
Abstract
The metabolic syndrome is a condition characterized by a special constellation of reversible major risk factors for cardiovascular disease and type 2 diabetes. The main, diagnostic, components are reduced HDL-cholesterol, raised triglycerides, blood pressure and fasting plasma glucose, all of which are related to weight gain, specifically intra-abdominal/ectopic fat accumulation and a large waist circumference. Using internationally adopted arbitrary cut-off values for waist circumference, having metabolic syndrome doubles the risk of cardiovascular disease, but offers an effective treatment approach through weight management. Metabolic syndrome now affects 30–40% of people by age 65, driven mainly by adult weight gain, and by a genetic or epigenetic predisposition to intra-abdominal/ectopic fat accumulation related to poor intra-uterine growth. Metabolic syndrome is also promoted by a lack of subcutaneous adipose tissue, low skeletal muscle mass and anti-retroviral drugs. Reducing weight by 5–10%, by diet and exercise, with or without, anti-obesity drugs, substantially lowers all metabolic syndrome components, and risk of type 2 diabetes and cardiovascular disease. Other cardiovascular disease risk factors such as smoking should be corrected as a priority. Anti-diabetic agents which improve insulin resistance and reduce blood pressure, lipids and weight should be preferred for diabetic patients with metabolic syndrome. Bariatric surgery offers an alternative treatment for those with BMI ≥ 40 or 35–40 kg/m2 with other significant co-morbidity. The prevalence of the metabolic syndrome and cardiovascular disease is expected to rise along with the global obesity epidemic: greater emphasis should be given to effective early weight-management to reduce risk in pre-symptomatic individuals with large waists.
Introduction
Individuals with cardiovascular disease (CVD) (coronary heart disease (CHD) or cerebrovascular accident) often have a constellation of aetiologically linked cardiometabolic risk factors including dyslipidaemia, high blood pressure and high fasting plasma glucose, which may or may not co-exist with a number of inflammatory markers (e.g. C-reactive protein, uric acid and cytokines) and prothrombotic state (e.g. plasminogen activator inhibitor-1). 1 Reaven 2 was the first to draw attention to this clustering of metabolic abnormalities, particularly in overweight individuals. He coined the name ‘syndrome X’, however, this term is also used by cardiologists to indicate angina-like chest pain in association with reversible electrocardiographic signs of myocardial ischaemia in the absence of flow-limiting stenosis on coronary angiography, 3 a condition also more often found in obese individuals. Other terms have been used previously in the literature such as insulin resistance syndrome and plurimetabolic syndrome, but ‘metabolic syndrome’ has gained international acceptance and International Classification of Diseases coding (E88.81) in the past two decades. Arbitrary cut-offs based on epidemiological studies have been adopted for waist circumference 4 and for the biochemical components.5,6 Recognizing the greater risk of type 2 diabetes and premature CVD in overweight people of Asian origin, compared to those of European origin, lower cut-off values are applied for Asians. Some experts have been critical of the concept of the metabolic syndrome, referring to the dominant role waist circumference over the remaining components of the syndrome such that, in its entirety, the metabolic syndrome appears to add little improvement on waist circumference alone on risk assessment or therapeutic value. 7 While there has been semantic debate as to whether it should be considered a ‘syndrome’, metabolic syndrome has shown extensively to promote the development of diabetes and CVD8,9 and CVD related mortality.9–12 The appearance of the metabolic syndrome phenotype is provoked by weight gain, particularly an increase in intra-abdominal fat accumulation which is mirrored by a large waist circumference. The prevalence of the metabolic syndrome and CVD is expected to rise dramatically in parallel to the global obesity epidemic. Metabolic syndrome doubles the risk of CVD but since its components are all reversible, the diagnosis of metabolic syndrome offers an effective treatment approach – principally weight management.
Classification of body fat and fat distribution
Classification of body mass index and waist circumference and risk of obesity related co-morbidities.

WHO. 12
Lean et al. 4
It is important to point out that BMI is not a strong predictor of body fat: in most studies which have measured estimated total body fat by a reference method (underwater weighing, deuterium oxide dilution dispersal and magnetic resonance imaging), the amount of variance (R2) in body fat explained by BMI is about 70–80% in adults.14,15 Waist circumference predicts body fat similarly, 15 but is a somewhat better guide to cardiometabolic disease risks because it identifies people with relatively low BMI but with increased intra-abdominal fat accumulation. 16 A more rational approach to obesity would use the published, validated, equations to estimate body fat from a combination of anthropometric measurements. 17 Similar equations are available to estimate skeletal muscle mass, which is fundamental to metabolic risk status. 18 All these methods can be used to describe populations and groups, but none is appropriate for classifying individuals.
Diagnostic criteria of metabolic syndrome
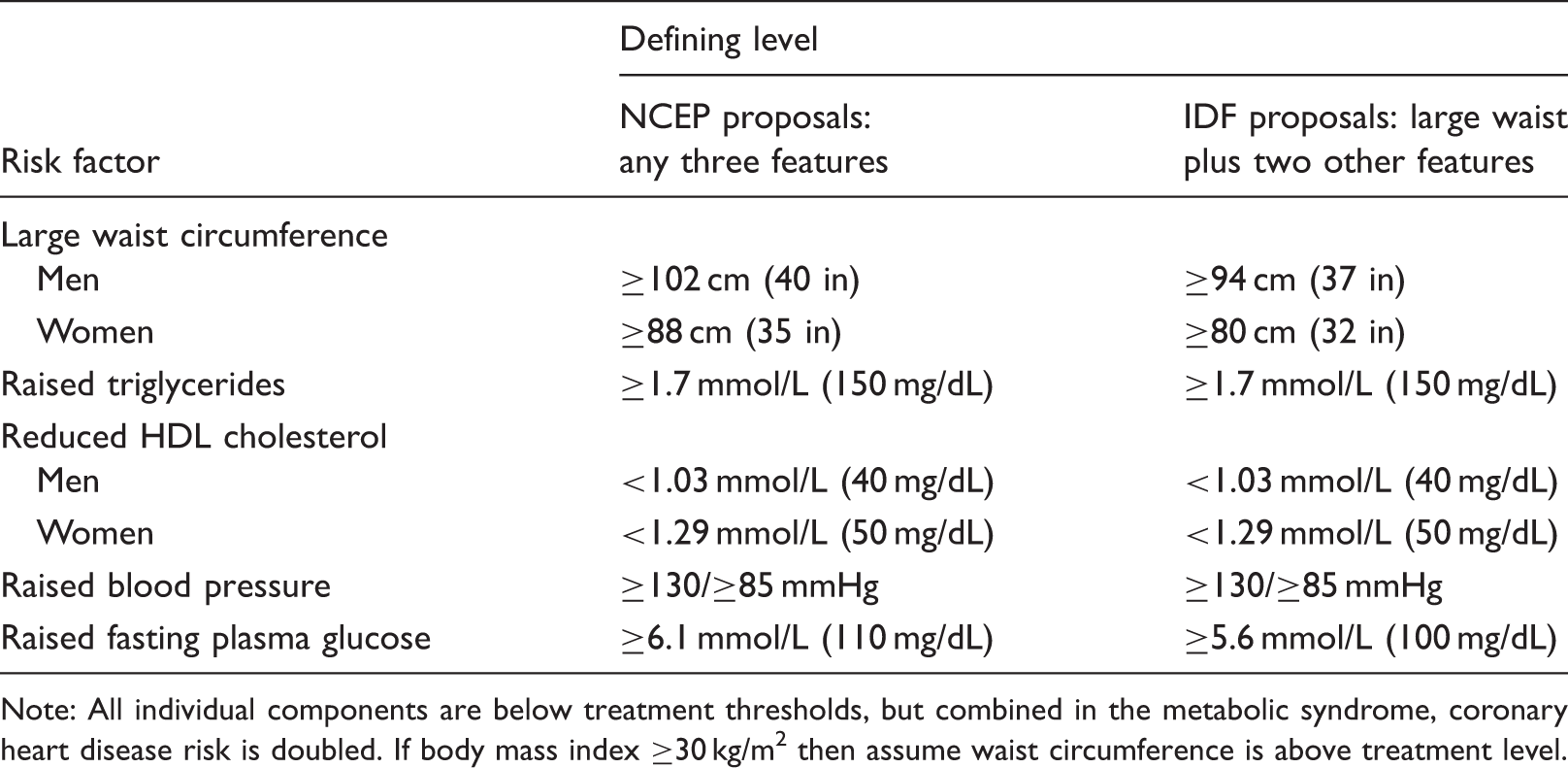
Note: All individual components are below treatment thresholds, but combined in the metabolic syndrome, coronary heart disease risk is doubled. If body mass index ≥30 kg/m2 then assume waist circumference is above treatment level.
Aetiology
Development of metabolic syndrome depends on two elements: firstly adult weight gain, with body fat accumulation and secondly a predisposition to locate fat in intra-abdominal sites, including ectopic fat in liver, pancreas and heart.5,6
The metabolic syndrome is strongly linked to a lifestyle characterized by an easy access to unlimited supply of high caloric, low nutrient-dense, foods and physical inactivity.20,21 This exposure is most potent during early period of life resulting in childhood obesity which is a major risk for metabolic syndrome in adults. 22 Psychosocial stress has also been suggested to contribute, with most metabolic components are more prevalent in socioeconomically deprived populations. 23 Not all individuals go on to develop the metabolic syndrome because of the high individual variation and genetic/epigenetic factors for both the components of the syndrome, for example insulin resistance and dyslipidaemia 24 and body composition 25 and their expression varies with changes in external environment. It is estimated that genetic factors contribute about 30% of the observed variance in BMI but about 70% of the variance in fat distribution that relates more to the metabolic syndrome. 25 The lifestyle factors that increase intra-abdominal fat and metabolic risk factors are weight gain, a diet high in saturated fat, smoking, inactivity and excess alcohol intake.
Increasingly, new insights into genetic basis of obesity have been gained from genome wide association studies (GWAS). The first single nucleotide polymorphism (SNP) associated with increased BMI was mapped to a gene now known as FTO (fat mass and obesity associated) in 2007.26,27 FTO gene acts by regulating appetite and energy expenditure. Over 40 genetic variants since have been identified to associate with BMI, fat distribution or risk of obesity and metabolic syndrome. 28 Although only a small proportion of variance in BMI (<2%) is observed to be attributable to common allelic variants, these risk alleles make substantial contribution to obesity in a polygenic manner such that people who carry a higher number of variants (more than 10) will likely to gain extra weight than those who carry only one or two variants. 29
While certain excessively rare single gene mutations (e.g. leptin deficiency, leptin-receptor defects) can cause massive obesity, usually manifest in early childhood, 30 genetic factors which affect BMI appear to contribute little to the very substantial weight gain needed to generate obesity.
The predisposition to deposit excess body fat in intra-abdominal and ectopic sites appears mainly to be determined very early in life. Poor intra-uterine growth is a recognized factor, 31 suggesting an epigenetic mechanism. 32 There is scattered evidence for other exposures during pregnancy or early infancy, for example maternal smoking. 33 Aside from certain drug effects (e.g. antiretroviral agents promote central fat accumulation, thiazolidinediones reduce it), 34 there is little evidence that any factors in later life can modify fat distribution.
Pathophysiology
High plasma glucose and insulin resistance
Some of the links between components of the metabolic syndrome relate to insulin resistance, although about a third of patients with the metabolic syndrome have normal insulin sensitivity. 35 Insulin resistance is characterized by a high plasma insulin concentration that fails to suppress plasma glucose normally. The contributing factors are complex, a central feature is unresponsiveness to insulin at the cellular level because of changes in receptor binding or post-receptor mechanisms. Exposure to high free fatty acid (FFA) concentrations is a common mediator which is a consequence of an expanded intra-abdominal fat mass. 36 Insulin resistance varies between organs (e.g. subcutaneous/white and intra-abdominal/brown adipose tissues, muscle, liver, skin); this may be important in the clinical manifestation of insulin resistance, pancreatic β-cell dysfunction and impaired insulin secretion. Insulin resistance is closely related to impaired glucose tolerance, diabetes and risk of CHD. 37
High blood pressure and insulin resistance
Many hypertensive individuals have glucose intolerance and hyperinsulinaemia. 36 However, this association is probably not causally linked since controlling hypertension neither improves glucose intolerance or hyperinsulinaemia 38 and hypertension is not observed in patients with insulinoma. 39 On the other hand, obesity contributes to hypertension and hyperinsulinaemia, while weight reduction usually improves both of these disorders. 40 Insulin resistance and hyperinsulinaemia could directly cause hypertension via an increase in catecholamine activity independent of plasma glucose concentration. Increased insulin concentration may also acutely raise blood pressure through insulin-mediated renal tubular reabsorption of sodium. 36
Dyslipidaemia
High triglyceride and low HDL cholesterol levels are core components of the metabolic syndrome. Derangements of these components have been shown to associate with elevated levels of plasma small dense low-density lipoprotein (LDL) cholesterol, the most atherogenic subfraction of LDL, in individuals who are susceptible to gain weight. 41 Individuals with high concentrations of these particles are at increased risk of CVD.41,42
Large waist circumference and intra-abdominal fat accumulation
Increased intra-abdominal fat accumulation, indicated by a large waist circumference, may have a direct intermediary role in the development of the metabolic syndrome. 43 It is thought that the large amounts of FFAs released by the metabolically active intra-abdominal fat mass, via the portal system into the liver, may interfere with hepatic insulin clearance. 44 Intra-abdominal fat which has its origin as brown adipose tissue (mainly omental and retroperitoneal), exhibits greater mitochondrial density and rates of lipolysis and glycolysis than the subcutaneous white adipose tissue. 45 Intra-abdominal fat appears to be primarily involved in high-turnover distribution of FFAs to other body organs. Metabolic complications arise when intra-abdominal fat evolves into a fat storage. Intra-abdominal adipose tissue is an active endocrine organ secreting a range of adipocytokines including leptin, adiponectin, resistin, interleukins (IL) such as IL-1 and IL-6, and tumour necrosis factor alpha (TNF-α), 1 which are important factors in energy regulation. The imbalanced release of these factors by an expanded intra-abdominal fat mass is associated with increased metabolic disorders.
Conditions associated with increased metabolic syndrome and CVD
A number of conditions have been shown to associate with increased risk of obesity, metabolic disorders and CVD that may give clues to underlying pathophysiology of the metabolic syndrome. Individuals with partial lipodystrophy have rare loss-of-function mutations of the PPARγ gene, resulting in subcutaneous adipose tissue atrophy. Such patients have a high incidence of severe insulin resistance, diabetes, dyslipidaemia, hepatic steatosis and polycystic ovary syndrome in females 46 which are mostly reversed by treatment with leptin. 47 By contrast, individuals with acquired partial lipodystrophy (as the result of persistent complement activation) have intact PPARγ and treatment with the PPARγ agonist rosiglitazone increases subcutaneous adipose tissue through adipocyte proliferation. 48 In patients with spinal cord injury, extreme disuse and consequent muscle atrophy and altered muscle fibre characteristics and function (oxidative and anaerobic capacity) is associated with increased central fat distribution and metabolic disorders. 49 Observations of high incidence of the metabolic syndrome in individuals with partial lipodystrophy or those with spinal cord injury have highlighted the important roles of subcutaneous adipose tissue and skeletal muscle in the development of metabolic disturbances. Lifelong exposure to glucocorticoids, such as in patients with congenital adrenal hyperplasia to control hyperandrogenism is linked to excess risk of obesity and metabolic disorders.50,51 In cancer survivors, who are known to have increased risk of CVD, excess rates of obesity and metabolic disorders have been observed which are thought to be the consequence of late effects of chemotherapy and radiotherapy. 52 Low birthweight, a marker of poor early growth, is strikingly associated with metabolic disorders in adult life. Using the thrifty and programming hypotheses, Barker suggested that poor nutrition in utero and early life has an adverse effect on the structure and function of vital organs. 53 Since the endocrine and cardiovascular systems develop late in the foetus, they are more severely affected by undernutrition in the later trimesters. Such individuals would stay unaffected if they remained in an environment of reduced nourishment, but suffer health problems when exposed to certain stimuli such as abundant food, corticosteroids or stress. The time of onset and severity of the disease in adult life is determined by obesity and physical inactivity. These hypotheses help explain, in part, the high incidence of obesity, metabolic syndrome, type 2 diabetes and CHD observed in immigrants from the Indian sub-continent to Western countries. There is evidence that increased central body fat distribution, commonly observed in migrant South Asians compared with general white British, diminished in the next generation of British-born South Asians, at least in females. 54 However, the persistent greater risk of diabetes and hypertension in African Americans 55 and CHD in South Asians 56 who were born in the West compared with white Caucasians suggest other factors, driven by genetic and/or epigenetic processes, are involved to promote body fat and lean body mass development, and more crucially body fat distribution and the less studied muscle fibre composition with are known to have significant impact on insulin sensitivity. There is evidence from various studies to support this notion. A study by Nightingale et al. 57 has suggested that the metabolic sensitivity to adiposity was greater in South Asian children than white European children, while another study has shown that African American women had increased proportions of the less oxidative and more insulin resistant type IIB muscle fibres than white women. 58 These findings are in line with another small study of 20 British South Asians and 20 white British men of similar BMI, showing South Asian men had reduced insulin sensitivity, exercise capacity and skeletal muscle expression of key insulin signalling proteins. 59
Implications of metabolic syndrome prevalence on CVD
The prevalence of metabolic syndrome is estimated to be between 10 and 30%, increasing sharply in older age-groups in most European countries. 60 Data from the National Health and Nutrition Examination Survey showed that the prevalence of metabolic syndrome in the United States was 28% in the 1988–1994 survey and had risen to 34% in the 1999–2004 survey. 61 By the age of 70, the prevalence of metabolic syndrome rose to 42% among American men and women. 62
It is likely that the prevalence of metabolic syndrome will continue to rise in the future given the persistently rising trends in obesity, especially among young people. The epidemic of obesity and metabolic syndrome will have major impact on the future risk of CVD, both short term (10-year risk) and long term (lifetime). As population age, and inactivity and overweight become the norm, world-wide, it is likely that metabolic syndrome will become more frequent in older people. Sarcopenic obesity has yet to be defined in a way that can be used for clinical diagnosis or even for an agreed assessment of survey data, but studies using birth cohorts have shown a disconnect between changes in BMI and waist circumference in older people, with waists continuing to rise even when BMI has plateaued; 63 this implies loss of muscle while fat is still rising: a recipe for metabolic syndrome.
Risk categories suggested by NCEP based on the individual’s risk status.
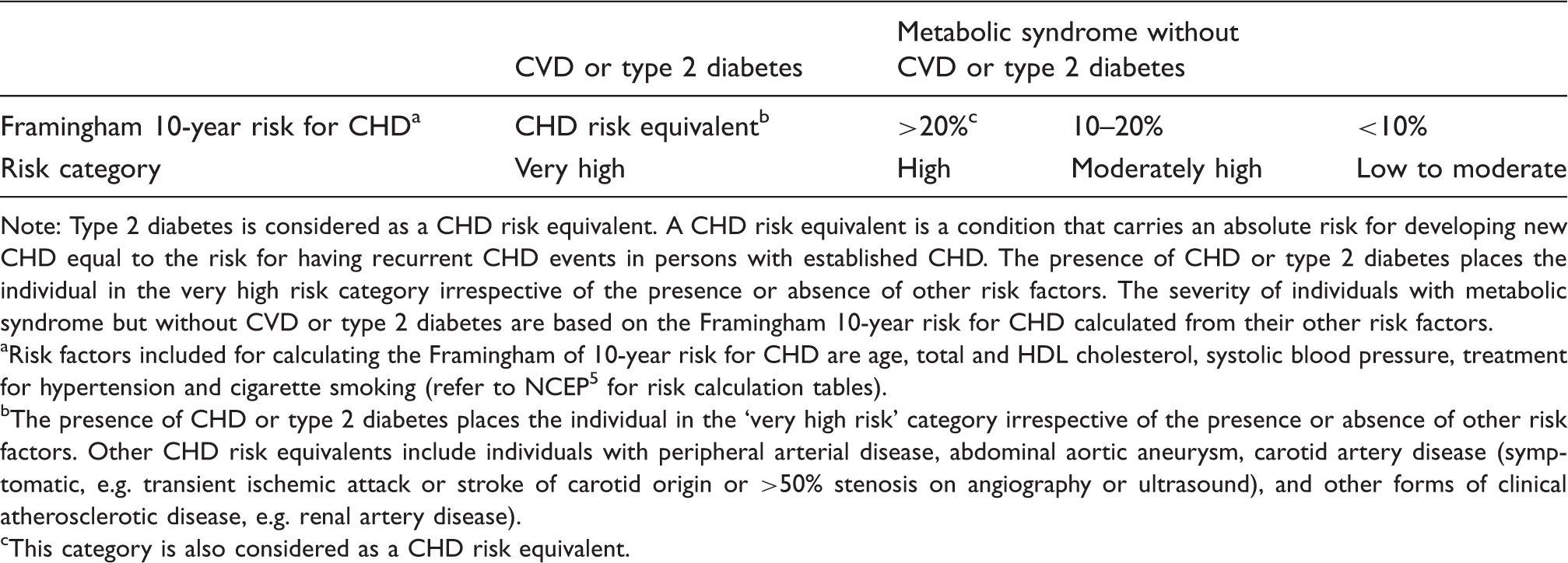
Note: Type 2 diabetes is considered as a CHD risk equivalent. A CHD risk equivalent is a condition that carries an absolute risk for developing new CHD equal to the risk for having recurrent CHD events in persons with established CHD. The presence of CHD or type 2 diabetes places the individual in the very high risk category irrespective of the presence or absence of other risk factors. The severity of individuals with metabolic syndrome but without CVD or type 2 diabetes are based on the Framingham 10-year risk for CHD calculated from their other risk factors.
Risk factors included for calculating the Framingham of 10-year risk for CHD are age, total and HDL cholesterol, systolic blood pressure, treatment for hypertension and cigarette smoking (refer to NCEP 5 for risk calculation tables).
The presence of CHD or type 2 diabetes places the individual in the ‘very high risk’ category irrespective of the presence or absence of other risk factors. Other CHD risk equivalents include individuals with peripheral arterial disease, abdominal aortic aneurysm, carotid artery disease (symptomatic, e.g. transient ischemic attack or stroke of carotid origin or >50% stenosis on angiography or ultrasound), and other forms of clinical atherosclerotic disease, e.g. renal artery disease).
This category is also considered as a CHD risk equivalent.
Medical management
Management of the metabolic syndrome through lifestyle changes and drugs to reverse modifiable risk factors for atherosclerotic disease.
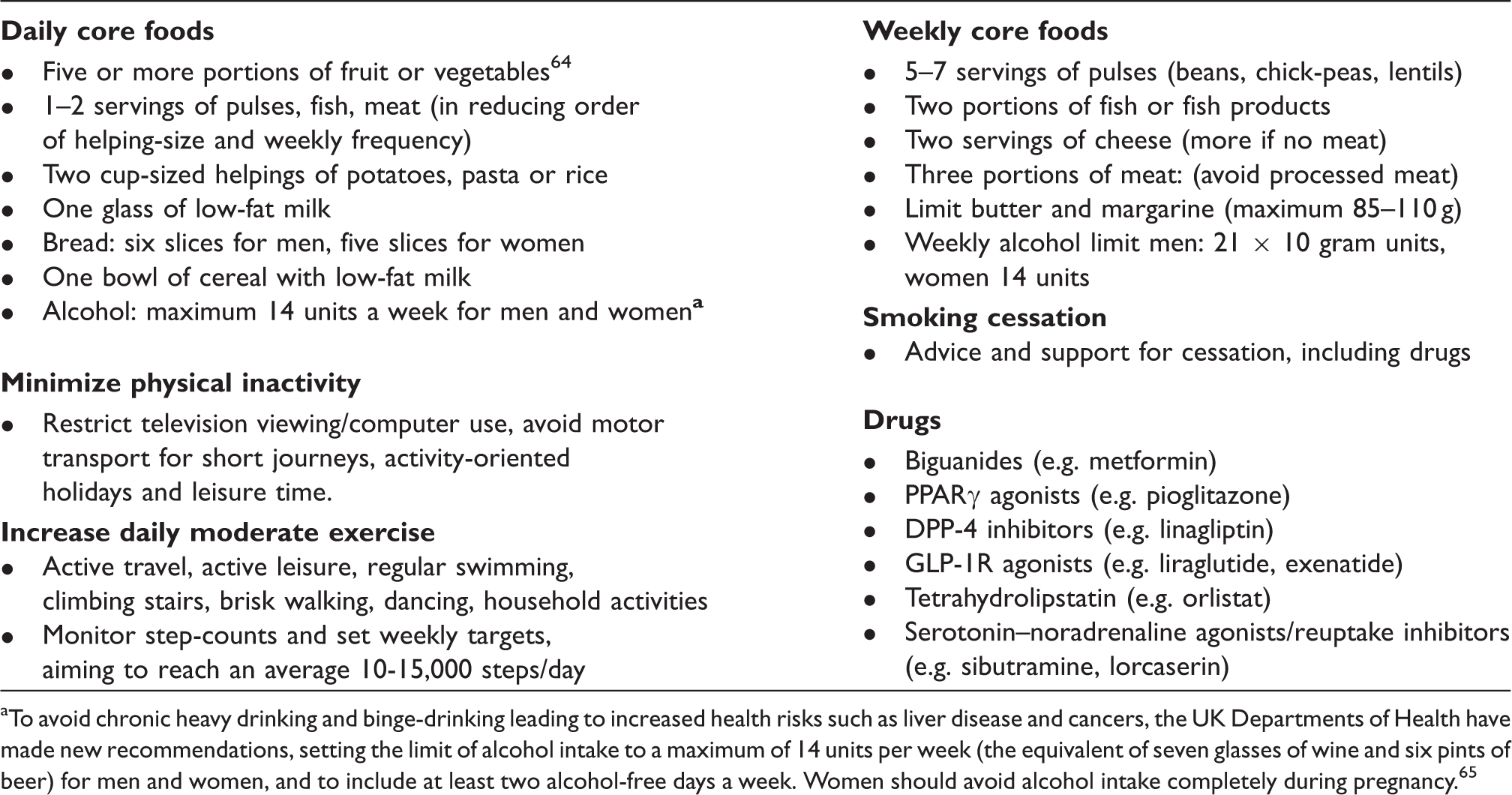
To avoid chronic heavy drinking and binge-drinking leading to increased health risks such as liver disease and cancers, the UK Departments of Health have made new recommendations, setting the limit of alcohol intake to a maximum of 14 units per week (the equivalent of seven glasses of wine and six pints of beer) for men and women, and to include at least two alcohol-free days a week. Women should avoid alcohol intake completely during pregnancy. 65
Pragmatic suggestions for the management of elevated waist circumference in relation to CVD risk (adapted from Lawlor et al. 66 ).
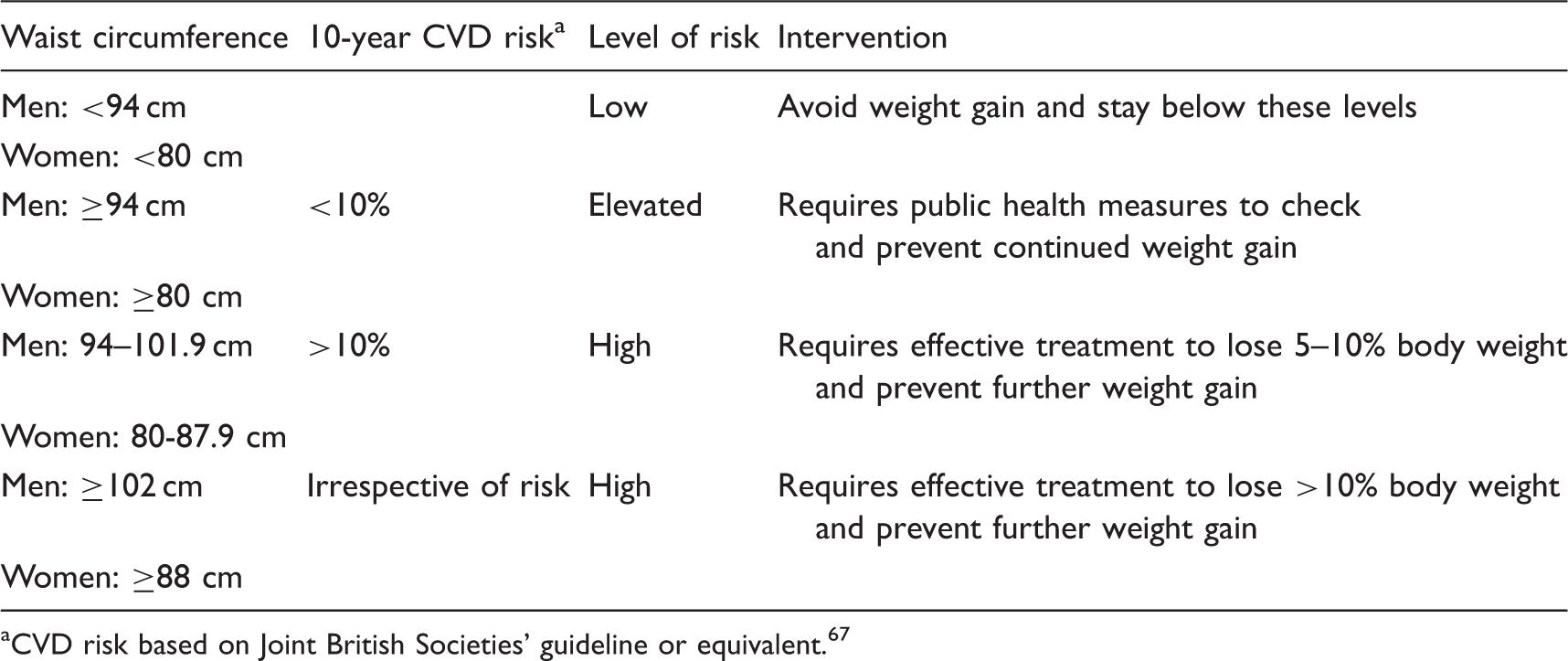
CVD risk based on Joint British Societies’ guideline or equivalent. 67
Drug therapy is directed towards the major risk factors. A number of drugs have been shown to improve more than one metabolic syndrome component and may shed lights to the underling biochemical disorders. The PPARγ agonists thiazolidinediones act by shifting intra-abdominal fat to subcutaneous fat depot 34 with an associated improvement in glucose tolerance and lipid profile. The expanded mass of metabolically favourable subcutaneous adipose tissue appears to serve as a sump for glucose and lipid disposal. Biguanides, used to treat type 2 diabetes, have also been shown to improve lipid profile and regulate menstrual cycles and increase fertility in patients with polycystic ovary syndrome. However, biguanides have not been shown to modify all components of the metabolic syndrome and not known to alter body fat distribution.
Treatment with anti-obesity drugs such as tetrahydrolipstatin (e.g. orlistat) 73 and serotonin–noradrenaline reuptake inhibitors (e.g. sibutramine – note: this drug has been withdrawn from some countries) 74 leads to weight loss and, more importantly, reduction in long-term weight regain. These drugs have been shown to reverse or delay most components of the metabolic syndrome. Orlistat has been shown to reduce the incidence of metabolic syndrome and of diabetes by 30–40% 75 and sibutramine is expected to have similar properties, but their effects on CHD are unknown. One of the adverse effects of orlistat is the unpleasant and often intolerable loose bowel movements which increase more frequently with greater fat ingestion. Serotoninergic agents may have independent effects on blood pressure and glucose tolerance, but do not have identical actions; sibutramine tends to raise blood pressure unless this is counteracted by the blood pressure reduction that occurs with weight loss, while fluoxetine has a minimal effect on appetite. Although sibutramine treatment is contra-indicated in individuals with high cardiovascular risk factors, the Sibutramine Cardiovascular Outcome Trial (SCOUT) has shown that sibutramine treatment with weight management is well tolerated by the majority of high-risk individuals with CVD. 76
Two classes of insulin secretagogues are currently in use for treating patients with type 2 diabetes who have sufficient β-cell reserve. The oral agents dipeptidyl peptidase-4 (DPP-4) inhibitors act by increasing endogenous activity of glucagon like peptide-1 (GLP-1) while the injectable GLP-1 receptor (GLP-1R) agonists directly activate GLP-1R expressed in the pancreatic β-cells, leading to enhanced insulin synthesis and secretion in the presence of elevated plasma glucose. 77 GLP-1R agonists have also been shown to suppress the secretion of glucagon. Since GLP-1 receptors are expressed in a wide range of extra-pancreatic organs, including the gastrointestinal tract and the brain, GLP-1R agonists have major effects on the gut–brain axis by delaying gastric emptying and promoting hypothalamic satiety, resulting in weight loss 78 and reduction in hepatic fat content, but the evidence of their long-term effects on metabolic disturbances is not yet available. A few studies of small samples and short term duration of treatment with DPP-4 inhibitors have shown conflicting results 79 while Boschmann et al. 80 found no changes in a number of risk factors.
One of the recently approved anti-obesity drugs by Food and Drug Administration and European Medicines Agency is the combination of bupropion and naltrexone (approved name Contrave in the United States and Mysimba in Europe). Bupropion, usually used as treatment for depression and smoking cessation, is an aminoketone acting as a mixed dopamine/norepinephrine reuptake inhibitor. 81 Naltrexone, used as treatment for alcohol dependence, is an opioid receptor antagonist which reduces cravings by inhibiting the action of β-endorphins on dopaminergic reward pathways. 82 Treatment with the combination of sustained-release naltrexone (32 mg/day) and bupropion (360 mg/day) over 56 weeks has been shown to reduce body weight by 6.1 kg (equivalent to 6.1%). 83
In general, weight loss through diet and lifestyle plus anti-obesity drugs results in improvement in all the cardiovascular risk factors of metabolic syndrome. Some drugs, through their mode of action, have weight-independent actions to enhance the benefit of weight loss (e.g. orlistat on lipid-lowering, liraglutide on blood pressure and glucose-lowering). In some cases, drug affects may attenuate slightly the cardiovascular benefit of weight loss (e.g. weight loss with Contrave/Mysimba, or with sibutramine, reduces blood pressure, but to a lesser degree than for the same amount of weight loss if that can be achieved without the drug).
Surgical management
Medical treatment of obesity remains ineffective, particularly long-term weight loss, for a large number of people even when intensive lifestyle modification combined with the limited available pharmacological agents. Bariatric surgery offers an alternative, but it has never been shown that bariatric surgery works well in people who have failed with a formal drug and diet approach. People who fail with one approach tend to fail with others. The National Institute for Health and Clinical Excellence has made clear guidelines for individuals who should be considered for bariatric surgery, 84 to reduce intake or absorption of calories. Various surgical procedures are now available including gastric banding, sleeve gastrectomy and gastric bypass. Criteria for bariatric surgery require a BMI of above 40 or 35–40 kg/m2 with other significant co-morbidity (e.g. sleep apnoea, type 2 diabetes or hypertension) that could be improved by weight loss. The individual is usually required to have exhaustively undertaken appropriate non-surgical approaches, but failed to achieve clinically beneficial weight loss for at least six months, to be fit for anaesthesia and surgery, and to commit to the need for long-term follow-up. All bariatric surgical procedures have potential complications, therefore should be performed in a specialist centre.
Demand for gastric bypass surgery under the UK National Health Service has risen by six-fold (from 808 to 5407 cases) in the five-year period between 2006–2007 and 2011–2012. 85 Similar patterns have been observed in the United States. 86 In the current frenzy to escalate bariatric surgery, it may be prudent to step back and reflect on the ultimate goal of management. The greater, more rapid weight losses by surgery are off-set by a number of permanently social and health consequences that the individual has to adapt, including interference with daily activities such as the impossibility of eating normal family meals and the hazards of dumping syndrome, and of micronutrient deficiencies, coupled with the need for revisionary surgery in 10–20% of cases. 87 It is important therefore optimized non-surgical approaches should be offered readily for obese individuals. 88 If the aim is a more modest maintained weight loss of 15 kg (adequate to reverse type 2 diabetes) is the target, then low-energy liquid diet methods may be cheaper and safer than surgical option. 89
Effects of weight loss on risk factors of metabolic syndrome using by various regimens of low calorie diet, exercise, orlistat, liraglutide and bariatric surgery, reported in selected representative studies.

Weight instead of BMI was reported.
Range was reported.
Glycosylated haemoglobin reported.
Prevention
It is likely that risk factors exist long before overt symptoms of the metabolic syndrome and CVD are expressed. Some individuals carry their risk from an early age because of childhood obesity while others endured even longer period due to their intra-uterine growth retardation. A greater emphasis should be given to risk prevention of pre-symptomatic individuals. At-risk individuals can be screened from their family history. Regular physical activity and modest weight loss is likely to prevent most features of metabolic syndrome and, can even reverse all its components in those with the existing syndrome, thereby reducing its prevalence and incidence, as well as preventing new cases of diabetes. Smoking cessation is highly important not only to the individuals, but also to their offspring to avoid intra-uterine growth retardation and adverse epigenetic modification leading to adult obesity. Anti-obesity drugs or other agents such as PPARγ agonists and GLP-1R agonists may also be considered as primary prevention of metabolic syndrome and CVD.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MEJL has received research funding from, and provided professional consultancy to, Novo Nordisk, Orexigen, Counterweight Ltd and Cambridge Weight Plan.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
None.
Guarantor
Not applicable.
Contributorship
TSH wrote the first draft, and with MEJL edited the manuscript.
Provenance
Invited contribution.