
Abstract
Background
The prognostic effect of multi-component cardiac rehabilitation (CR) in the modern era of statins and acute revascularisation remains controversial. Focusing on actual clinical practice, the aim was to evaluate the effect of CR on total mortality and other clinical endpoints after an acute coronary event.
Design
Structured review and meta-analysis.
Methods
Randomised controlled trials (RCTs), retrospective controlled cohort studies (rCCSs) and prospective controlled cohort studies (pCCSs) evaluating patients after acute coronary syndrome (ACS), coronary artery bypass grafting (CABG) or mixed populations with coronary artery disease (CAD) were included, provided the index event was in 1995 or later.
Results
Out of n = 18,534 abstracts, 25 studies were identified for final evaluation (RCT: n = 1; pCCS: n = 7; rCCS: n = 17), including n = 219,702 patients (after ACS: n = 46,338; after CABG: n = 14,583; mixed populations: n = 158,781; mean follow-up: 40 months). Heterogeneity in design, biometrical assessment of results and potential confounders was evident. CCSs evaluating ACS patients showed a significantly reduced mortality for CR participants (pCCS: hazard ratio (HR) 0.37, 95% confidence interval (CI) 0.20–0.69; rCCS: HR 0.64, 95% CI 0.49–0.84; odds ratio 0.20, 95% CI 0.08–0.48), but the single RCT fulfilling Cardiac Rehabilitation Outcome Study (CROS) inclusion criteria showed neutral results. CR participation was also associated with reduced mortality after CABG (rCCS: HR 0.62, 95% CI 0.54–0.70) and in mixed CAD populations.
Conclusions
CR participation after ACS and CABG is associated with reduced mortality even in the modern era of CAD treatment. However, the heterogeneity of study designs and CR programmes highlights the need for defining internationally accepted standards in CR delivery and scientific evaluation.
Keywords
Introduction
Although several recent studies, meta-analyses1–11 and recommendations of national and international guidelines12,13 suggest a beneficial effect of cardiac rehabilitation (CR) in patients with coronary artery disease (CAD), considerable scientific doubt is still apparent for the following reasons:
The type of CR offered varies considerably between and within the countries with respect to content, duration, intensity and volume, and worldwide there are no accepted minimal standards for judging the quality of CR delivery, thereby leaving doubt as to the effectiveness of CR as delivered in routine clinical practice.14,15 Developments within the past 20 years, including interventional therapies, surgery and medications, have had a large impact on the quality of care delivered to patients who are participating in modern CR.16,17 On this basis, older studies evaluating the effect of CR are no longer suitable for estimating CR effectiveness. In some countries, high levels of CR participation supported by government policy, health insurance, pension funds and ethical criteria make it virtually impossible to randomise patients out of CR, and large prospective randomised trials on CR efficacy with experimental and highly reproducible designs are scarce.18–20 However, alternative robust research designs using routine clinical data captured through cohort studies, observational studies and registries have been published with findings that are worthy of consideration.3,4–9,21
For these reasons, the present study sought to assess the actual evidence of CR’s effectiveness by focusing on CAD patients after a recent cardiac event (acute coronary syndrome (ACS), coronary artery bypass grafting (CABG) or mixed populations also including patients with stable CAD) and treated in the era of acute revascularisation during ACS and routine medication with statins. Furthermore, in order to better reflect clinical practice, apart from randomised controlled trials (RCTs), controlled cohort studies (CCSs) were also included in the meta-analysis.
Methods
This systematic review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) statement (see also Supplemental Material, Table SM 5).22,23 The study protocol was prospectively published in PROSPERO International prospective register of systematic reviews (University of York, Centre for Reviews and Dissemination) and verified as original (CRD42014007084).
Study eligibility criteria
The study selection criteria (populations, interventions, controls, outcomes and designs) are outlined in detail in Table 1. Three groups of patients were defined:
patients after hospitalisation for ACS, including ST-elevation myocardial infarction (STEMI), non-STEMI (NSTEMI) or unstable angina pectoris (UAP); patients after hospitalisation for CABG; mixed populations including patients after ACS and/or after CABG as a basic requirement, but also including patients with chronic stable CAD with or without elective percutaneous coronary intervention (PCI). Cardiac Rehabilitation Outcome Study inclusion criteria. Studies including patients before and after 1995 were only included into the analysis, if the vast majority of patients was treated in 1995 or later. CR: cardiac rehabilitation; CROS: Cardiac Rehabilitation Outcome Study.
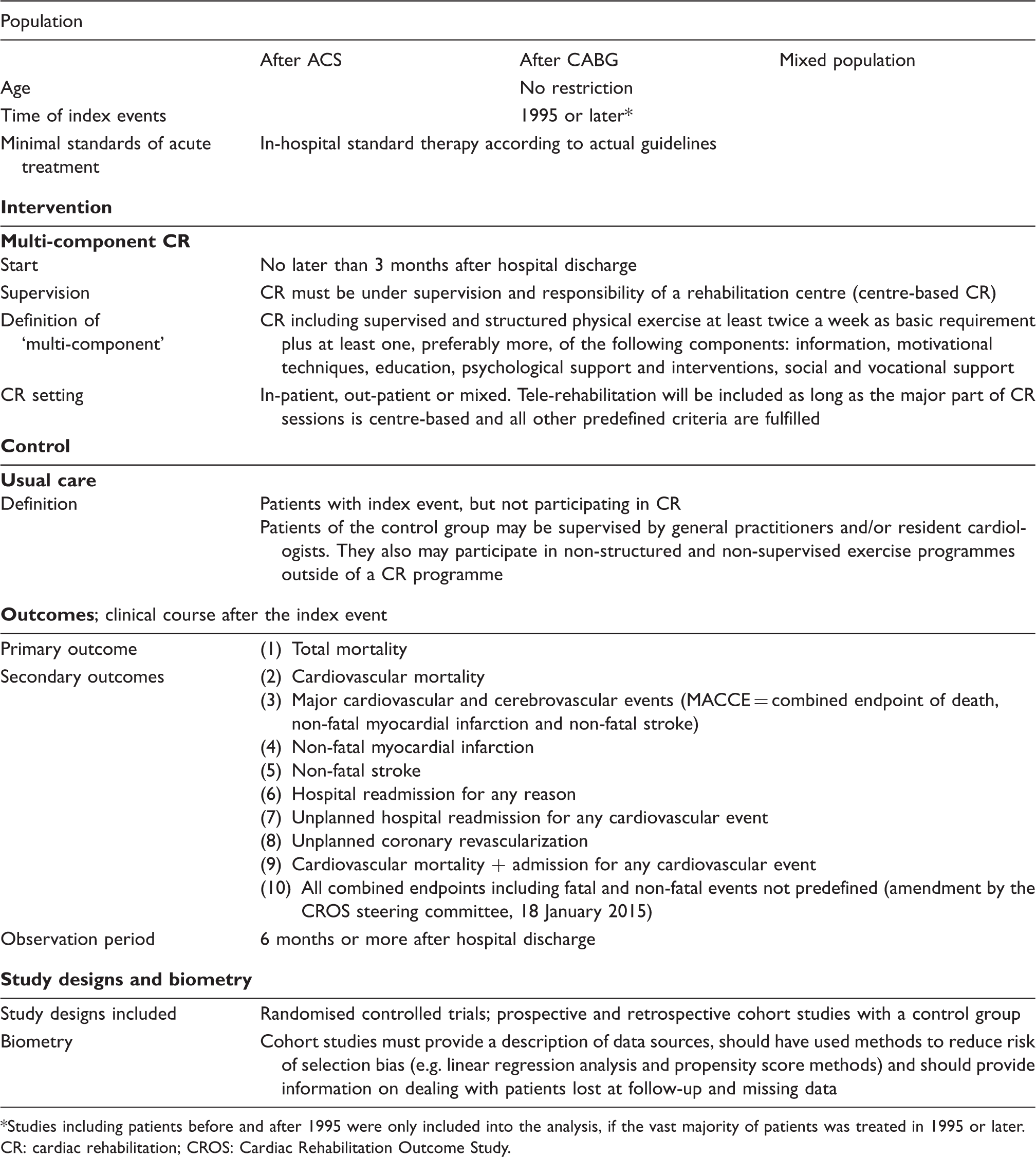
To guarantee current CAD treatment standards (operationally defined by the Cardiac Rehabilitation Outcome Study (CROS) as revascularisation for acute myocardial infarction (AMI) and routine use of statins), only studies that recruited patients in 1995 or later were included. Total mortality was the primary endpoint. Predefined secondary endpoints are outlined in Table 1 and primarily include non-fatal cardiovascular events, hospital readmissions and mixed endpoints.
Search methods and identification of studies
Highly sensitive search strategies were developed by a graduate information scientist (MIM) for seven databases in order to identify two types of studies: RCTs and CCSs, regardless of the studies’ current status (published, unpublished, finished or ongoing). For developing the search strategy, candidate terms were identified (text words and controlled vocabulary) by using a multi-stranded approach. Known key literature and the publications included in two systematic reviews on the same topic were assessed.24,25 Fifty abstracts retrieved from PubMed using the Medical Subject Heading (MeSH) ‘myocardial infarction/rehabilitation’ were evaluated. All MeSH terms belonging to ‘heart diseases ‘and ‘rehabilitation ‘were reviewed. Afterwards, search blocks on two concepts were built: ‘myocardial infarction ‘and ‘coronary bypass’ for the population of interest, and ‘rehabilitation’ as the intervention under evaluation. These were then combined with validated methodological search filters for the two included study types.
The search strategy was elaborated for PubMed and subsequently peer-reviewed by an independent, external information specialist (Margaret Sampson, Children's Hospital of Eastern Ontario, USA). After revisions resulting from this quality assurance process, the strategy was adapted to the specific requirements of each database (syntax, search options and controlled vocabulary). If validated search filters were not available, filters were developed for databases where filtering seemed reasonable.
Starting with the year 1995, the following bibliographic databases were used with no restriction on language: PubMed, Embase, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS) and Center for International Rehabilitation Research Information and Exchange (CIRRIE). Additionally, unpublished or ongoing studies were searched using the World Health Organization’s International Clinical Trials Registry Platform (ICTRP), a meta-register of trials including 16 primary trial registers of different countries. The search was originally run in December 2013, and thereafter updated in April 2015 and again in 22 December 2015. The details of all search strategies are documented in the Supplemental Material (Table SM 1). The only difference between the protocol and this review was the exclusion of the databases Current Contents Medicine (CC MED) and Web of Science due to the limited benefits they were judged to provide.
Study selection
The selection process is outlined in Figure 1. All references (titles plus abstracts) were independently evaluated by three members of the CROS study group (BR, CHD and PD, the ‘reference selection board’) using an algorithm that guaranteed the independent evaluation of each title by at least two of these experts. In addition, the references of recent meta-analyses and potentially eligible studies were screened. This primary selection (PS) process was finalised by consensus within the reference selection board, resulting in n = 243 abstracts of potential interest. By re-evaluating these abstracts, n = 67 publications were selected for full-text evaluation, resulting in n = 39 publications being selected for a structured study evaluation (SSE). SSE was performed and consented within an extended reference selection board (BR, CHD, PD, AS and HV), including two biometricians (DS and KJ). In four publications, descriptions of the CR characteristics remained incomplete despite contacting the authors for clarification (see Tables 2 and 4a). Incomplete description of CR characteristics did not lead to study exclusion by decision of the reference selection board, provided the other inclusion criteria were fulfilled. On the basis of the SSE process, 25 studies remained for meta-analysis. The primary reasons for study exclusion at the PS level are given in Supplementary material Table SM 2. Table SM 2 also includes studies of potential interest that were not published at the closure of the CROS literature search.
Study selection flow chart. Studies selected for quantitative analysis; baseline study characteristics and overall results. Descriptive values of metric variables are given in mean or mean plus SD, if applicable. Other calculations are noted in the table. Mdn: median; N: number of total population, n: number of subpopulation; na: not applicable (not published); min: minute(s); h: hour(s); d: day(s); wk: week(s); mo: month(s); y: year(s). AMI: acute myocardial infarction; AP: angina pectoris; CABG: coronary artery bypass grafting; CAD: coronary artery disease; CHF: congestive heart failure; CI: confidence interval; CR: cardiac rehabilitation; CSS: controlled cohort study; EF: ejection fraction; EP: endpoint; HD: haemodialysis; HR: hazard ratio; HREA: hospital readmission for any reason; IG: intervention group; ITT: intention to treat; MACE: major adverse cardiac events (death and non-fatal re-infarction); MACCE: major adverse cardiac and cerebrovascular events (death, non-fatal re-infarction and stroke); NSTEMI: non-ST-elevation myocardial infarction; pCCS: prospective controlled cohort study; PCI: percutaneous coronary intervention; PEP: primary endpoint; rCCS: retrospective controlled cohort study; RCT: randomised controlled trial; RR: risk ratio; SEP: secondary endpoint; SMC-CR: structured and multi-component cardiac rehabilitation; STEMI: ST-elevation myocardial infarction; UC: usual care including ambulatory supervision by family doctor and/or cardiologist, and may also include advice to exercise at home. Summary of results. ACS: acute coronary syndrome; CABG: coronary artery bypass grafting; NO: sum of events has not been calculated, if one study of a specific subgroup did not report the number of events; MH: Mantel–Haenszel pooling; NA: not applicable; IV: inverse variance pooling; RCT: randomised controlled trial; rCCS: retrospective controlled cohort study; pCCS: prospective controlled cohort study; HR: hazard ratio; CI: confidence interval; OR: odds ratio. Quality evaluation of cohort studies included into meta-analysis.26,35 Outcomes under investigation: the numbers refer to the predefined outcomes as outlined in Table 1. Confounding domains as specified by CROS: 1, age; 2, gender; 3, smoker; 4, diabetes; 5, history of stroke; 6, history of acute myocardial infarction; 7, reduced left ventricular ejection fraction; 8, acute/early percutaneous coronary intervention during acute myocardial infarction. Biometrical methods to manage confounding: (a) multivariable regression analysis; (b) propensity score matching; (c) propensity score-adjusted multivariable regression analysis; (d) confounders described; (e) retrospective matched pairs. Adjusting only for age and gender has been regarded as insufficient for the limitation of confounding. APPROACH: Alberta Provincial Project for Outcomes Assessment in Coronary Heart Disease; NACRP: Northern Alberta Cardiac Rehabilitation Program; FRENA: Risk Factors and Arterial Disease registry (Factores de Riesgo y ENfermedad Arterial); OMEGA: Randomized, Placebo-Controlled Trial to Test the Effect of Highly Purified Omega-3 Fatty Acids on Top of Modern Guideline-Adjusted Therapy after Myocardial Infarction; DepreMI: Depression after Myocardial Infarction study; MIND-IT: Myocardial Infarction and Depression Intervention Trial.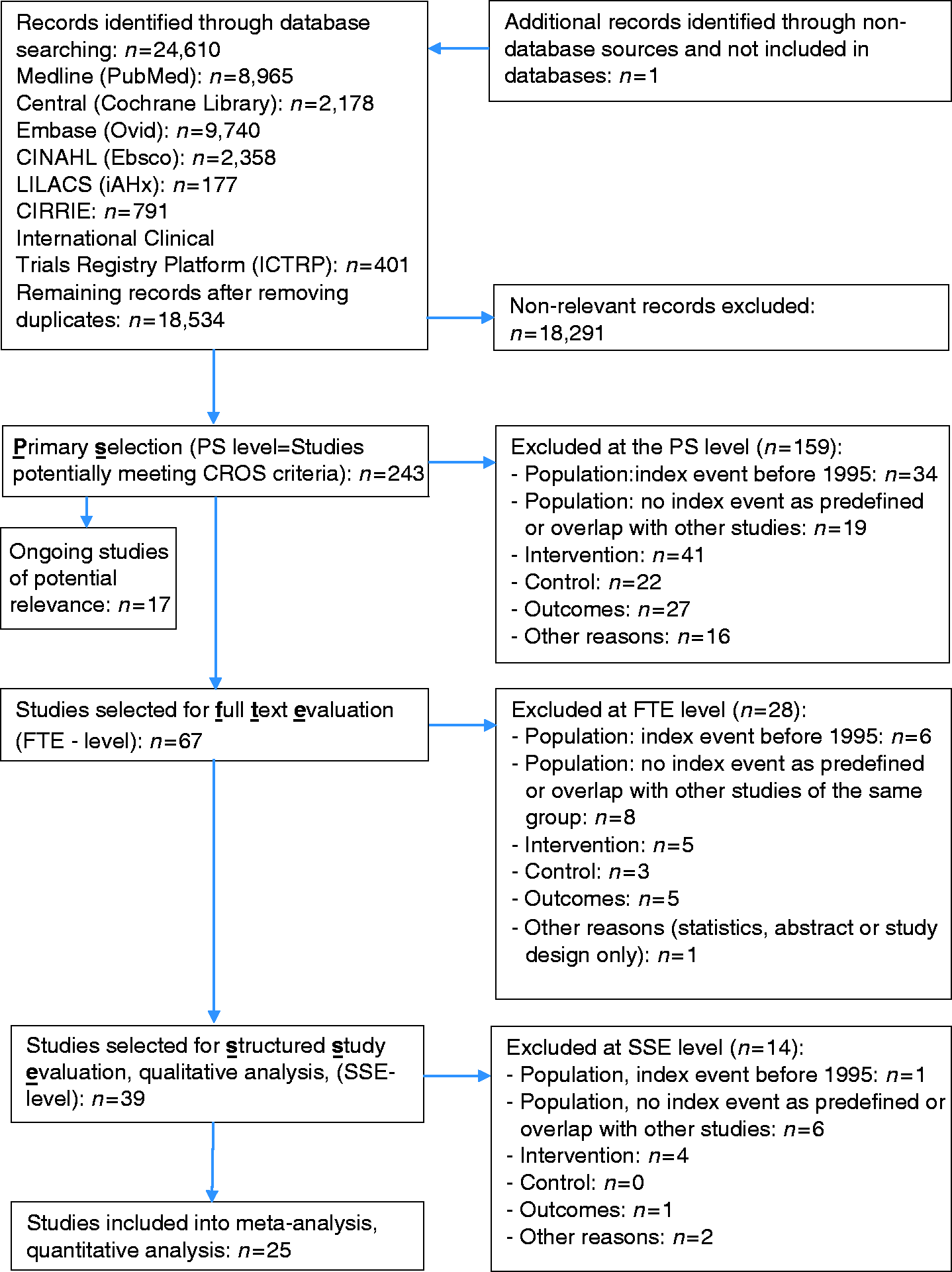



Study evaluation process
The study evaluation included design, data sources, information on populations, interventions, controls, calculation and presentation of outcomes and handling of bias. For RCTs, the Cochrane risk of bias table (http://tech.cochrane.org/revman/download) was used, and for the CCSs, the checklists of methodological issues on non-randomised studies 26 and the Newcastle–Ottawa Scale (NOS) were used. 27 In order to facilitate the study evaluation with respect to the management of confounding, n = 8 potential confounders were prespecified, including age, gender, smoker, diabetes, history of stroke, history of AMI, reduced left ventricular ejection fraction and acute or early PCI during AMI.
Data extraction
The following data were extracted from the studies that were selected for meta-analysis: name of first author, year of publication, study location (country), study design, data source, number of participants, population (AMI, CABG or mixed), inclusion period, exclusion criteria, mean follow-up time, mean age of participants, gender, intervention characteristics, control characteristics, reported outcomes, information on outcomes, data on outcomes and covariates included in the adjusted models.
Statistical analysis
Analyses were separately performed with regards to population (ACS, CABG or mixed) and study design (prospective RCT or prospective or retrospective cohort study). For time-to-event outcomes, the hazard ratio (HR) with its 95% confidence interval (CI) was chosen as the effect measure. If possible, log HRs and their standard errors were extracted directly, preferably from an adjusted model and matched-group analysis. If these were not reported but adequate univariate analyses were available, an indirect estimation method was used.28,29 In some publications, an odds ratio (OR) or only absolute event numbers were reported. Therefore, in this review, studies calculating HRs or ORs were separately pooled and presented. 28 For dichotomous outcomes, the OR with its 95% CI was used as the effect measure. If necessary, the treatment effect was recalculated in order to be in the same direction, with HR or OR >1.0 indicating a higher event risk for patients participating in CR. HRs were combined using the generic inverse-variance method. ORs were pooled using the Mantel–Haenszel method or the generic inverse-variance method. The latter was only used when at least one study reported an adjusted OR and no absolute event numbers were given. Random-effects models were used to calculate overall effect estimates and confidence intervals, as heterogeneity between the ‘true’ effects of different rehabilitation programmes that were evaluated in the studies was assumed.
All of the results were checked for statistical heterogeneity by I2 statistics with 0–30% representing no or only small heterogeneity, 30–60% representing moderate heterogeneity, 50–90% representing substantial heterogeneity and 75–100% representing considerable heterogeneity. 29 Due to the heterogeneous study designs (rCCSs, pCCSs and RCTs) and statistical analysis methods (calculating either HR or OR), the number of studies per single meta-analysis was low. A statistical evaluation of potential publication bias based on funnel plot asymmetry could therefore not be performed. 29 Nevertheless, sensitivity analyses have been performed with respect to extracted results of alternative analysis techniques (e.g. independent groups instead of matched groups) and with respect to study quality (Table SM 4, Supplemental Material)).
Some deviations from the review protocol published in PROSPERO have to be reported. ORs instead of risk ratios were used as effect measures for dichotomous outcomes because, in some studies, adjusted ORs and no absolute event numbers were reported. Due to the small number of studies, a subgroup analysis, as originally planned, was not performed. R version 3.2.2 (R Foundation for Statistical Computing, 2015) and the R meta package version 4.3-2 (developed by Guido Schwarzer) were used for statistical analyses.
Results
Study characteristics
Study characteristics (design, population, interventions, controls and primary results) are given in Table 2. With respect to the design, only one RCT (n = 1813 patients) fulfilled the CROS criteria. In addition, 17 rCCSs (n = 206,096 patients) and seven pCCSs (n = 12,193 patients) were included. The populations predefined in CROS were distributed as follows: after ACS, n = 12 studies (n = 46,338 patients); after CABG, n = 5 studies (n = 14,583 patients); and mixed populations, n = 9 studies (n = 158,781 patients). The CR setting was ‘out-patient’ in most studies (n = 21) and predominantly ‘in-patient’ (including a variable part of “out-patient” CR) in the four studies from Germany. CR duration varied from 3–4 weeks up to 12 months, and CR intensity varied from two up to more than five exercise sessions per week plus sessions for motivation, information, education and psychosocial interventions, with variable intensities and combinations.
Meta-analysis
A summary of the clinical outcomes is given in Table 3. The primary endpoint ‘total mortality’ was evaluated in n = 22 studies, one of them evaluating both mortality after ACS and after CABG (Figure 2). 30 Participation in CR was associated with significantly reduced mortality in all but three studies.20,31,32 In another study, total mortality after AMI was reduced only in depressed patients. 33
After ACS, mortality was reduced in all pCCSs by a factor of 0.37 for patients participating in CR (n = 4 studies; HR 0.37, 95% CI 0.20–0.69), and heterogeneity was low (I2 = 17.8%). Similar results were obtained in the rCCSs, but heterogeneity was moderate to substantial. Sensitivity analyses did not change the results. The single RCT meeting the CROS inclusion criteria yielded a neutral result. 20
After CABG, all rCCSs consistently showed reduced mortality in patients participating in CR (HR 0.62, 95% CI 0.54-0.70), and heterogeneity was absent (I2 = 0%). One additional pCCS supported this result. 34 Using independent groups instead of matched groups in the study of Goel et al. did not change the results substantially (HR 0.56, 95% CI 0.45–0.69). 3
In ‘mixed populations’, CR participation was associated with a significant mortality reduction on the basis of n = 5 rCCSs and n = 1 pCCS. The analysis of the two rCCSs using ORs yielded a neutral result (OR 0.56, 95% CI 0.26–1.22), but heterogeneity was high (I2 = 81%). While the study of Suaya et al. showed a significant mortality reduction (OR 0.42, 95% CI 0.40–0.45), 4 the results of Schwaab et al. were neutral (OR 0.91, 95% CI 0.45–1.81). 32 Sensitivity analyses did not change the overall results.
Regarding the endpoints ‘cardiovascular mortality’ (n = 4 studies) and ‘major cardiovascular and cerebrovascular events (MACCE)’ (n = 3 studies), only single studies with different populations and designs could be identified, showing a trend in favour to CR participation. The outcomes ‘non-fatal myocardial infarction’ (total n = 6 studies) and ‘non-fatal stroke’ (total n = 2 studies) did not show any trends, and again all selected studies had different designs and populations.
Hospital readmission was investigated under various conditions (endpoints 6–9) by n = 6 studies with different designs. A consistent and clear effect of CR on hospital readmissions could not be observed after ACS, after CABG or in mixed populations.
In n = 7 studies, combined endpoints with various components were evaluated without any clear effect of CR participation. Again, these studies differed with respect to design and study population.
Quality evaluation of the studies
The quality of the cohort studies was assessed using the NOS and the checklists of methodological issues in non-randomised studies criteria.26,27,35 The sum of positive adjudications estimated by NOS is given in Table 4a (for details, see Table SM 2, supplemental material). Four out of 24 studies were adjudicated to have 5 points or less. Limitations have been adjudicated with respect to representativeness (n = 6), comparability of the cohorts (n = 3), adequacy of follow-up (n = 5) and the assessment of outcomes (n = 2).
On the basis of the checklist of methodological issues in non-randomized studies, the following characteristics were obtained: n = 3 studies gained their results by secondary analysis of other clinical studies with different original objectives. In n = 2 studies, there were either time or location differences between the study groups. Health care decision makers and patient preferences had potential influences on group formation in most studies. Moreover, the existence of study protocols was unclear in most studies, and a consort flow diagram was presented only in six out of 24 cohort studies. Management of confounding was not reported in n = 2 studies, whereas the description of potential confounding domains was unclear or not reported in n = 12 studies. Predefinition and calculation of confounding domains as prespecified by CROS (see ‘Methods’ section) were performed to various degrees, reflecting all eight predefined items in n = 4 studies. In contrast, n = 6 studies considered only three items, or even fewer. Adjustment for confounding was performed in n = 21 CCSs, with n = 3 studies not applying adequate biometrical methods.
Discussion
CROS is the first review and meta-analysis evaluating the prognostic effect of structured and multi-component CR exclusively in the era of statins and early interventional revascularisation for acute coronary events. Moreover, by systematically evaluating large CCSs, CROS makes an important independent contribution that more closely reflects the conditions in routine clinical practice. Previous systematic reviews have, in the pursuit of increased validity, exclusively included RCTs irrespective of publication date, with almost half of the studies having been performed in the pre-statin era.1,25 During this earlier period, treatment and medications were very different compared to clinical practice from 1995 onwards, and the impact of CR participation on the long-term clinical course could potentially have been attenuated through modern treatment options.
The major finding of CROS is that CR in the modern era of cardiology is associated with significantly reduced total mortality after ACS and after CABG (Table 3 and Figure 2). However, in the population after ACS, this positive result of CCSs does not concur with the only RCT included, which showed a neutral result (RAMIT).
20
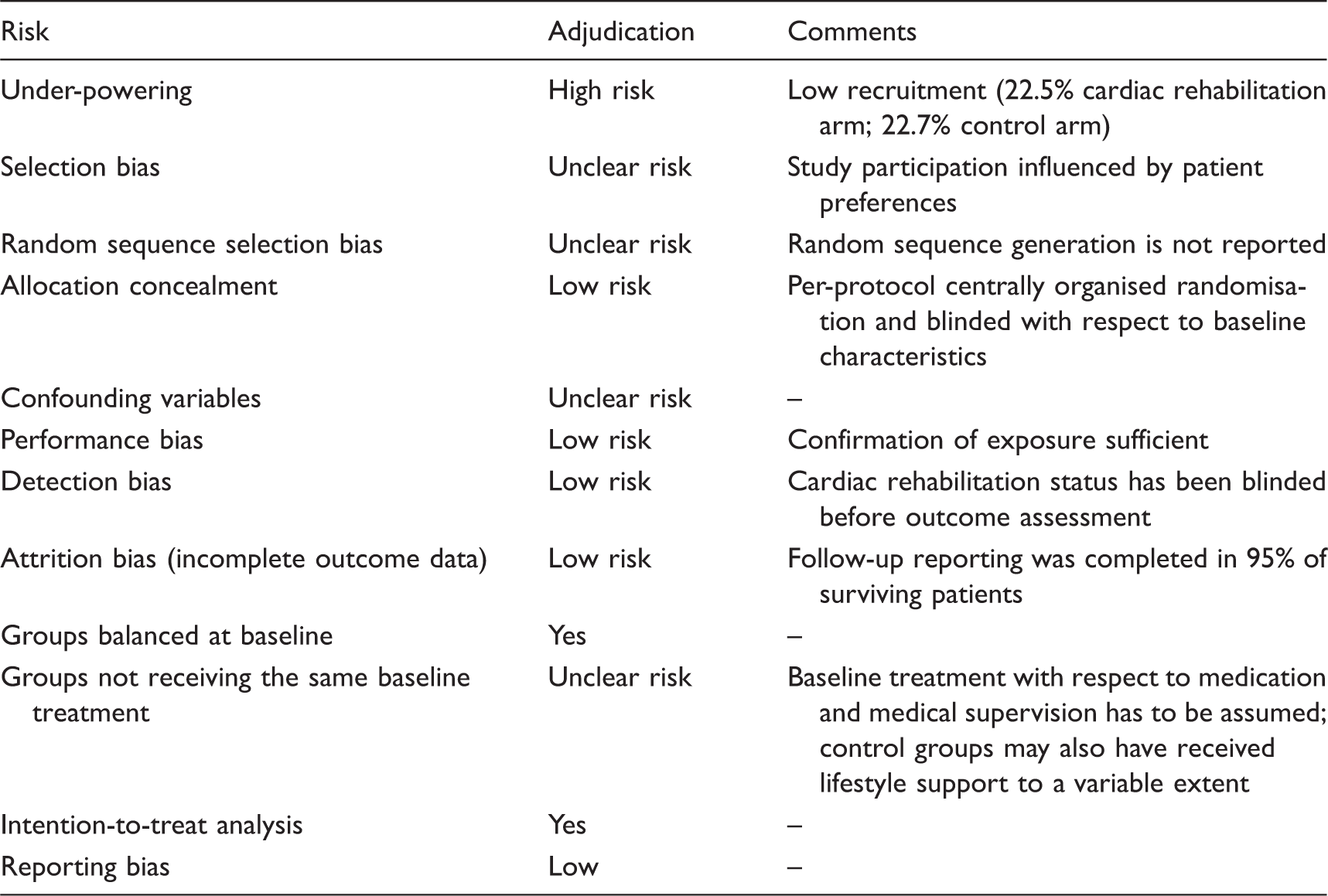
However, the RAMIT sample size represented, at best, 23% of the original predefined sample in each trial arm. This issue of poor recruitment does not explain the differences in findings, but it does indicate that the results from RAMIT may not be generalisable to a wider population. Plausible reasons for the neutral result in RAMIT may include super-selection of patients ready to participate in a RCT and a variable dose of CR compared to other trials.8,9,21,30,36
Analysis of total mortality. Forest plots presenting the evaluation of the endpoint ‘total mortality’.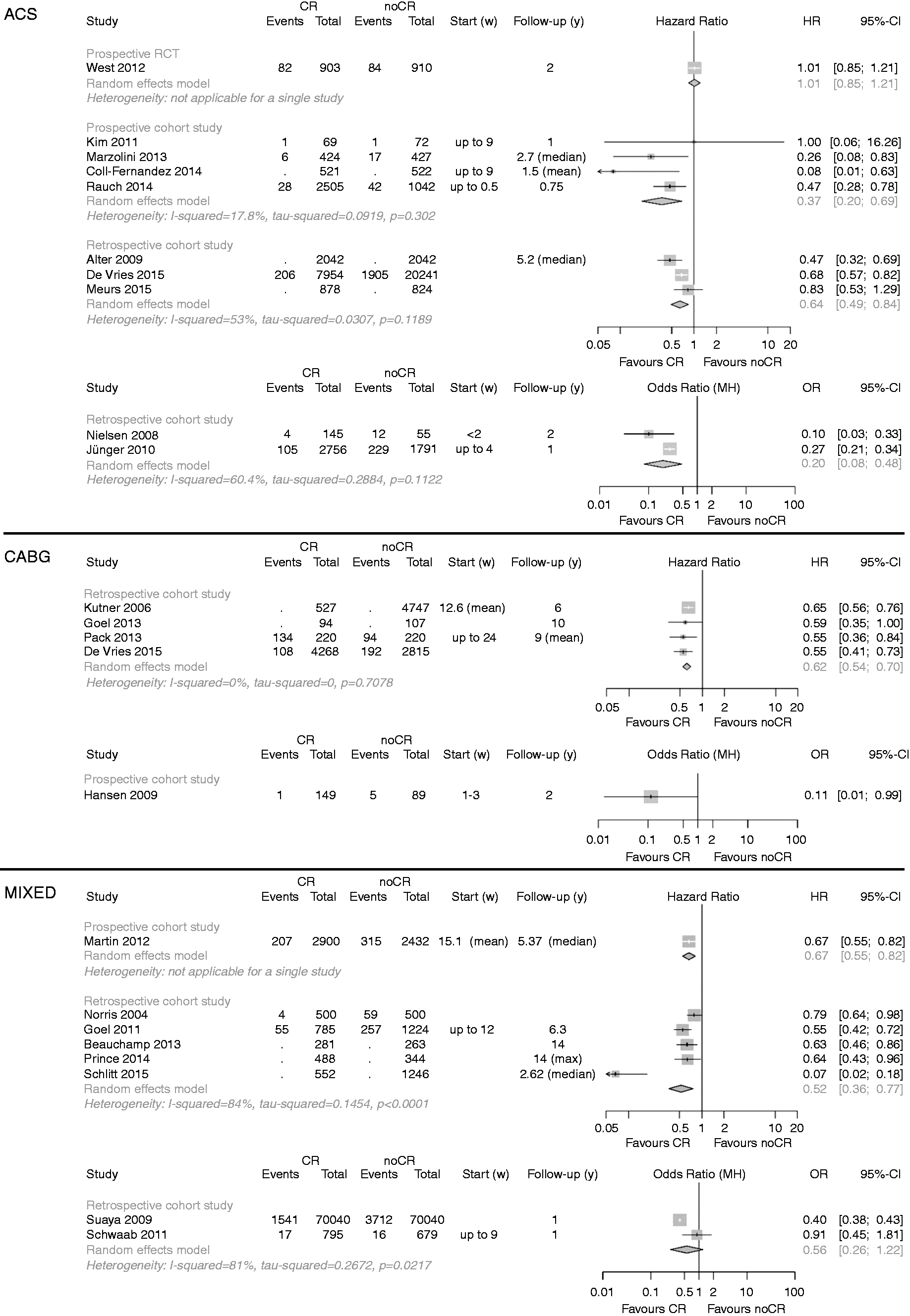
It may be criticised that within CROS, only one RCT was included. However, this was the result of a rigorous and targeted application of predefined selection criteria (e.g. population, timing and type of CR) (Table 1). The latest Cochrane review exclusively including RCTs also did not show a reduction of total mortality in the subgroup of studies published after 1995. However, in the same review, cardiovascular mortality was significantly reduced in both time periods, before and after 1995. 1 The variation in mode of mortality benefit between CROS (total mortality) and the Cochrane review (cardiac mortality) is not clarified, but may be the result of differences in populations under investigation and the type of CR delivered; for instance, ‘exercise-only’ interventions being part of the Cochrane analysis versus ‘multi-component’ CR being exclusively evaluated in CROS. Such differences in outcome from two recent meta-analyses highlight the ongoing need for well-designed studies with specified minimal standards in CR delivery and study reporting. Moreover, these problems underscore the need of both RCTs to prove efficacy under controlled (experimental) conditions and controlled and well-designed observational studies in order to prove the effectiveness of such complex clinical interventions as CR in clinical practice.
As structured and supervised exercise during CR has been a precondition for studies to be included in CROS, this may be regarded as the major mechanism contributing to mortality reduction. However, medical supervision, motivation, education and increased adherence to secondary prevention medication as shown in some included studies may also have contributed to the positive results.
No clear CR effect could be demonstrated with respect to non-fatal re-infarction and hospital readmissions (Table 3). One explanation for this could be that CR participation shifts a number of potentially ‘fatal re-infarctions’ to ‘non-fatal’ events, thereby reducing mortality, but not the rate of non-fatal re-infarctions. ‘Hospital readmission’ by definition is a weak clinical endpoint, as it is exposed to a variety of effectors and potential confounders (e.g. routine control coronary angiography in some areas, not necessarily reflecting the individual's health condition, availability of ambulatory cardiologists, psychosocial confounders, etc.). The results with respect to the remaining secondary endpoints are based on a single study or a low number of studies, therefore not allowing us to derive sufficiently evidence-based conclusions (Table 3).
In summary, from the presented results, it can be concluded that in the modern era of cardiology, multi-component CR remains an important and effective therapeutic intervention for reducing the risk of the premature death of CAD patients, especially after an acute event. CR therefore should be recommended as a core part of clinical practice after ACS or following CABG.
Limitations and strengths
Some aspects and limitations have to be considered.
Search strategy: while validated methodological search filters for RCTs exist, we were not aware of any validated methodological filters for cohort studies. Therefore, for cohort studies, the search filters used have not been validated so far. Study quality: for a final and conclusive estimation of the presented outcomes, the quality evaluation of the studies included is a basic requirement. However, the transferability of some predefined evaluation items of the methodological checklist for reviewing non-randomised trials was hampered, mainly due to the limited presentation of study protocol details in several studies. Limitations of the studies include the processes for group formation, information on study protocols and CR content, missing consort flow diagrams and management of confounding at the design stage (Tables 4a,b). The application of the NOS did not add significantly more information; rather, it confirmed the limitations of some of the studies (Tables 4a,b and SM3 in supplemental materials).
Heterogeneity of included studies: the CCSs included in CROS exhibited large heterogeneity due to them being prospective or retrospective and – as exemplified by nine studies – predominantly evaluating mixed populations, including patients after ACS and CABG, but also stable CAD patients in considerably varying proportions. Heterogeneity was also noted with respect to CR duration, intensity and volume (Table 2). Whereas the endpoint of ‘total mortality’ was evaluated in n = 22 studies (88%), the distribution and combination of secondary endpoints differed in every study, as did the composite endpoints under investigation with respect to their single components. Finally, a large variation was found with respect to the statistical methods applied in order to reduce confounding and the potential confounders included in the calculations (Tables 4a,b).
Heterogeneity with respect to study designs and statistical methods limits the validity of additional detailed analysis, hence our main task was to provide least biased and conservative effect estimates. Therefore, neither different types of effect estimates nor different study types were pooled together, meaning that only data based on adjusted models and matched-group analyses were used for the primary analysis. The heterogeneity of the studies therefore resulted in small numbers of studies per single meta-analysis, and evaluation of potential publication bias by funnel plots was not possible (see the ‘Methods’ section).
Heterogeneity, on the other hand, may also reflect the reality of routine clinical practice, which is known to vary between countries. This includes health care systems with different modalities of delivering CR and different conditions for gaining clinical outcome data for scientific evaluations. As these social, health economic and political preconditions cannot be changed, clinical science should try to balance and compensate for these factors by defining common international modalities for study designs that are appropriate for the investigation of multi-factorial health care interventions such as CR.
Conversely, the similarity of clinical results, such as the reduction of mortality in CAD patients associated with CR participation despite heterogeneous preconditions, could also reflect the robustness of the clinical CR effect. Against this background, the criteria for multi-component CR as defined for inclusion in CROS could, as a first step, become the minimal requirements (or standards) for successful CR. These standards should consist of early CR referral after an acute event and structured and supervised exercise at least twice a week, with additional education sessions and psychosocial interventions, all delivered by a multi-disciplinary team of skilled health professionals.
Conclusions
From the basis of 24 CCSs including 217,889 patients and reflecting routine clinical care in nine countries worldwide, participation in structured multi-component CR is associated with reduced mortality after an acute coronary event, even in the era of statins and acute revascularisations. In order to achieve high-quality evidence, internationally accepted minimal standards for the planning, performing and presenting of CCSs are warranted.
Footnotes
Author contribution
All authors participated in designing the study, generating hypotheses, interpreting data and critically reviewing the report. The special responsibilities were as follows: initiation, organisation and leading of the project: Bernhard Rauch, Patrick Doherty, Constantinos H. Davos, Jean-Paul Schmid and Heinz Völler; literature search and search strategies: Maria-Inti Metzendorf and Bernhard Rauch; study selection: Constantinos H Davos, Patrick Doherty and Bernhard Rauch; study evaluation: Daniel Saure, Constantinos H Davos, Patrick Doherty, Annett Salzwedel, Bernhard Rauch, Heinz Völler and Katrin Jensen; statistical and biometrical analyses: Daniel Saure and Katrin Jensen; writing: Bernhard Rauch, Constantinos H Davos, Patrick Doherty, Daniel Saure, Maria-Inti Metzendorf and Katrin Jensen; internal reviewing: Jean-Paul Schmid, Heinz Völler, Annett Salzwedel and the members of the nucleus of the cardiac rehabilitation section of the European Association of Preventive Cardiology (EAPC).
Acknowledgements
We thank Margaret Sampson (Children's Hospital of Eastern Ontario) for her peer review of the MEDLINE search strategy. We also thank Thomas Werner Holzinger for supporting the scientific group during the process of study evaluation.
EAPC Cardiac Rehabilitation Section, nucleus members:
– Patrick Doherty, Dep. of Health Sciences, University of York, Heslington, York, UK – Constantinos H Davos, Cardiovascular Research Laboratory, Biomedical Research Foundation, Academy of Athens, Athens, Greece – Ana Abreu, Dept. Hospital Santa Marta, Lisbon, Portugal – Jean-Paul Schmid, Department of Cardiology Spital Tiefenau, Bern, Switzerland – Marco Ambrosetti, Cardiovascular Rehabilitation Unit, ‘Le Terrazze’ Clinic, Cunardo, Italy – Romualdo Belardinelli, Cardiac Rehabilitation & Prevention, Lancisi Heart Inst. – Azienda Ospedali Riuniti, Ancona, Italy – Ugo Corra, Cardiology Div., Salvatore Maugeri Foundation, IRCCS, Scientific Institute of Veruno, Veruno, Italy – Margaret Cupples, Dept. of General Practice, UKCRC Centre of Excellence for Public Health Research, Queens University, Belfast, Northern Ireland, UK – Stefan Höfer, Innsbruck Medical University, Austria – Marie-Christine Iliou, Cardiac Rehabilitation and Secondary Prevention, Corentin Celton Hospital, APHP, Paris, France – Carlo Vigorito, Internal Medicine and Cardiac Rehabilitation, Dept. Translational Medical Sciences, University of Naples Federico II, Italy – Heinz Völler, Centre of Rehabilitation Research, University of Potsdam, Germany
Systematic review registration
PROSPERO international prospective register of systematic reviews: http://www.crd.york.ac.uk/prospero/review_print.asp?RecordID=7084&UserID=5736. Prospero registration number: CRD42014007084.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Pfizer AG Switzerland (unrestricted grant), Deutsche Herzstiftung e.V. (German Heart Foundation), Deutsche Gesellschaft für Prävention und Rehabilitation von Herz-Kreislauferkrankungen e.V. (DGPR; German Society of Cardiovascular Prevention and Cardiac Rehabilitation). The sponsors did not have any influence on study initiation, conducting and reporting.