
Abstract
Heart failure is a complex syndrome affecting several organs including kidney, lungs, liver, brain muscles and sympathetic system. Each of these organs might contribute to its severity and prognosis. The prognosis assessment is critical for a correct heart failure management. It has already been demonstrated that a single parameter is weaker for prognosis than different parameters combined. The Metabolic Exercise test data combined with Cardiac and Kidney Indexes (MECKI) score has been built and validated for heart failure with reduced ejection fraction (HFrEF) patients by considering cardiopulmonary exercise test data combined with clinical, laboratory and echocardiographic measurements. The betablockers treatment is a milestone in the HFrEF management. In the MECKI score database, the association of betablockers treatment with outcome has been investigated in different settings.
Keywords
Beta-blockers, heart failure prognosis and scores
Several heart failure scores have been proposed based on clinical evaluation, laboratory findings, comorbidity analysis and data from echocardiography and cardiopulmonary exercise testing (CPET). There are prognostic scores for acute and chronic heart failure, right heart failure and end-stage heart failure. Beta-blockers (β-blockers) therapy is frequently included as a prognostic index.
By adding CPET- and six-minute walking test-derived variables to the Seattle Heart Failure Model (SHFM) a minimal improvement of the assignment of risk was obtained. 1
The Heart Failure Survival Score (HFSS) was conceived for risk stratification in patients with advanced heart failure, providing effective risk stratification with or without β-blockers therapy. 2
Comparing the prognostic accuracy of the Metabolic Exercise test data combined with Cardiac and Kidney Indexes (MECKI) score, 3 HFSS 2 and SHFM1 for the combined endpoint of cardiovascular death, urgent heart transplantation, or ventricular assist device implantation, Agostoni et al. 4 demonstrated that the prognostic accuracy of the MECKI score was superior to that of HFSS and SHFM in stable heart failure patients. In the MECKI score database, testing the prognostic role of oxygen consumption (VO2) at the anaerobic threshold, β-blockers and digoxin therapy turned out to be significant prognostic indexes. 5 In another analysis from MECKI score database, in ≥70 years-old heart failure patients, the use of β-blockers was one of the independent predictors of the primary endpoint (composite of cardiovascular death and urgent heart transplantation). 6
The MAGGIC risk score is a simple and powerful method of risk stratification for both morbidity and mortality in heart failure with preserved ejection fraction (HFpEF). 7 In its final model, not prescribed β-blockers was included between highly significant independent predictors of mortality.
β -blockers selectivity and dosage regimens in heart failure prognosis
Guidelines recommend that β-blockers should be titrated up to a maximum or target dose unless contraindicated or intolerant 8 but the target dose has been achieved only in one-third to one-fourth of patients in clinical practice. Data from the MECKI score database showed a better outcome in heart failure with reduced ejection fraction (HFrEF) patients receiving a high daily dose (>25 mg carvedilol equivalent daily dose) than in both medium dose (12.5–25 mg) and low dose (<12.5 mg), with no differences between the last two groups. 9 In HFrEF patients, there were more improvements in outcomes with higher β-blockers dose than with reduced heart rate, suggesting that titration of β-blockers dose gives a greater benefit than reduction of heart rate in such patients (HF-ACTION trial). 10 Few studies have compared different β-blockers in HFrEF. In heart failure patients with chronic obstructive pulmonary disease (COPD), bisoprolol reduces the incidence of chronic heart failure and/or COPD exacerbation compared with carvedilol. 11 In the MECKI score database, β-blockers were associated with a more favourable prognosis (composite outcome of cardiovascular death, urgent heart transplantation or left ventricular assist device implantation) without any difference between β1- and β2-receptor-blockers versus β1-selective blockers. 9 In a propensity matched study, treatment with bisoprolol or carvedilol, both at high and at lower doses, is associated with an improved prognosis of patients newly diagnosed with HFpEF. 12
β -blockers, heart failure prognosis and exercise parameters
Exercise limitation is a common issue in patients with heart failure. CPET is an important tool to assess functional status and prognosis in heart failure. Among the CPET measures of aerobic efficacy, peak VO2 and ventilatory efficacy assessed through the measurement of the slope of relationship between minute ventilation and carbon dioxide production (VE/VCO2) represent the most useful parameters to assess prognosis, as demonstrated by the MECKI score data. 3 Moreover, in patients with severe heart failure, defined as those with low peak VO2, VE/VCO2, reported as percentage of predictive value, showed to have a stronger prognostic capacity. 13 Notably, the MECKI score population was mostly treated by β-blockers (81–87%).3,13 For any peak VO2 class, patients treated with β-blockers showed better survival rate. 14 Consequently, recent published criteria for heart transplantation have proposed different cut-off criteria: peak VO2 ≤14 mL/kg/min and ≤12 mL/kg/min in heart failure patients without and with β-blockers, respectively, are recommended to guide listing to heart transplantation. 15 Another prognostic heart failure parameter is the exercise oscillatory ventilation (EOV), a specific behaviour of ventilation consisting of a regular waxing and waning of ventilation (hyperpnoea and hypopnoea), which may persist throughout the entire exercise or disappear before peak exercise. MECKI score data confirmed that the presence of EOV in patients with HFrEF or heart failure with mid-range ejection fraction is associated with worse survival and identifies heart failure patients requiring a more intensive follow-up and a more aggressive treatment. 16 There was no difference in β-blockers treatment (88% vs. 89%) between EOV+ and EOV– groups. Finally, the oxygen uptake at the anaerobic threshold (VO2AT), a CPET derived variable that has proven to be a strong independent predictor of outcome in heart failure patients, can be adopted as complementary/alternative to peak VO2 in pre-operatory cardiovascular risk stratification, being independent of patient’s motivation, exercise protocol and exercise duration. 5 However, the MECKI score data demonstrated that different cut-off values between sinus rhythm and atrial fibrillation should be adopted. Notably, β-blockers were prescribed more frequently in the sinus rhythm group, likely influencing the findings. 5
β -blockers, heart failure prognosis and gender
Heart failure occurs at an older age and with less ischaemic aetiology in women than in men. 8 HFpEF represents the dominant form of heart failure in women with more frequently predisposing risk factors, such as hypertension, diabetes, renal dysfunction, obesity and low-grade inflammation. 8 Some gender differences are described for the efficacy and adverse effects of medical therapy. Compared with men, mortality under digitalis treatment, as well as the rate of adverse drug events, principally with the use of diuretics, anticoagulants and angiotensin converting enzyme inhibitors, is higher in women. On the contrary, no difference in β-blockers efficacy and occurrence of adverse events, such as dizziness, diarrhoea, diabetes or depression, are evidenced according to sex.17,18 However, several studies have shown that women receive suboptimal treatment and, in particular, β-blockers are less frequently prescribed.19,20
Heart failure women have better clinical outcome than men, even though peak VO2 was lower compared with men, raising doubts about the accuracy of risk assessment by CPET in women. Recently, Corrà et al. 21 evaluated whether the predictive role of CPET risk indexes (i.e. VO2 and VE/VO2 slope) was sex independent and whether sex-related characteristics that impact heart failure outcome should be considered as associations that may confound the effect of sex on survival. They found that the low peak VO2 and female association with better outcome in heart failure might be false if sex-specific differences (e.g. body mass index, left ventricular ejection fraction, incidence of non-ischaemic cause, prevalence of atrial fibrillation) were correctly taken into account, suggesting that, for an effective and efficient heart failure model, adjustment must be made for sex-related characteristics. Notably, there was no difference in β-blockers treatment between male and female groups in ‘sex’ studies on CPET and outcomes.
β -blockers and heart failure prognosis in special setting
Elderly heart failure patients
Heart failure is one of the most important causes of hospitalization and death among patients aged >65 years and age is one of the major determinants of prognosis in heart failure patients. 8 Several demographic changes are noted with advancing age, such as higher prevalence of women, more ischaemic aetiology, higher systolic blood pressure, lower heart rate and reduced kidney function; these factors can affect the heart failure prognosis of heart failure patients in different ways.
Like the majority of heart failure trials, major β-blockers trials enrolled a proportion of elderly patients which does not reflect the real world. The SENIORS trial 22 evaluated the effect of nebivolol in patients aged ≥70 years with heart failure and demonstrated both the efficacy and tolerability of nebivolol in an elderly heart failure cohort. This evidence is supported by a recent meta-analysis of patients with HFrEF in sinus rhythm, 17 which demonstrated that the effect of β-blockers remained significant and that drug discontinuation was no higher in older age groups. Recently, Carubelli et al. 23 evaluated the relationship between age, exercise tolerance and the prognostic value of the MECKI score and showed that older heart failure patients had higher prevalence of comorbidities, lower exercise performance and higher MECKI score compared with younger patients. Moreover, they found that, in patients aged ≥70 years, the use of β-blockers, as well as high left ventricle ejection fraction (LVEF), kidney function, peak VO2, serum sodium, is associated with lower risk of cardiovascular death and urgent heart transplantation.
Chronic kidney disease
Renal dysfunction is one of the most relevant comorbidities in heart failure and its severity degree impacts significantly the outcome in heart failure patients. Recently, it was demonstrated that renal dysfunction positively correlated with decreased peak VO2, independently of other established factors influencing peak VO2, suggesting that renal dysfunction may contribute to exercise intolerance in heart failure. 6 There was no difference in β-blockers treatment between groups. The mechanisms that potentially link renal dysfunction to reduced exercise performance were not totally clear. It was supposed that dysfunctional kidneys may act as an amplifier of sympathetic activation in heart failure, leading to decreased responsiveness of the heart to catecholamines. This condition results, during exercise, in a limited ability to increase cardiac output, an increased peripheral vascular resistance and an impaired skeletal muscle vasodilatation capacity, leading to muscle hypoperfusion. Moreover, chronic sympathetic activation may contribute to skeletal myopathy. These combined abnormalities are causally linked to reduced exercise capacity in heart failure. β-blockers play an important role in balancing the sympathetic hyperactivity of heart failure patients, in both those with and those without renal dysfunction. Indeed, in patients with HFrEF and moderate or moderately severe renal dysfunction, β-blockers reduce mortality and do not lead to any overall deterioration in renal function. 24 However, the true efficacy in patients with severe renal dysfunction is still unclear.
Anaemia
Anaemia is frequently observed in heart failure patients and the presence of anaemia is associated with a higher all-cause mortality and hospitalization rate as an independent risk factor. 8 The MECKI Score Group evaluated 3913 heart failure patients with different haemoglobin (Hb) values to assess prognosis and the role of established heart failure prognostic parameters in this setting. 25 In line with several previous reports, MECKI score data confirmed that anaemia influences heart failure prognosis, adding the demonstration of a direct correlation between Hb level and prognosis below but not above 12 g/dL. Moreover, established heart failure prognostic parameters, such as peak VO2 and LVEF, maintain their validity in the anaemia setting, suggesting the use of a multiparametric prognostic approach also in heart failure patients with low Hb. Notably, 84.6% of the study cohort patients were treated with β-blockers with equal results in groups with different Hb values.
However, the mechanisms by which anaemia worsens the prognosis of heart failure patients are yet unclear and the β-blockers’ effect on the prognosis of heart failure patients with or without anaemia remains unproved. A recent sub-study of the Japanese Chronic Heart Failure Study evaluated the effect of anaemia in HFrEF patients receiving carvedilol therapy, demonstrating that low Hb was associated with a blunted response to β-blockers. These data suggested that the deleterious effects induced by heart failure-related anaemia might lead to persistent left ventricle remodelling refractory to carvedilol therapy. 26
Severe heart failure
Recent updated Heart Failure Association of the European Society of Cardiology criteria define advanced heart failure as a chronic condition characterized by severity of symptoms, cardiac dysfunction/abnormalities, brain natriuretic peptide elevation and functional limitation in patients with several episodes of congestion or low cardiac output. 27 Accurate assessing of prognosis is crucial in advanced heart failure to plan treatment and follow-up strategies. β-blockers are involved in both.
The impossibility to tolerate and/or titrate β-blockers is one of the crucial signs of bad prognosis, as underlined in the simple acronym proposed for identification of severe heart failure patients to refer for advanced therapies: ‘I NEED HELP’. 27 The letter P represents ‘Prognostic medication’, such as inability to optimize therapy, including β-blockers. The MECKI score Group evaluated 715 ambulatory severe heart failure patients, demonstrating that the absence of β-blockers per se predicts worse survival, as in the ‘I NEED HELP’ message, heart failure patients without β-blockers being an independent risk population. 14
Moreover, the role of CPET, traditionally considered a crucial part of the evaluation of advanced heart failure for heart transplantation, was evaluated. CPET parameters, as well as heart failure prognosis, are influenced by β-blockers treatment, so that cut-offs considered for heart transplantation are peak VO2 <12 mL/kg/min for patients with β-blockers and 14 mL/kg/min for patients without β-blockers. 15 The MECKI Score Group confirmed that optimized medical therapy, especially with β-blockers, offers an important improvement of long-term survival benefit, leading to lower peak VO2 cut-off for heart transplantation. 14 Data from heart failure patients treated with new therapy, such as angiotensin receptor neprilysin inhibitor, need to be evaluated in the near future.
Atrial fibrillation
Atrial fibrillation is the most common arrhythmia in heart failure. It is usually associated with severe heart failure28 but does not directly affect prognosis. 29 Current guidelines recommend treatment with β-blockers for HFrEF patients, irrespective of rhythm disorders. 2 However, most heart failure patients included in clinical trials with β-blockers were in sinus rhythm, with only 11% to 35% of patients with atrial fibrillation, data on survival often being inconclusive. 30 A paper from the MECKI score database 31 pointed out that heart failure patients with permanent atrial fibrillation have a better outcome if treated with β-blockers. Moreover, the association between β-blockers and survival improvement was in parallel with daily β-blocker dose increase. The β1 selectivity versus non-selectivity for β-receptors did not influence patient survival. According to these results, a large nationwide Swedish registry 30 and a post hoc analysis of the AF‐CHF trial 32 revealed a significant reduction of all‐cause mortality in patients with heart failure and atrial fibrillation treated with β-blockers (a relative risk reduction of 25% and 28%, respectively).
β -blockers and heart failure prognosis over time
Since the pivotal classification of heart failure severity by Weber and Janicki, 33 peak VO2 has been proposed to identify patients with poor prognosis suitable for heart transplantation. 15 The initial value of 14 mL/kg/min was then reduced to 12 mL/kg/min for patients receiving β-blocker treatment.14,15 However, the heart failure population phenotype has significantly changed over time. Furthermore, since the first European heart failure guidelines published in 1997, the implementation of guidelines and the progressive increase in clinicians’ adherence to the recommendations definitely legitimated the cornerstone treatment for heart failure patients’ improving survival over time. 8 Therefore, while the increased use of β-blockers therapy in clinical practice significantly contributed to patients’ improved outcome, prognostic variables and relative cut-off values can result as misleading when applied for patients’ prognostication. Indeed, considering risk of morbidity/mortality for heart failure patients in different enrolment periods from 1993 to 2015, peak VO2 and VE/VCO2 slope cut-off values progressively decreased and increased, respectively, observing in more recent years values of 5 mL/min per kg and 57 for a 20% predictive risk. 34 Similar findings have been observed by Levy and Dardas, 35 showing a reduction of risk for the same peak VO2 when comparing heart failure patients from different periods. Accordingly, such important concerns would probably apply for heart failure scores and highlight how an update of risk parameters over time is mandatory, while their reliability, feasibility and reproducibility are yet unknown.
Conclusions
The MECKI Score Group was born with the aim of building an HFrEF prognostic score including CPET data, 3 working with the main focus on ‘heart failure and prognosis’ and confirming the prognostic power of the main CPET indexes (peak VO2,3,13 VE/VCO2,3,13 EOV, 16 VO2AT 5 ) without sex difference 21 and in the presence of common co-morbidities, such as anaemia 25 and renal insufficiency. 6 Notably, the HFrEF patients included in the MECKI score database were mostly treated with β-blockers therapy without differences between groups.
Lessons learned from MECKI score papers, specifically conceived for β-blockers evaluation, are reported in Table 1 and illustrated in Figure 1.
Lessons learned from MECKI score papers.
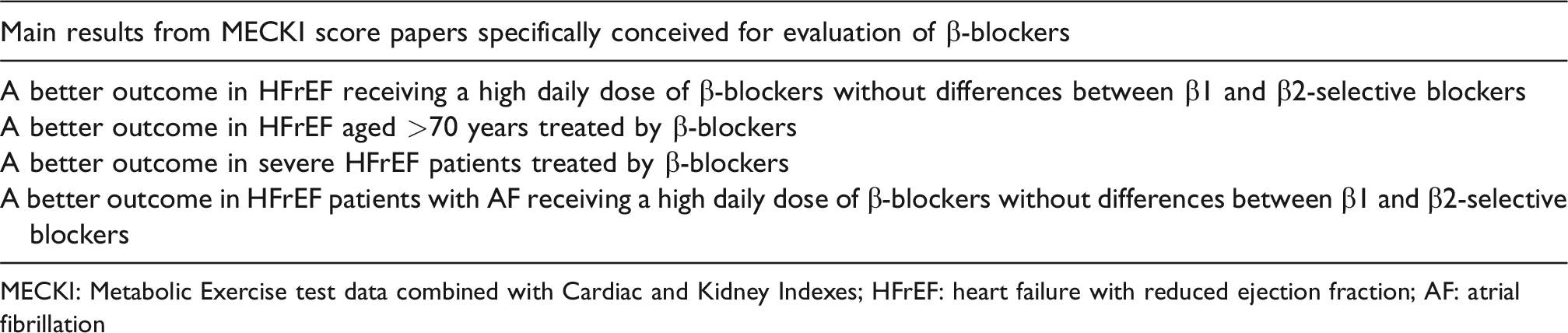
MECKI: Metabolic Exercise test data combined with Cardiac and Kidney Indexes; HFrEF: heart failure with reduced ejection fraction; AF: atrial fibrillation
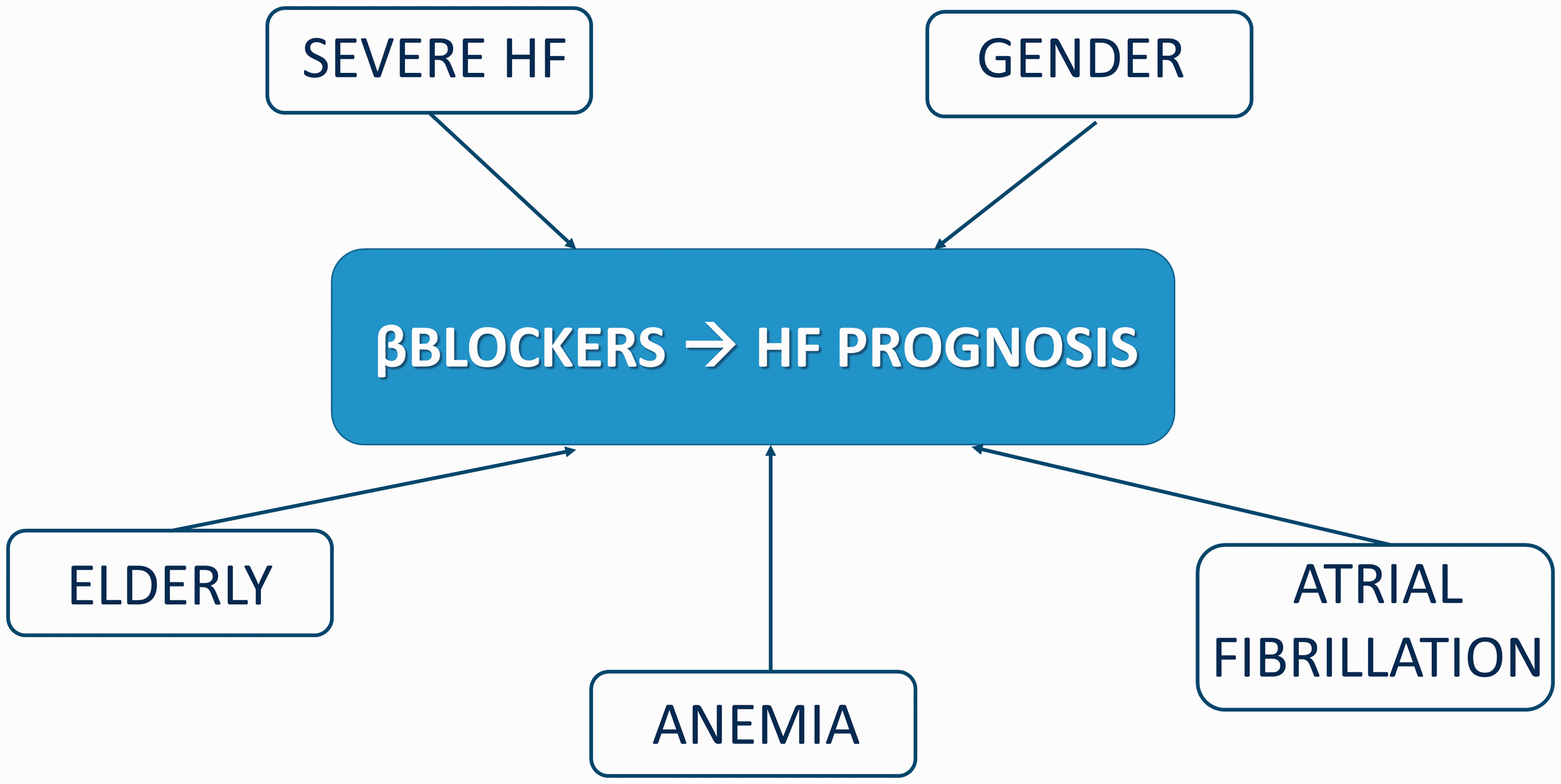
Association of β-blockers treatment with outcome evaluated in different settings by MECKI Score Group.
Choosing among β-blockers in heart failure patients according to β-receptors’ location and functions in the cardiopulmonary system is likely to be one of the more intriguing challenges in the future.
Footnotes
Author contribution
GC, GL, RB and MC contributed to the conception and the design of the work. All the authors drafted the manuscript, critically revised the manuscript and gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.