
Abstract
A 34-year-old man found a mildly tender preauricular mass. Ultrasonography revealed an anechoic mass in the superficial lobe of the parotid gland. Magnetic resonance imaging showed thin ring-like contrast enhancement and homogenously high intensity on T2-weighted images. The mass was resected due to its rapid growth. The cystic lesion contained keratine-like material and a stratified squamous epithelium without granular layers, which was consistent with keratocystoma.
Introduction
Of various tumors of the parotid gland, keratocystoma is a relatively new entity, first being defined by the pathologist Nagao et al. (1). To the best of our knowledge, so far only six cases of this benign tumor have been reported (1–4). Although these papers describe the histopathological characteristics of the tumor, we were unable to find any literature reporting radiological findings of keratocystoma. The purpose of this report is to describe the imaging findings in a case with a verified keratocystoma examined with ultrasonography (US), magnetic resonance imaging (MRI), and salivary scintigraphy.
Case report
A 34-year-old man noticed a small mass in the left preauricular region. The mass was painless at rest, but slightly tender when pressed. The subject had no symptoms of upper airway infection. The patient visited our ear, nose, and throat (ENT) clinic 1 month after he first recognized the mass.
The patient had no history of malignant tumor or other ENT complications, no relevant family history, and no history of tobacco or alcohol abuse.
The mass was unrecognizable on the surface of the face. Physical examination revealed a moderately hard, well circumscribed, smoothly movable mass of less than 1 cm in diameter. No facial nerve palsy was observed. No mass was palpable in the right preauricular region. There was no diffuse swelling of the parotid glands. No abnormal neck node swelling was found on palpation.
US showed an anechoic lesion (6 × 6 × 6 mm) with posterior echo enhancement in the
left parotid gland (Fig.
1a). No other mass was found in the parotid glands. The parotid gland
parenchyma had a normal echoic signal. US revealed no enlarged neck nodes. (a) US image of the left parotid gland showed a
low echoic mass (arrow) with posterior echo enhancement (arrowhead) in
the border zone between the superficial lobe and subcutaneous tissues.
(b) T2W MRI showed a well-defined and slightly lobulated lesion with
homogenously high intensity. This lesion had high intensity on DWIs (c)
and slightly increased ADC (d). The mass had homogenously low intensity
on T1W images (e), and ring-like enhancement after the injection of
gadolinium contrast medium (f).
On T2-weighted (T2W) MR images (3.0-Tesla Achieva TX, Philips Medical Systems, Best, The Netherlands), the mass was seen as a slightly lobulated lesion with homogenously high intensity and well-defined margins (Fig. 1b). Diffusion-weighted images (DWIs) (b factor = 1000) showed high intensity with slightly increased apparent diffusion coefficient (ADC) (1.04 × 10−3 mm2/s) (Fig. 1c, d). On T1-weighted (T1W) images, the mass showed homogenously low signal intensity (Fig. 1e). After injection of gadolinium contrast medium (0.2 mmol/kg), we observed ring-like enhancement with a smooth outline in the rim of the mass (Fig. 1f). The central part of the mass did not enhance.
Salivary gland scintigraphy using 99mTcO4− was performed to detect tumors retaining saliva, such as Warthin’s tumors. We found no abnormal uptake in the tumor, indicating that the mass did not contain saliva.
Since the imaging results were inconclusive, an experienced ENT physician performed a fine-needle cytology test using a 22-gauge needle. The aspirated liquid was moderately viscous and contained predominantly neutrophils and a small number of atypical epithelial cells. No cells with nuclear atypia indicating malignancy were observed in the sample. These findings indicated an inflammatory condition of the lesion. The patient was given a broad-spectrum antibiotic agent (levofloxacin, 500 mg/day) for 1 week. The pain gradually receded. During the next few months, the patient occasionally experienced tenderness of the lesion, which was relieved by antibiotics.
Five months after onset, the tumor became large enough to be recognized visually on the surface. Although the imaging studies and cytology test previously performed did not indicate malignancy of the lesion, its continuing growth justified surgical resection. A left superficial parotidectomy was performed under general anesthesia 6 months after onset. The facial nerve was carefully preserved, and the patient showed no facial nerve palsy after the surgery.
Histologically, the tumor consisted of a 19 × 19-mm cystic lesion filled with
keratinous materials. The cystic space was lined with a stratified squamous
epithelium without granular layers (Fig. 2). The thickness of the epithelium varied from thin to some
thicker areas. There were also some smaller islands of benign squamous epithelium
present in the surrounding stroma. One focus of granulomatous inflammation to
keratin materials was present as well as foci of lymphocytic inflammation. Salivary
gland lobules adjacent to the cystic lesion showed mild atrophy. The lack of
granular layers ruled out dermoid or epidermoid cyst. These findings are consistent
with keratocystoma (1).
There was no evidence of malignancy. The tumor was considered to be completely
excised, and no recurrence has been observed during the follow-up 17 months after
the operation. Histological findings (hematoxylin and eosin stain).
(a) A low-power view shows that the tumor consists primarily of a large
cystic lesion lined with a stratified squamous epithelium. (b)
High-power views show that the squamous epithelium is lacking a granular
layer. (c) Granulomatous inflammation of keratin materials (arrows) can
also be seen.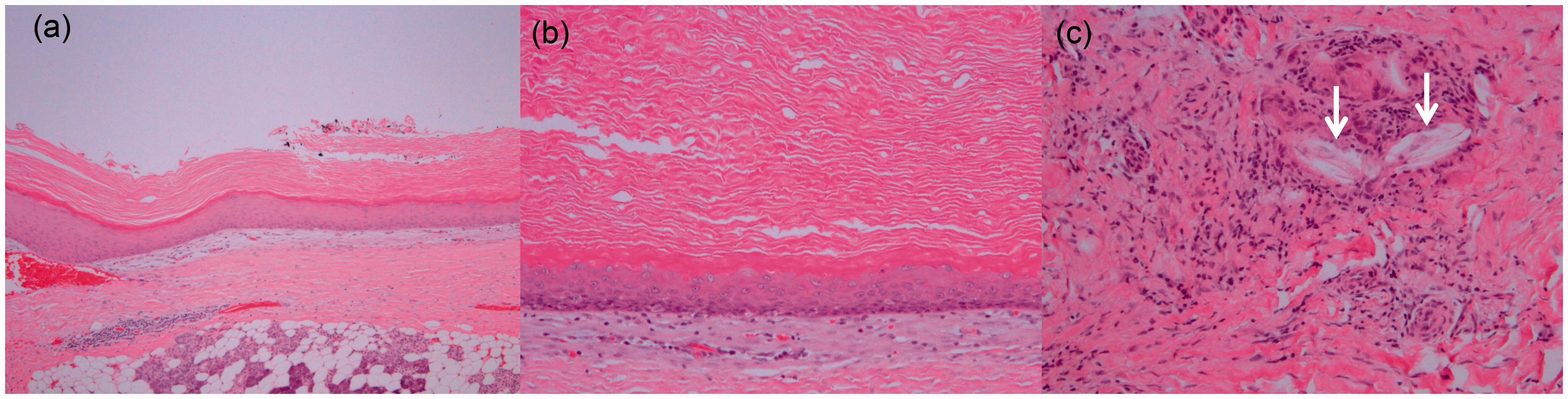
Discussion
This tumor can be summarized as a cystic lesion without a solid component. The lesion had a homogenously thin wall that was enhanced by gadolinium contrast medium. It showed gradual growth over months and occasional tenderness which was ameliorated by antibiotics. The tumor was resected and the pathological diagnosis was keratocystoma.
The US images suggested the mass to be a pleomorphic adenoma, which is the most common benign parotid tumor, or a purely cystic lesion. The MRI findings, however, differed from the typical findings of a pleomorphic adenoma, which usually presents with a solid component with intensive enhancement (5). Ring-like enhancement indicated a viable cell component along the wall. We considered the possibility of less common entities, such as epidermoid tumor or necrotizing lymphadenitis. Infection of an existing cystic lesion (lymphangioma, lymphoepithelial cyst, or type I first bronchial cleft cyst) and cystic formation of a Warthin’s tumor were also considered.
There are only four previous papers reporting a total of six patients with keratocystoma: three men (age range, 18–38 years) and three girls/women (age range, 8–49 years) (1–4). Four of these six patients showed gradual growth of the lesion over months or years. In the present case, both the age of the patient and the growth rate of the tumor are similar to those in the previous reports.
The MRI signals of the lesion (i.e. a low signal on T1W images, a high signal on T2W images, a high signal on DWIs, and a slightly increased ADC) seem to be atypical for keratin, which usually shortens T2 resulting in a low signal on T2W images. In previous papers, cholesteatoma lesions containing keratin displayed a high signal on DWI and decreased ADC (6), whereas epidermoid cysts, which usually contain keratin, showed no marked decrease in ADC (7). In this case, we speculate that the high signal of the T2W images and the slightly increased ADC might be ascribed to other components than keratin in the tumor as seen in epidermoid cysts. Use of different MRI scanners could also influence ADC. The ring-like enhancement in the wall is thought to express hyperpermeability of the squamous epithelium with foreign-body reactions.
We examined this tumor using salivary scintigraphy. The tracer did not accumulate in the tumor. Unlike Warthin’s tumor, we suggest that salivary scintigraphy may not be useful for diagnosing keratocystoma because many other salivary tumors show no tracer uptake.
In conclusion, we have presented the radiological findings of a keratocystoma. Keratocystoma should be included in the differential diagnosis in cases with a cystic parotid lesion, which may help pathologists in making the correct diagnosis.
Footnotes
Conflict of interest
None declared.