
Abstract
Background
Initial studies have suggested the familial clustering of mitral valve prolapse, but most of them were either community based among unselected individuals or applied non-specific diagnostic criteria. Therefore little is known about the familial distribution of mitral regurgitation in a referral-type population with a more severe mitral valve prolapse phenotype. The objective of this study was to evaluate the presence of familial mitral regurgitation in patients undergoing surgery for mitral valve prolapse, differentiating patients with Barlow's disease, Barlow forme fruste and fibro-elastic deficiency.
Methods
A total of 385 patients (62 ± 12 years, 63% men) who underwent surgery for mitral valve prolapse were contacted to assess cardiac family history systematically. Only the documented presence of mitral regurgitation was considered to define ‘familial mitral regurgitation’. In the probands, the aetiology of mitral valve prolapse was defined by surgical observations.
Results
A total of 107 (28%) probands were classified as having Barlow's disease, 85 (22%) as Barlow forme fruste and 193 (50%) patients as fibro-elastic deficiency. In total, 51 patients (13%) reported a clear family history for mitral regurgitation; these patients were significantly younger, more often diagnosed with Barlow's disease and also reported more sudden death in their family as compared with ‘sporadic mitral regurgitation’. In particular, ‘familial mitral regurgitation’ was reported in 28 patients with Barlow's disease (26%), 15 patients (8%) with fibro-elastic deficiency and eight (9%) with Barlow forme fruste (P < 0.001).
Conclusions
In a large cohort of patients operated for mitral valve prolapse, the self-reported prevalence of familial mitral regurgitation was 26% in patients with Barlow's disease and still 8% in patients with fibro-elastic deficiency, highlighting the importance of familial anamnesis and echocardiographic screening in all mitral valve prolapse patients.
Introduction
Mitral valve prolapse (MVP) affects 2–5% of the general population and is the most common cause of primary mitral regurgitation (MR). 1 The presence of MVP and MR may result in left ventricular (LV) dysfunction, heart failure, atrial fibrillation and less frequently sudden cardiac death. 1 Surgery is so far the only therapeutic option for MVP with severe MR and early diagnosis, and close monitoring of these patients is recommended to identify the most appropriate timing for operation.2,3 The underlying cause of MVP is unclear, but a genetic basis has been suggested by demonstrating familial clustering of this disease and by identifying few pathogenic genes.4–8 Familial screening of MVP patients may therefore represent an important tool to identify these patients at an early stage of the disease and to improve their management and risk stratification. However, collection of family history specific for valvular heart disease is not yet adopted in current practice and systematic family screening is rarely performed in these patients. This lack of awareness may be due to the limited evidence available so far, as studies evaluating the familial occurrence of MVP were either small and observational,4,7 or community based with a low overall prevalence of MVP and significant MR.5,6 Therefore, little is known about the actual prevalence of familial MR in a referral-type population with a severe MVP phenotype. Moreover, previous studies did not characterise the phenotype of familial MVP with complete echocardiographic analysis, although MVP presents with very different forms, such as Barlow's disease (BD), in which the whole valve is affected by excessive leaflet and annular abnormalities, or fibro-elastic deficiency (FED), in which the disease is limited to a single-scallop prolapse or flail. 9 Therefore, it has not been evaluated whether inheritance differs among BD as compared with FED, although they might have different aetiology. Accordingly, the aims of the present study were three-fold: (a) to evaluate the familial occurrence of MR based on self-reported family history in a large cohort of MVP patients with a severe phenotype requiring mitral valve surgery; (b) to assess whether familial occurrence is different for patients with BD compared with patients with FED; and (c) to evaluate the accuracy of self-reported family history.
Methods
Patient selection
All patients who underwent mitral valve surgery for severe MR due to MVP in our centre from 2000 to 2017 were identified. Patients with congenital valve disease, connective tissue disorder, endocarditis, rheumatic valve disease and non-ischaemic and ischaemic cardiomyopathy were excluded. Also, patients who died during follow-up were excluded, because their family history could not be retrospectively obtained. The remaining patients received a letter to ask permission to be contacted by phone; those who objected were excluded. The other patients were contacted and underwent a thorough structured interview on their cardiovascular family history. In case of a positive family history for valvular heart disease and/or in case of BD (considered in this study as most likely secondary to genetic or developmental alterations), patients were referred to the clinical geneticist. The study complies with the Declaration of Helsinki and was approved by the institutional review board and medical ethical committee. The medical ethical committee waived the need for written informed consent for collecting patient family history. If patients were referred to the clinical geneticist, written informed consent was obtained.
Clinical characteristics
Clinical data were collected from the departmental cardiology information system (EPD-Vision; Leiden University Medical Center, Leiden, The Netherlands). The aetiology of mitral valve disease was defined according to the surgical observations and patients were classified in three groups: 9 (a) FED, defined when thin leaflets or thickening limited to a single prolapsing mitral valve segment were observed, mostly with chordal rupture/flail; (b) BD, defined when bi-leaflet prolapse with generalised excess tissue, elongated chordae and severe annular dilatation were observed; (c) forme fruste (FF) Barlow, defined when myxomatous changes in more than one segment of a single leaflet were observed, and with moderate annular dilation. Other clinical data included demographics, cardiovascular risk factors, medication use and concomitant procedures at the time of mitral valve surgery.
Self-reported family history
To evaluate the familial prevalence and distribution of MR in MVP patients, cardiovascular family history was systematically obtained (see Supplementary file). First, the contacted patients (‘probands’) were asked whether they had any relatives known with MR. Only patients who were completely sure their relative had MR were classified as having ‘familial MR’. In order to apply only a very restrictive definition for familial MR, patients were classified as having ‘sporadic MR’ in case the family history was negative, unknown or if patients were unsure (e.g. if they only reported ‘valve regurgitation’ or ‘valve surgery’). Second, the presence of other cardiovascular disease in the family was asked: other valvular pathology, coronary artery disease (CAD), arrhythmias, cardiomyopathy, congenital heart disease, aortic pathology, cerebrovascular accident/transient ischaemic attack and unexplained sudden death (SD) at a young age (<65 years). Other valvular pathology was defined as valvular heart disease other than MR, or if the patient reported unspecified valvular pathology in the family. CAD was defined when myocardial infarction, prior percutaneous coronary intervention, coronary artery bypass grafting (CABG), or medical treatment for stable angina pectoris was reported in a relative younger than 65 years. The presence of arrhythmias in a relative was defined in the case of specific treatment for either atrial or ventricular arrhythmias (e.g. medications or implantable cardiac defibrillator). Family history was considered positive for cardiomyopathy only if the proband could report a specific diagnosed cardiomyopathy. Aortic pathology included reported aortic aneurysms/dissections. SD was defined as unforeseen and unexplained SD in a relative less than 65 years. For all reported cardiac diseases, the relation of the affected relative to the proband was noted.
Genetic consultation and evaluation of affected relatives
The probands who were referred to the clinical geneticist underwent consultation according to standard practice. The family history was reviewed in detail and a pedigree was constructed. If the patient reported any relevant cardiac family history, the involved relative was asked for consent to retrieve their medical information in order to confirm the exact diagnosis. Familial MR was defined in a relative if the echocardiographic report was available and described MR of grade 2 or greater and/or a specific description of primary MR, such as BD, FED or MVP in general. The pedigrees were also evaluated to suggest possible patterns of inheritance. However, considering the lack of data on the penetrance of primary MR and the incomplete familial screening, no definite conclusions could be drawn.
Echocardiography
Standard transthoracic echocardiography was performed in all probands before operation with a commercially available ultrasound device (Vivid 5, Vivid 7 and E9; GE-Vingmed, Milwaukee, WI, USA). Left atrial (LA) diameter and LV dimensions were acquired from the parasternal long-axis view. LV volumes, left ventricular ejection fraction (LVEF) and LA volumes were measured using the Simpson method and indexed for body surface area. 10 MVP was defined based on the Carpentier classification, and the severity of MR was quantitatively assessed using a multiparametric approach. Systolic pulmonary artery pressure (sPAP) was estimated from the tricuspid regurgitant jet velocity as recommended. 11 Image analysis was performed with EchoPAC (version 112; GE Medical Systems, Horten, Norway).
Statistical analysis
Continuous variables are presented as mean ± standard deviation, when normally distributed and as median (interquartile range) when not normally distributed. Categorical variables are expressed as absolute numbers and percentages. Differences in clinical and echocardiographic characteristics between patients with familial MR and sporadic MR were assessed using Student's t-test, the Mann–Whitney U test or chi-square test, when appropriate. The agreement between self-reported and confirmed family history was assessed with Cohen's kappa. Statistical analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). A P value less than 0.05 was considered statistically significant.
Results
Patient population
A total of 385 patients (62 ± 12 years, 63% men) were included for final analysis from a cohort of 693 patients who underwent surgery for severe primary MR between 2000 and 2017 (Figure 1). A total of 185 patients were excluded because they died, 92 patients declined to participate and 31 could not be contacted. Based on the surgical observations, 193 (50%) patients were diagnosed with FED, 107 (28%) with BD and 85 (22%) with FF Barlow (Table 1).
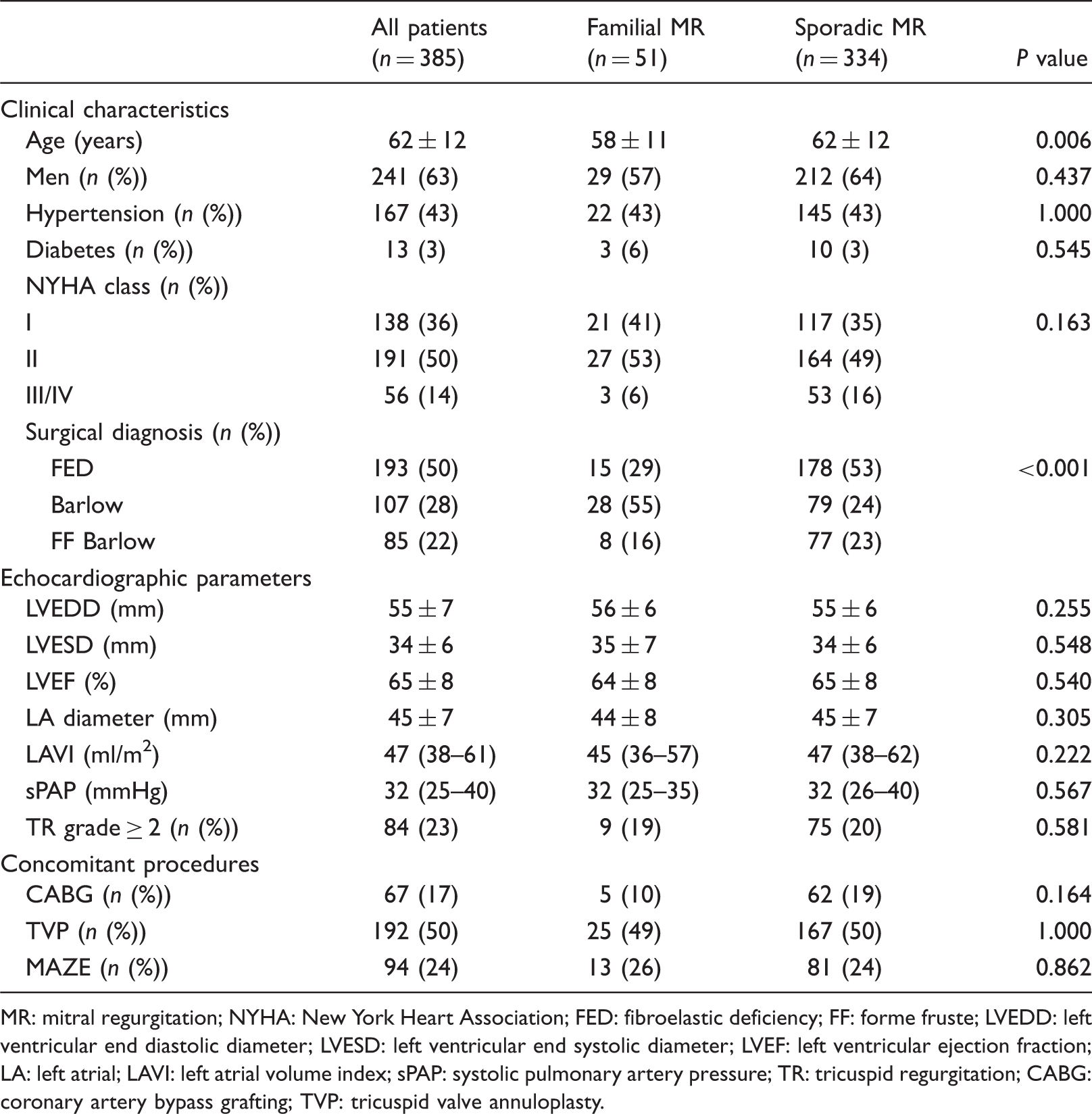
Flow-chart of patient selection. BD: Barlow's disease; FED: fibro-elastic deficiency; MR: mitral regurgitation; MV: Mitral valve; MVP: Mitral valve prolapse. Clinical and echocardiographic characteristics of patients with and without self-reported familial primary mitral regurgitation. MR: mitral regurgitation; NYHA: New York Heart Association; FED: fibroelastic deficiency; FF: forme fruste; LVEDD: left ventricular end diastolic diameter; LVESD: left ventricular end systolic diameter; LVEF: left ventricular ejection fraction; LA: left atrial; LAVI: left atrial volume index; sPAP: systolic pulmonary artery pressure; TR: tricuspid regurgitation; CABG: coronary artery bypass grafting; TVP: tricuspid valve annuloplasty.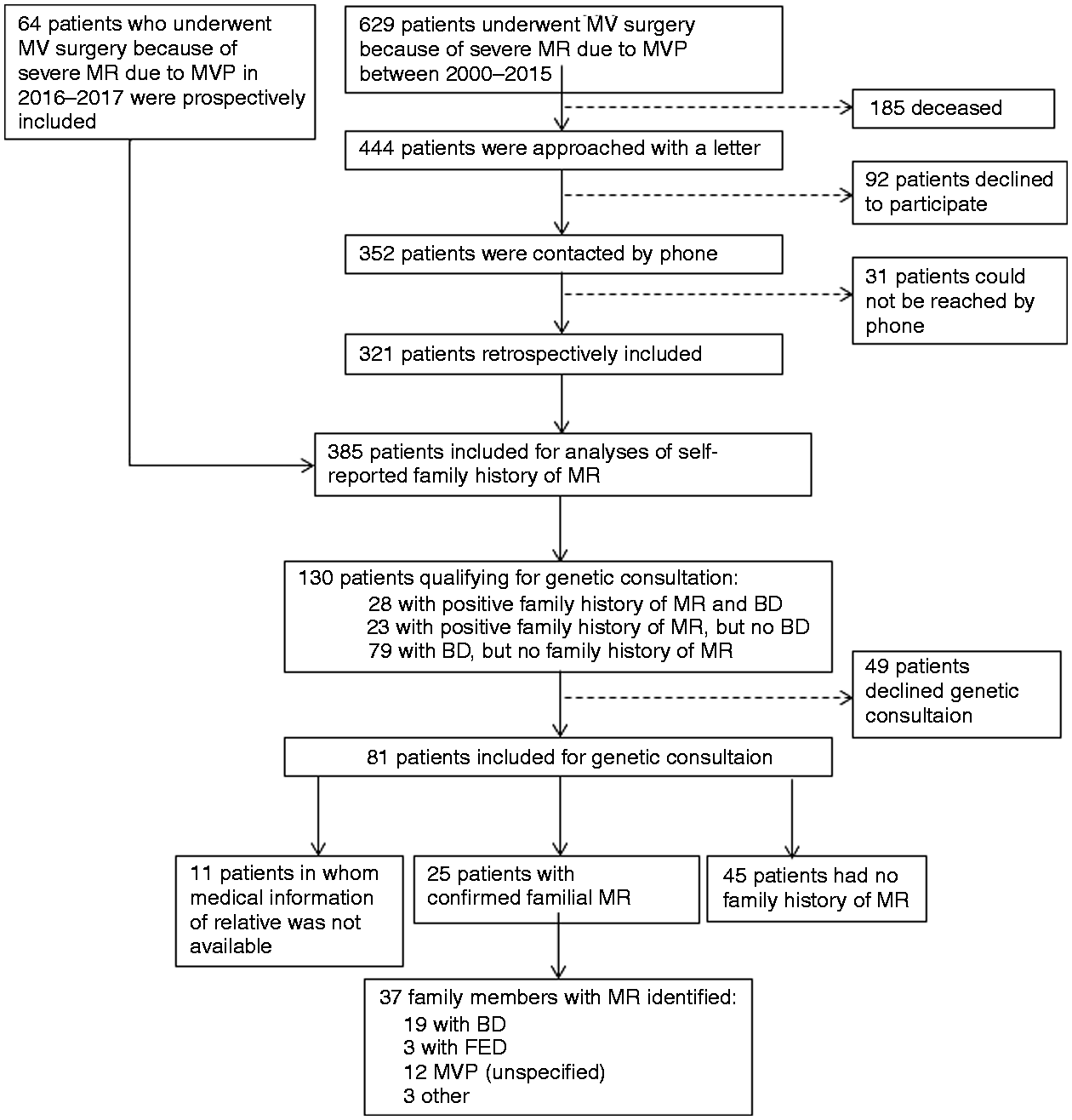
Prevalence of familial MR and family history of other cardiovascular disease in MVP patients
A self-reported family history of MR was positive in 51 MVP patients (13%). Table 1 shows the clinical and echocardiographic characteristics of patients with familial MR as compared with patients with sporadic MR. No differences between the two groups were observed regarding cardiovascular risk factors, concomitant surgical procedures and echocardiographic parameters. However, patients with familial MR were significantly younger and more often diagnosed with BD (55%) compared with patients with sporadic MR (24%). Figure 2(a) presents the prevalence of familial MR per MR aetiology and shows that patients with BD more often reported a positive family history (26% vs. 8% in FED and 9% in FF Barlow patients, P < 0.001). In Figure 2(b) the self-reported prevalence of other cardiovascular diseases is presented. No differences were observed between patients with familial MR and with sporadic MR regarding most diseases; however, SD in family members less than 65 years of age was significantly more frequent in patients with familial MR (29% vs. 14%, P = 0.007). No significant differences were observed when comparing the prevalence of SD per MR aetiology: 20% of BD patients reported unexplained SD under 65 years of age versus 14% of FF Barlow and FED patients (P = 0.29).
(a) Prevalence of self-reported familial mitral regurgitation (MR) among different MR aetiologies. (b) Prevalence of family history of other cardiovascular disease in all patients and compared between patients with familial MR and sporadic MR.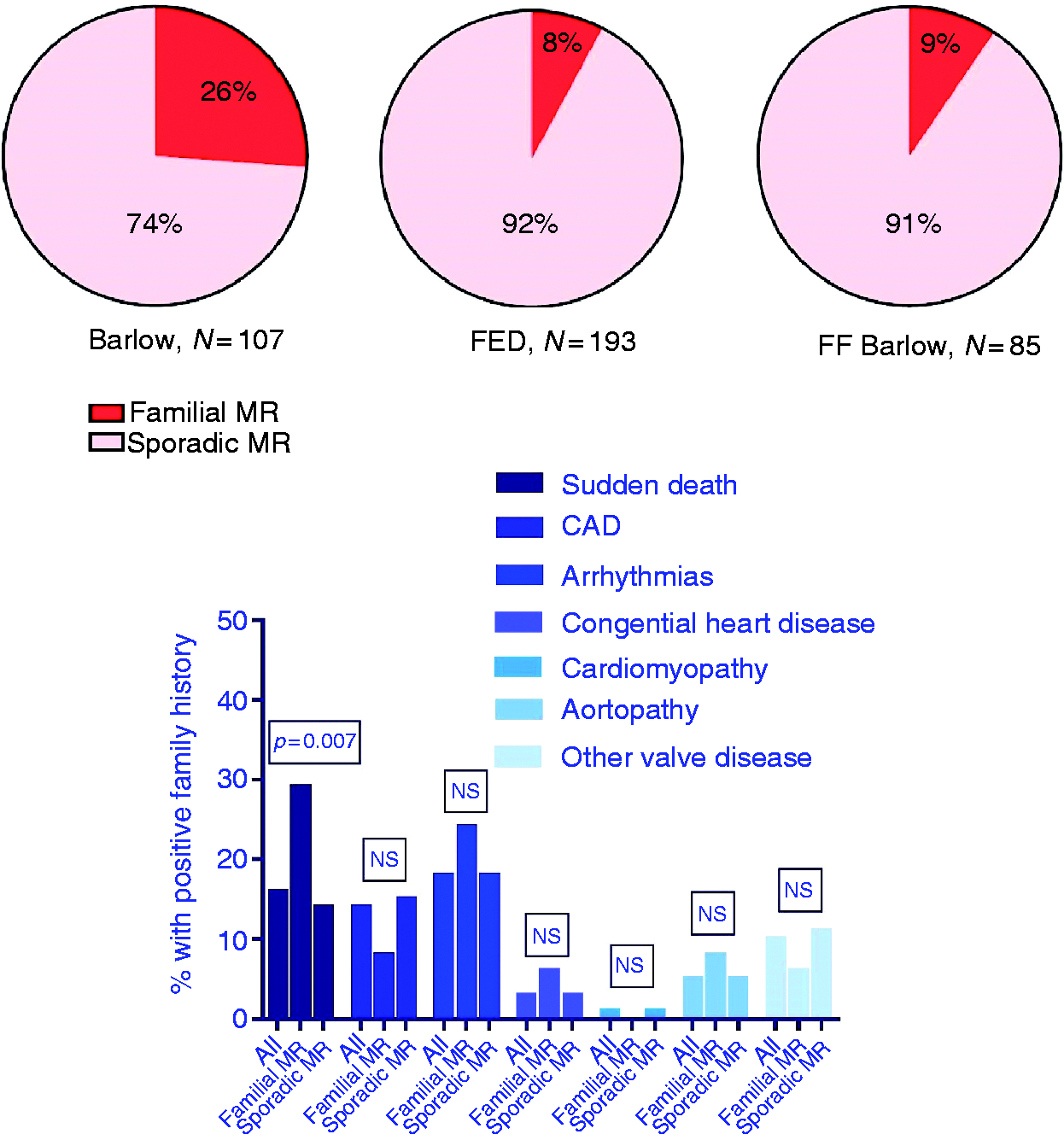
Confirmed familial MR by clinical geneticist
A total of 81 probands were referred for genetic consultation (Figure 1). Of those, 36 had a positive family history of MR (15 patients with a positive family history of MR declined genetic consultation) and the remaining 45 probands did not report familial MR, but were referred because of BD. For 11 relatives who were reported by the probands to have MR, this could not be confirmed, because the information was no longer available (n = 4) or because consent was not obtained from the affected relative (n = 7). Eventually, the presence of primary MR was confirmed by echocardiographic and/or surgical reports in 37 relatives from 25 different probands. In 19 (52%) relatives the echocardiographic report described the presence of BD, while in three (8%) relatives FED and in 12 (32%) relatives a MVP (not further defined) was reported. In three relatives the aetiology was not completely clear (i.e. calcified mitral valve with significant MR). Interestingly, different aetiologies of MR were observed within the same family. In particular, for 10 relatives (53%) with BD, the diagnosis of the proband was discordant (i.e. FED).
Patterns of inheritance
For the 36 probands with familial MR who were referred to the clinical geneticist, the pedigrees were evaluated and suggested different possible patterns of inheritance. Figure 3 shows examples of pedigrees from the study cohort with a different distribution of affected family members.
Pedigrees from different families with a different distribution of affected family members. (a) Affected men and women in two generations; (b) two brothers and a sister affected; (c) three affected brothers; (d) mother and two sons and one daughter affected; (e) mother and both of her children, daughter and son, affected: both mother and daughter show severe mitral valve prolapse at echocardiography.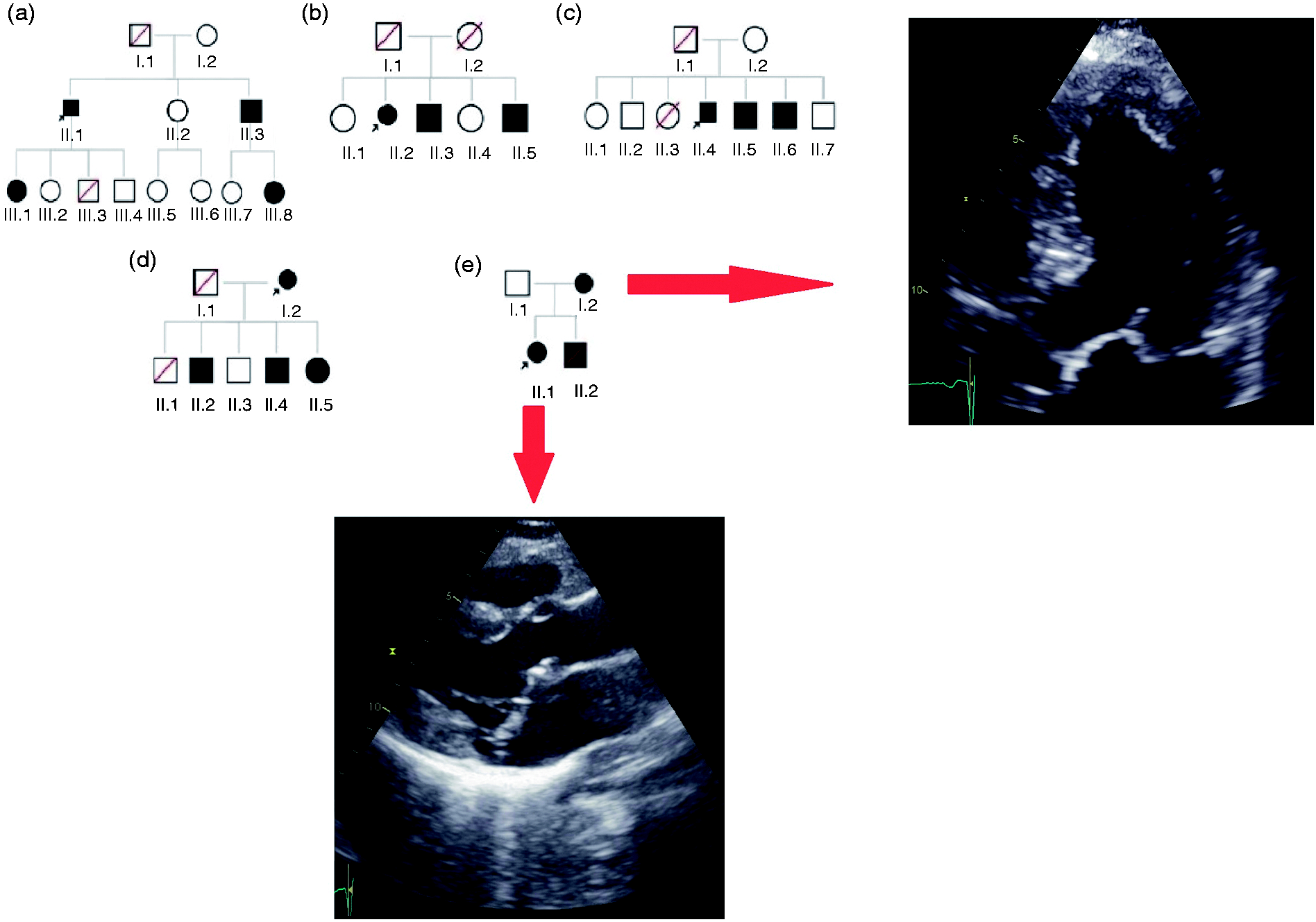
Accuracy of self-reported family history
Medical information was received from 37 relatives who were reported by the probands to have primary MR. In 34 of these patients, a diagnosis of primary MR was confirmed by the echocardiographic or surgical report. In three relatives, primary MR could not be confirmed due to: a functional MR secondary to LV dilatation (n = 2); no clear prolapse or MR but a sclerotic mitral valve in the context of an aortic valve replacement (n = 1).
Furthermore, during the genetic consultation three more relatives appeared to be affected but were not reported during the first contact with the proband. In all of these three relatives, the presence of primary MR was confirmed. The agreement of self-reported and confirmed family history was therefore overall good with κ=0.80, P < 0.001.
Discussion
The main results of the present study can be summarised as follows: (a) In a large cohort of patients who underwent mitral valve surgery because of severe MR due to MVP, the prevalence of self-reported familial MR was 26% in patients with BD and 8% in patients with FED; (b) patients with familial MR were younger as compared with patients with sporadic MR and also more frequently reported SD in their family; (c) a self-reported family history of primary MR showed good agreement with the assessment during genetic counselling.
Heritability of MVP and MR
MVP is a relatively common valve abnormality and its heritability was already suggested in 1966 by Hancock and Cohn, who observed a systolic click and murmur in multiple relatives from different families. 12 Since then, other studies have demonstrated the familial clustering of MVP.4–8 In 1982, Devereux et al. 4 evaluated 45 probands and 179 first degree relatives, and using M-mode echocardiography found MVP in 30% of them. In two large community-based studies by the group of Delling and colleagues5,6 familial clustering of MR was demonstrated in non-selected individuals, and the authors showed that familial MVP was associated with a higher prevalence of MVP and MVP-related MR in the offspring. These studies also suggested a higher heritability of MVP based on the severity of the disease, with a magnitude comparable with other complex diseases such as CAD and atrial fibrillation, and advocated the need for further studies in a referral-type population with more severe phenotype. Therefore, the present study evaluated the self-reported family history in a large referral-type population of patients requiring mitral valve surgery and demonstrated that familial clustering is also present in this cohort. In the past years, several genetic studies were also performed in patients with familial MR due to MVP and identified three possible loci for autosomal-dominant MVP on chromosomes 16 (MMVP1), 11 (MMVP2) and 13 (MMVP3).13–15 Furthermore, DCHS1 and PLD1 have been linked to autosomal MVP16,17 and mutations in the filamin A (FLNA) gene have been identified to cause a X-linked form of MVP. 18 In line with these findings, the present study observed different distributions of affected family members between families (Figure 3). However, no final conclusions regarding the pattern of inheritance could be drawn, because 100% penetrance is unlikely and the familial screening was not complete.
Differences in familial MR between BD and FED
Previous studies evaluating the heritability and familial distribution of MVP mainly distinguished the presence of MVP from the non-diagnostic morphology of MVP, as a prodromal phenotype of the disease. However, these studies did not explore the difference in heritability between different aetiologies of MVP, such as BD and FED. It is well known that BD and FED differ in many characteristics, such as age of diagnosis, clinical presentation and morphology of the valve, suggesting different pathophysiological mechanisms. 9 Differences in heritability are therefore plausible among these phenotypes, considering also recent findings suggesting that mitral valve abnormalities in BD might be secondary to developmental alterations at the annular junction and leaflets. 19
The present study showed a significantly higher prevalence of familial MR in BD patients (26%), but still a prevalence of 8% familial MR in FED and of 9% in FF Barlow. Interestingly, when studying the phenotype of MVP within families, patients with FED and BD were observed within the same family, suggesting that in some cases more limited involvement of the mitral valve might be a form of the mild phenotype of the same disease, although it might be confused with FED when based on an echocardiographic morphological definition (such as the single scallop involvement). These findings suggest that although BD is associated with a higher magnitude of heritability, a thorough family history should also be performed in patients with FED and FF Barlow, and more in-depth studies on the morphological characteristics of familial MR in MVP should be performed.
Family history of other cardiovascular disease
It has been reported that MVP may be associated with other cardiovascular diseases, such as cardiomyopathies, congenital heart disease, CAD, ventricular arrhythmias and sudden cardiac death.1,2 Therefore, the present study aimed at collecting a complete family history also including other cardiovascular diseases. No differences were observed for most cardiovascular diseases when comparing familial versus sporadic MR. However, 29% of patients with familial MR, compared with 14% in patients with sporadic MR, reported SD at less than 65 years of age in their family. Previous studies showed that MVP is significantly associated with sudden cardiac death in young adults, especially in women, and that specific characteristics, such as fibrosis of the papillary muscle and mitral annular disjunction, were associated with ventricular arrhythmias.20–23 In the present study, additional information about the relatives who experienced SD was lacking and it is therefore unknown whether SD was of cardiac origin and whether they also had MVP; however, the fact that SD was more prevalent in patients with familial MR underlines the importance of the better characterisation of these patients and of obtaining an extensive family history in MVP patients.
Clinical implications
The present study showed that familial MR is a common finding in a large cohort of patients who underwent mitral valve surgery for severe MR due to MVP, and should be considered regardless of the aetiology of primary MR. Familial screening for MVP and MR is currently seldom performed, but it could represent an important tool for early diagnosis and therefore strict monitoring of the relatives. This approach might be helpful considering the increasing evidence that patients benefit the most from mitral valve surgery when LV function is still preserved and symptoms have not yet occurred,24,25 and also to improve risk stratification for sudden cardiac death in this patient population. However, further studies are needed to demonstrate the cost-effectiveness of family screening in MVP. The present study also showed that clinicians can rely with sufficient confidence on the family information the patient provides, at least about the first degree affected relatives (positive family history). Therefore, the present study strongly suggests to collect family history as part of standard clinical practice in MVP. In turn, the value of self-reported negative family history could not be evaluated in the present study, because a systematic screening with echocardiography was not performed in all relatives.
Limitations
The present study has several limitations that should be mentioned. First, self-reported family history was used to estimate familial distribution, and the accuracy of this information can vary because not all patients are aware of the medical histories of their relatives and it is more susceptible to ascertainment bias. However, the importance of family history has been recognised for several other (cardiac) diseases and has been shown to be reliable at least in first-degree relatives.26–28 Also for the family history of other cardiovascular diseases, recall bias might exist in a family, as patients with already known familial MR might be more aware of other cardiac diseases in their family. However, this bias was minimised by asking the cardiac family history systematically and thoroughly in all patients. Second, patients who died after the operation or refused to participate were excluded; whether excluding these patients might influence the results cannot be proved. Also, non-diagnostic morphologies of MVP were not systematically evaluated, 6 as probands were by definition characterised by a severe phenotype and not all family members were screened with echocardiography (only when they gave consent). Because of the aforementioned limitations and the strict definition applied, the prevalence shown in this study is probably underestimated. A systematic echocardiographic screening of all family members is needed to assess the real prevalence and to identify characteristics associated with familial MR.
Conclusion
In a large cohort of patients operated for MVP with severe MR, a significant prevalence of self-reported familial MR was observed, reaching 30% in patients with BD and almost 10% in patients with FED. Familial MR was also associated with a higher incidence of SD. A self-reported family history of MVP is reliable and can be used by physicians to perform further family screening.
Supplemental Material
Supplemental material for Familial occurrence of mitral regurgitation in patients with mitral valve prolapse undergoing mitral valve surgery
Supplemental Material for Familial occurrence of mitral regurgitation in patients with mitral valve prolapse undergoing mitral valve surgery by Yasmine L Hiemstra, Aniek L van Wijngaarden, Mathilde W Bos, Martin J Schalij, Robert JM Klautz, Jeroen J Bax, Victoria Delgado, Daniela QCM Barge-Schaapveld and Nina Ajmone Marsan in European Journal of Preventive Cardiology
Footnotes
Author contribution
All authors contributed to the conception and design of the study. YLH, ALW, MWB, DQCMBS and NAM contributed to acquisition of the data. YLH and NAM analysed the data, all authors contributed to interpretation of the data. Drafting of the manuscript was done by YLH, DQCMBS and NAM, the manuscript was critically revised by JJB and VD. Finally, all authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VD received consulting fees from Abbott Vascular. The Department of Cardiology of Leiden University Medical Centre received research grants from Biotronik, Medtronic, Boston Scientific and Edwards Lifesciences.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.