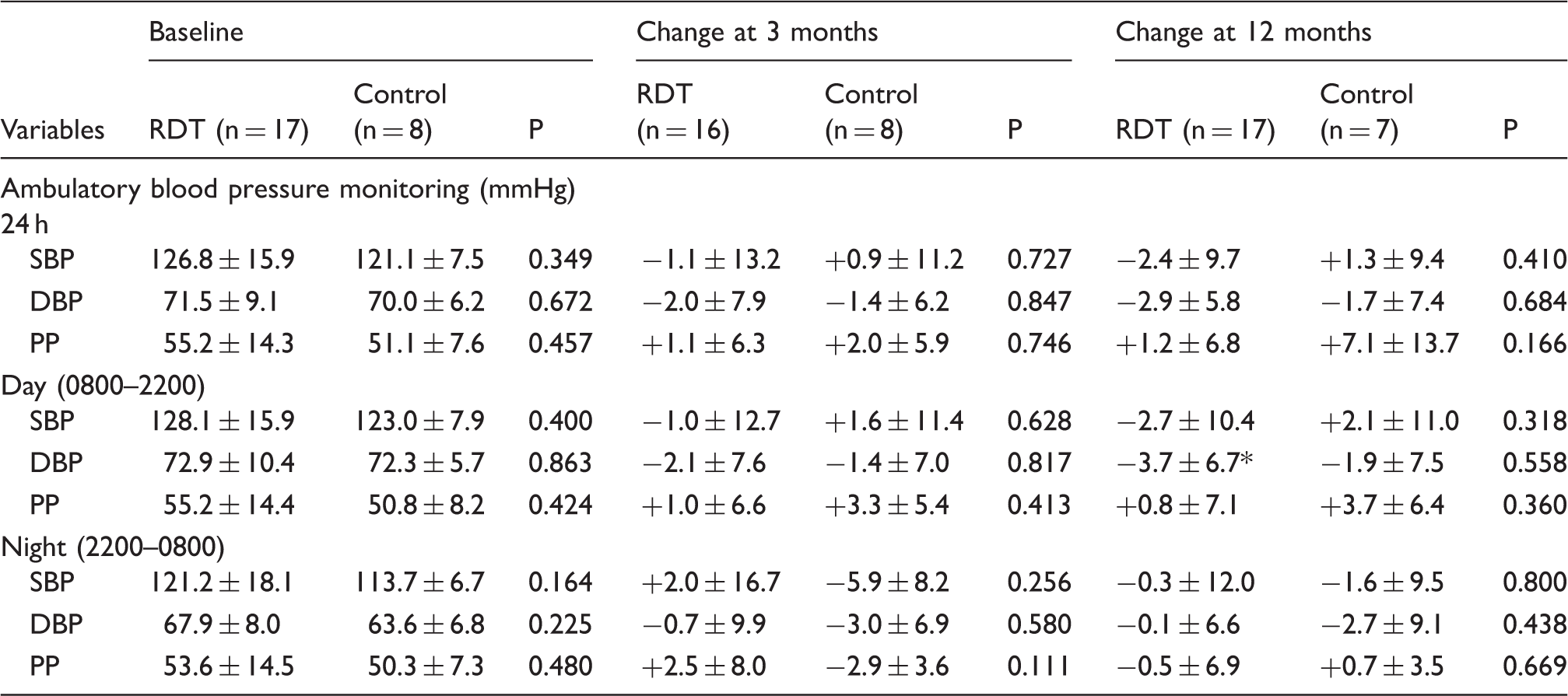
P < 0.05 for within group change.
Aorta function and endothelial function
Macro- and micro-vascular function.

AA: ascending aorta; DA: descending aorta; AI: augmentation index; LnRHI: natural log of reactive hyperaemic index; ACR: albumin:creatinine; disten.: distensibility.
P < 0.05 (for within group change).
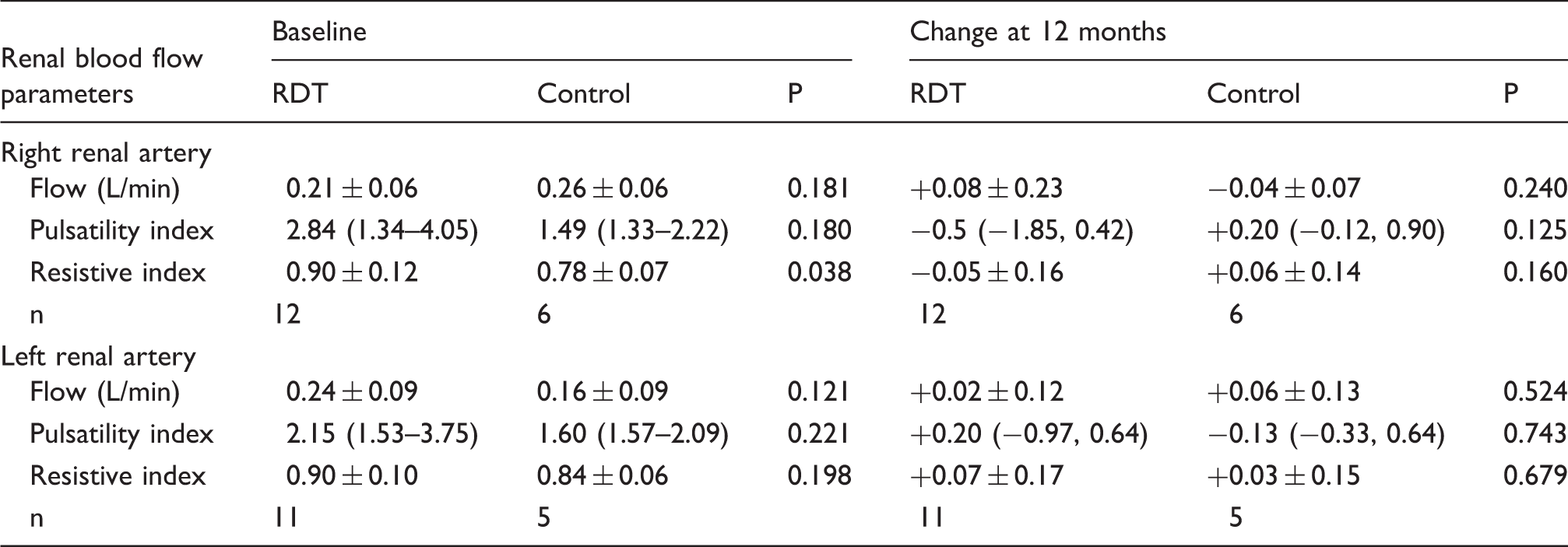
Renal blood flow
Renal magnetic resonance derived markers of blood flow.
Effects of age on vascular function
There was a trend for age to be associated with baseline ascending aorta strain (rho = −0.46, P = 0.02) and distensibility (rho = −0.42, P = 0.04) as well as descending aorta strain (rho = −0.45, P = 0.03). No correlations were seen with any of the other parameters.
Correlations between baseline vascular function and primary endpoints and eGFR
Spearman’s correlation between baseline vascular function and baseline primary efficacy endpoints and estimated glomerular filtration rate (eGFR).

The numbers in bold are the values that reached statistical significance. AA: ascending aorta; DA: descending aorta; AI: augmentation index; LnRHI: natural log of reactive hyperaemic index; UACR: urine albumin:creatinine; RBF: renal blood flow; PI: pulsatility index; RI: resistive index.
Discussion
The main finding of this body of work is that RDT did not improve vascular function in patients with HFpEF. It is therefore important to review: (a) the evidence supporting the initial hypothesis that vascular dysfunction plays an important role in HFpEF and (b) whether, if demonstrated, vascular dysfunction in HFpEF can be improved.
The literature promoting the biological plausibility of both large and small vessel dysfunction driving HFpEF has been extensively reviewed. 13 Increased arterial stiffness predicts incident cardiovascular dysfunction including hypertension, heart failure and peripheral organ damage. 14 In heart failure, an association between increased stiffness and premature death has been demonstrated albeit predominately in the reduced ejection fraction cohort. 15 Ageing is associated with a decrease in the elasticity of large conduit blood vessels, 16 however, this decline is accelerated in patients with HFpEF. 17 Indeed in the RDT-PEF population, age trended with pulse pressure, a crude index of large artery stiffness. 13
Increased myocardial wall stress, systolic and diastolic dysfunction, left ventricular hypertrophy and left atrial dilatation17,18 are commonly observed consequences of increased arterial stiffness and these features mirror those seen in patients with HFpEF. 19 Furthermore, aorta stiffening in selected populations of HFpEF is correlated positively with natriuretic peptide level and negatively with peak oxygen uptake on exercise.2,3,18 Similarly in the RDT-PEF cohort, pulse pressure was correlated with heart failure symptoms and exercise performance.
The large conduit blood vessels function to transform pulsatile flow generated from the heart to a continuous uniform flow at a lower pressure throughout systole and diastole enabling downstream organ perfusion. 20 Arterial stiffness shifts the transition point from pulsatile flow to continuous, distally from the macrovasculature to the microvasculature, which causes end-organ damage and has been extensively demonstrated in the kidneys. 21 This is important, as HFpEF is a condition driven by both cardiac and non-cardiac pathology. 22
Based on these previously published data, it is reasonable to hypothesize that therapies to reverse arterial stiffness and improve ventricular-arterial coupling might be beneficial in patients with HFpEF. 3 In heart failure (both HFpEF and HFrEF), neurohumoral activation (including the SNS) and inflammation leading to endothelial dysfunction have been identified as explanatory mechanisms (and hence targets) for increased vascular stiffness.3,22
Randomised controlled trials in HFpEF have failed to identify an intervention that can reduce aorta stiffness in patients with HFpEF. Therapies investigated to date include angiotensin-converting-enzyme inhibitors, 23 alagebrium, 24 sildenafil 25 and exercise training. 26 The RDT-PEF trial joins this long list of neutral trials, even though there was a signal for improvement in exercise performance and E/e’ at 3 months (albeit not sustained to 12 months follow-up) in those patients randomised to RDT this was not associated with an improvement in vascular function. A common theme in the discussions following all of these trials is that patients with HFpEF are heterogeneous and that future trials should target therapies according to the underlying dominant pathophysiology, e.g. a trial of a new therapy that improves vascular function should recruit HFpEF patients who all have proven abnormal vascular responsiveness, which historically has not been done.
An important observation is that all these trials have used different modalities (invasive pressure catheters, echocardiography, MR, tonometry, oscillometric cuffs) as well as different parameters (carotid femoral PWV, carotid-radial PWV, brachial-ankle, PWV, ascending-thoracic aorta PWV, aorta distensibility, AI, reactive hyperaemic index, albuminuria) to measure arterial stiffness and function. The difficulty with this is that each combination has varying repeatability and furthermore provides a different insight into the macro- and micro-vasculature function that is not comparable. The American Heart Association have recently published a guidance document on how to assess arterial stiffness in research and discuss the lack of a widely adopted and rigorous method of vascular function investigation. 27 They promote the carotid-femoral PWV technique for non-invasive assessment of arterial stiffness. Though this is valuable guidance, it is sobering to note that using data from the RDT-PEF cohort, approximately 536 patients would need to be recruited for an intervention to detect a 15% change in PWV (80% power, P = 0.05, standard deviation = 6.2 m/s), which for many research units seeking to investigate a HFpEF population might be prohibitive.
It is possible that arterial stiffness is not an ideal endpoint to use in an HFpEF clinical trial. The majority of the evidence showing that an intervention can improve arterial stiffness has been in the context of hypertension trials; it is unknown whether the aorta can be ‘unstiffened’ independent of a blood pressure reduction. 27 Also, patients recruited into HFpEF trials tend to be older than those in hypertension trials and consequently reversal of aorta stiffening with an intervention may take longer to manifest (requiring prolonged trial follow-up) or may be impossible reflecting an irreversible stage of the disease process.
We have demonstrated that RDT did not have an effect on blood pressure up to 12 months of follow-up, which is an important safety finding as the majority of patients with heart failure are not hypertensive. This has previously only been demonstrated in an uncontrolled study of seven patients with heart failure and reduced ejection fraction at 6 months follow-up. 28
Finally, improvement in renal blood flow is one of the purported mechanisms of action of RDT. In nine pigs, Tsioufis and colleagues showed that RDT both acutely and chronically after a month increased renal blood flow and reduced resistive index, assessed by an invasive Doppler wire. We were not able to reproduce this finding in 25 humans using spiral renal MR. Similarly in resistant hypertension, improvements in renal perfusion and oxygenation as assessed by MR have not been demonstrated following RDT, 5 though one group showed a decrease in resistive index (derived from ultrasound). 7 These neutral findings might just reflect the fact that the kidneys are well auto-regulated via multiple regulatory mechanisms, which are not all dependent on the SNS. In our population, the high burden of atrial fibrillation may have further complicated imaging and flow assessments.
The main limitation of study is its small size. However, this is the first report of RDT in an HFpEF population and hence the data presented should be used as valuable pilot data to inform sample size calculation for future work in this field. Several controversies remain that need to be addressed before the future role if any of RDT can be ascertained: first, with the technology (multi-electrode vs. single-electrode systems) and how best to apply it (number and location of ablations in the renal artery). When this study was conceived, the Symplicity™ single-electrode device was the only system with supporting efficacy and safety data, which is why it was used. Over the subsequent years, it has become apparent that multi-electrode systems are more likely to achieve a comprehensive denervation. 8 Furthermore, it is likely that the initial technique, which limited four to six ablations in the proximal renal artery prior to any bifurcations may have been too conservative with current data supporting more ablations that also extend to distal branch vessels. 29 Consequently, it remains unknown what the efficacy or safety of contemporary RDT on patients with heart failure are. 30 Finally, until an approach to accurately quantify the effects of RDT on renal sympathetic nerves is developed, it will remain difficult for future phase II studies to show a ‘dose–response’ effect, which will limit the credibility of any findings. 6
Conclusion
Renal denervation did not reduce blood pressure in a population of HFpEF, the majority of whom were normotensive; this is an important safety consideration. The intervention did not improve markers of vascular dysfunction, though with the limited numbers, in this study, it was underpowered to do so. It remains unknown whether pulse wave velocity is a modifiable risk marker in HFpEF.
Footnotes
Acknowledgements
We are grateful to the cardiovascular imaging team from the Laboratoire d’Imagerie Biomédicale, INSERM, France for supplying the ART-FUN software for analysis. We are indebted to the teams at Imperial College Healthcare trust and Guys and St Thomas Healthcare trust who identified patients suitable for inclusion in this trial. We are grateful to Iulia Munteanu and Sally-Ann McNae who served as the research nurses on this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by the Royal Brompton and Harefield NHS trust. The work was supported by the National Institute of Health Research (NIHR) Cardiovascular Biomedical Research Unit, Royal Brompton Hospital and Imperial College, London, UK. ARL is supported by a British Heart Foundation Intermediate Research Fellowship.
Ethical approval
National Research Ethics Service (12/LO/1941).
Guarantor
HCP.
Contributorship
HCP, CH, JK, PDG, RHM, RK, SDR, ARL and CDM contributed to the design of the study. HCP, JK, PDG, RR, RHM and RK were involved in data collection. HCP wrote the first draft. All authors contributed to and approved the final version.