
Abstract
Patients with chronic thromboembolic pulmonary hypertension (CTEPH) require lifelong anticoagulation therapy. However, the bleeding risk and recurrence of venous thromboembolism (VTE) in CTEPH patients who are administered warfarin have not been adequately evaluated. The purpose of this study was to evaluate the risk of clinically relevant bleeding, recurrent VTE, and clinical worsening in patients with CTEPH who were administered warfarin.
The clinical records of 72 patients with CTEPH who regularly visited our institution and were administered warfarin were retrospectively reviewed between 1 January 2011 and 31 December 2015. We investigated the incidence of clinically relevant bleeding events, recurrent VTE, and hospitalization for the deterioration of pulmonary hypertension or right heart failure (RHF) during the observation period.
The mean observation period for the 72 patients was 3.60 ± 1.60 person-years. Clinically relevant bleeding, RHF, and recurrent VTE occurred in 21 (29.2%), eight (11.1%), and three (4.2%) of 72 patients, respectively, and the incidence rates for these events were 8.1%/person-year, 3.1%/person-year, and 1.2%/person-year, respectively. The incidence rates for the major and non-major bleeding events were 5.0%/person-year and 3.9%/person-year, respectively. The incidence of clinically relevant bleeding events was 20.8%/person-year during medical treatment with a soluble guanylate cyclase stimulator. One of 35 patients (2.9%) during the post-pulmonary endarterectomy period experienced hemoptysis during observation period (> 6 months after pulmonary endarterectomy). No bleeding events occurred during the post-balloon pulmonary angioplasty period.
In conclusion, warfarin effectively prevents VTE recurrence in CTEPH patients, but its effects may be associated with a considerable bleeding risk.
Keywords
Chronic thromboembolic pulmonary hypertension (CTEPH) is a type of pulmonary hypertension (PH) characterized by chronic pulmonary obstruction caused by organized thrombi.1–3 Following its definitive diagnosis at specialist institutions, specific treatments for CTEPH are considered. Pulmonary endarterectomy (PEA), which is a surgical procedure that removes organized thrombi from the pulmonary arteries, 4 is recommended for CTEPH patients who have surgically accessible thrombi and low risk/benefit ratios. 2 For patients diagnosed with inoperable CTEPH or those who have symptomatic residual PH after PEA, balloon pulmonary angioplasty (BPA) and/or medical treatment using pulmonary vasodilators are considered. 2 The findings from the Chronic Thromboembolic Pulmonary Hypertension Soluble Guanylate Cyclase-Stimulator Trial (CHEST) showed that riociguat, which is a soluble guanylate cyclase (sGC) stimulator, improves the hemodynamics and exercise capacity of patients with CTEPH. 5 Prior to disease-specific therapy, lifelong anticoagulation is essential, 2 because venous thromboembolism (VTE) with repeated acute pulmonary thromboembolism1,6 may cause or trigger CTEPH. Warfarin, a vitamin K antagonist, is commonly used for anticoagulation in CTEPH patients. Recently, direct oral anticoagulants (DOACs) have become widely available for VTE, and they may become available for the treatment of CTEPH in the future. However, the recurrence of VTE and the bleeding risk in CTEPH patients while taking warfarin have not been investigated. We believe that the risks associated with warfarin use in CTEPH patients should be elucidated in a clinical practice setting before undertaking a study to investigate the transition from warfarin to DOAC therapy. Hence, with the above in mind, the purpose of this study was to evaluate the risk of clinically relevant bleeding, recurrent VTE, and clinical worsening in patients with stable CTEPH who were administered warfarin, and to investigate the relationships between the effects of the bleeding risk associated with warfarin and specific treatments for CTEPH.
Methods
Patient inclusion and exclusion criteria
This study was approved by the Ethics Committee of Chiba University (Approval number: 826). Written informed consent was provided by all patients.
Between March 1986 and December 2015, 268 patients were diagnosed with CTEPH at Chiba University Hospital. The CTEPH diagnostic criteria were as follows: (1) a mean pulmonary artery pressure (mPAP) ≥ 25 mmHg and a normal pulmonary arterial wedge pressure (PAWP) ≤15 mmHg, which was confirmed using right heart catheterization (RHC); (2) symptoms, including dyspnea, which had persisted for > 6 months; and (3) a persistent pulmonary embolism that was resistant to effective anticoagulation (>3 months) and was confirmed by a lung perfusion scan, a computed tomography (CT) scan, or pulmonary angiography.
3
We reviewed the clinical records of 268 patients and excluded 196 patients. The exclusion criteria were as follows: (1) the absence of clinical records from 2011 to 2015; (2) too few visits to our institution during the observation period to generate sufficient clinical data to enable evaluations of clinical worsening and bleeding; and (3) patients who did not take warfarin from 2011 to 2015. Finally, 72 CTEPH patients were retrospectively investigated in this study (Fig. 1).
Flow diagram showing the inclusion and exclusion of patients. CTEPH, chronic thromboembolic pulmonary hypertension.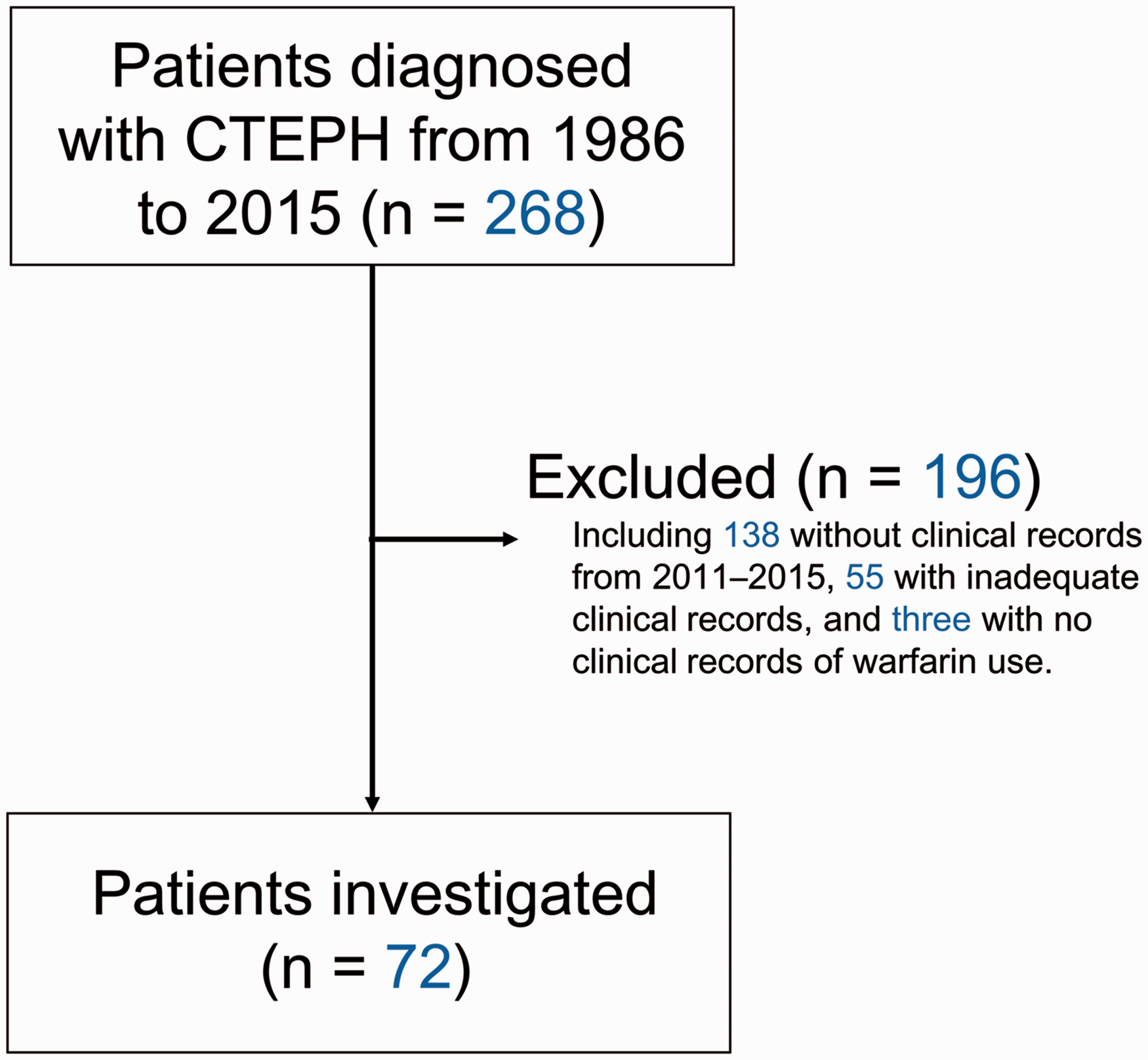
Definitions and exclusion criteria associated with the observation period
The entire observation period spanned from 1 January 2011 to 31 December 2015 (five years). For a patient who was diagnosed between 2011 and 2015, the start date was defined as the date of the definitive diagnosis at our institution. For a patient who was transferred to another hospital during the observation period, the end date was defined as the last day on which they visited our institution. For a patient who died during the observation period, the end date was defined as the date of death. The targets of this study were CTEPH patients in the stabilized period, and the confounding effects of other anticoagulants or interventional treatments were eliminated. Therefore, the following time periods were excluded from the observation periods: (1) the periods before a definitive diagnosis at our institution; (2) the six-month period after PEA or BPA; (3) treatment periods involving the use of DOACs or heparin including changes to heparin before and after interventional procedures; (4) periods associated with double-blind clinical trials, for example, those involving riociguat or selexipag.
Assessment of anticoagulation control
CTEPH patients require lifelong anticoagulation therapy. However, there is no evidence supporting an appropriate warfarin dose. 2 According to the 2014 European Society of Cardiology and the Japanese VTE guidelines, the target ranges for the prothrombin time (PT)-international normalized ratio (INR) for patients with acute pulmonary embolism are 2–3 and 1.5–2.5, respectively.7,8 Therefore, we aimed to use warfarin doses that achieved a PT-INR therapeutic range of 1.5–3.0. Anticoagulation control was assessed as a percentage of the INR value (%INR) using the method described by Nakatani et al. 9 The %INR was defined as the ratio of the number of PT-INRs within the target range to the total number of PT-INR measurements, and was correlated positively with the time within the therapeutic INR range (R2 = 0.917, P < 0.01). 9
Definition of clinically relevant bleeding events
To rigorously evaluate bleeding events, we adopted the bleeding events criteria used in previous clinical trials involving DOACs. 10 Clinically relevant bleeding comprised major bleeding and clinically relevant non-major bleeding. Major bleeding included hemorrhage associated with a reduction in hemoglobin level of >2.0 g/dL, bleeding requiring a red blood cell or whole blood transfusion of >2 units, hemorrhage in a vital organ, such as intracranial bleeding, or a hemorrhage that led to death. Clinically relevant non-major bleeding, or non-major bleeding, was defined as a mild-to-moderate temporary hemorrhage that originated from the gingiva, nose, airway, gastrointestinal tract, muscle, or subcutaneous tissue (>25 cm2), and persistent bleeding after catheter insertion or surgery.
Definition of clinical worsening events
We defined clinical worsening events as hospitalization caused by exacerbations of PH or right heart failure (RHF) or recurrent symptomatic VTE, although regular check-up hospitalizations for RHC were excluded. We defined VTE events as symptomatic pulmonary embolism or deep vein thrombosis, 10 confirmed by CT or leg echo. We excluded asymptomatic in situ rethrombosis or growing thrombosis of the pulmonary artery after PEA, which were incidentally found at follow-up CT.
Data analysis
All of the data were combined using Microsoft Excel 2013. Unless otherwise stated, the data are presented as means and standard deviations. To account for exposure to each specific CTEPH therapy, an event incidence was calculated as a ratio obtained by dividing the number of patients with that event by the mean exposure period to each treatment, and it is expressed as %/person-year. Comparisons between two groups were analyzed by Student’s t-test using EZR (ver. 1.29, Saitama Medical Center, Jichi Medical University, Saitama, Japan). 11
Results
Patients’ characteristics
The mean age of the 72 patients on the start date of the observation period was 59.7 ± 11.9 years; 11 patients were men. At diagnosis, the mPAP, pulmonary vascular resistance (PVR), and cardiac index were 43.5 ± 10.9 mmHg, 694 ± 270 dyne·s·cm–5, and 2.96 ± 0.82 L/min/m2, respectively. The number of days from diagnosis to the start of the observation period was 1663 ± 2121 days. At the last catheterization before the observation periods the mPAP, PVR, and cardiac index were 41.4 ± 13.6 mm Hg, 656 ± 321 dyne·s·cm–5, and 2.77 ± 0.56 L/min/m2, respectively. Sixty-two (86.1%) of the 72 patients had PH at the start of the observation period, and 39 (54.2%) and ten (13.9%) patients underwent PEA and BPA, respectively, from the date of their diagnosis to the end of the observation period.
Bleeding events, right heart failure, and recurrent thrombosis
The total observation period was 258.9 person-years (94,500 person-days) and the mean observation period was 3.60 ± 1.60 person-years. Clinically relevant bleeding, RHF or PH exacerbation, and recurrent pulmonary embolism occurred in 21 (29.2%), eight (11.1%), and three (4.2%) patients, respectively and the number of these events was 36, 14, and three, respectively. All three VTE events were symptomatic pulmonary embolism detected by enhanced CT. One RHF event was associated with recurrent pulmonary embolism. The incidence rates for patients with these events were 8.1%/person-year, 3.1%/person-year, and 1.2%/person-year, respectively (Fig. 2a).
Incidence rates of events. (a) Overall incidence of events. (b) Incidence of bleeding events from 2011 to 2015. RHF, right heart failure.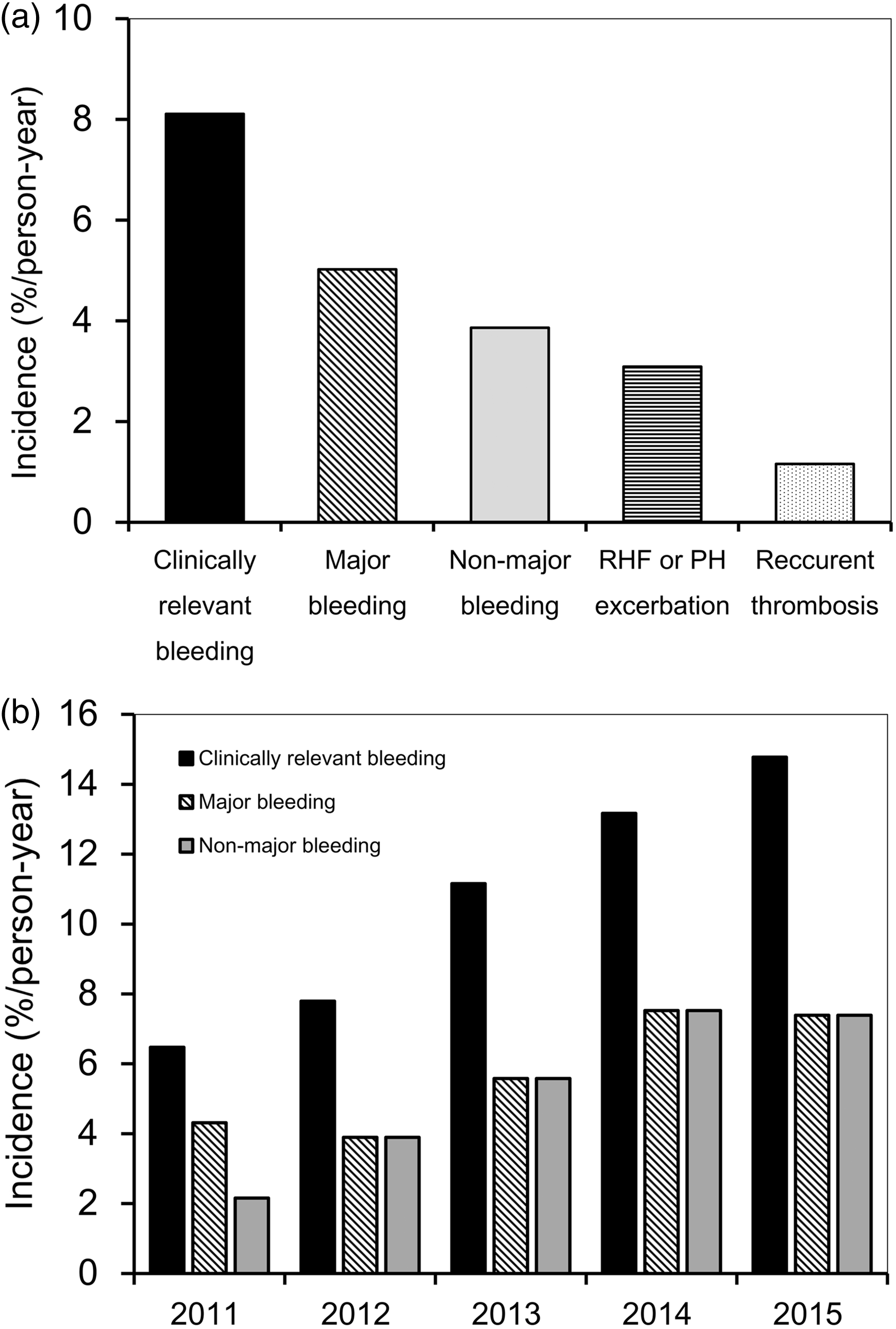
Characteristics of the clinically relevant bleeding events
Bleeding site or cause and prothrombin time-international normalized ratio.
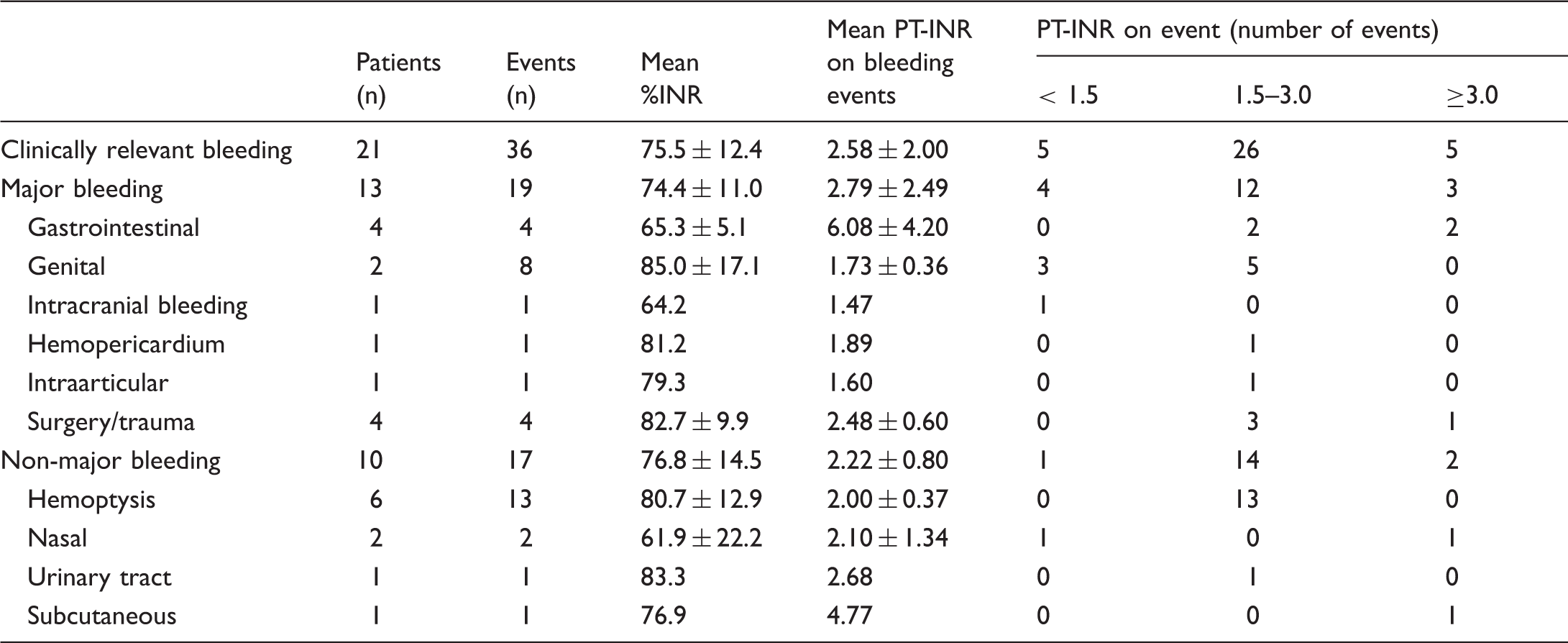
%INR, percentage of the international normalized ratio; PT-INR, prothrombin time-international normalized ratio.
Anticoagulation control and bleeding events
The 72 patients had a mean %INR of 81.1 ± 13.3% and the 21 patients with clinically relevant bleeding had a mean %INR of 75.5 ± 12.4%. Thirty-one of 36 clinically relevant bleeding events (86.1%) were not associated with hyperanticoagulation (PT-INR > 3.0) (Table 1).
PT-INR on clinical worsening events
Prothrombin time-international normalized ratio on clinical worsening events.

%INR, percentage of the international normalized ratio; PT-INR, prothrombin time-international normalized ratio; PH, pulmonary hypertension; RHF, right heart failure; VTE, venous thromboembolism.
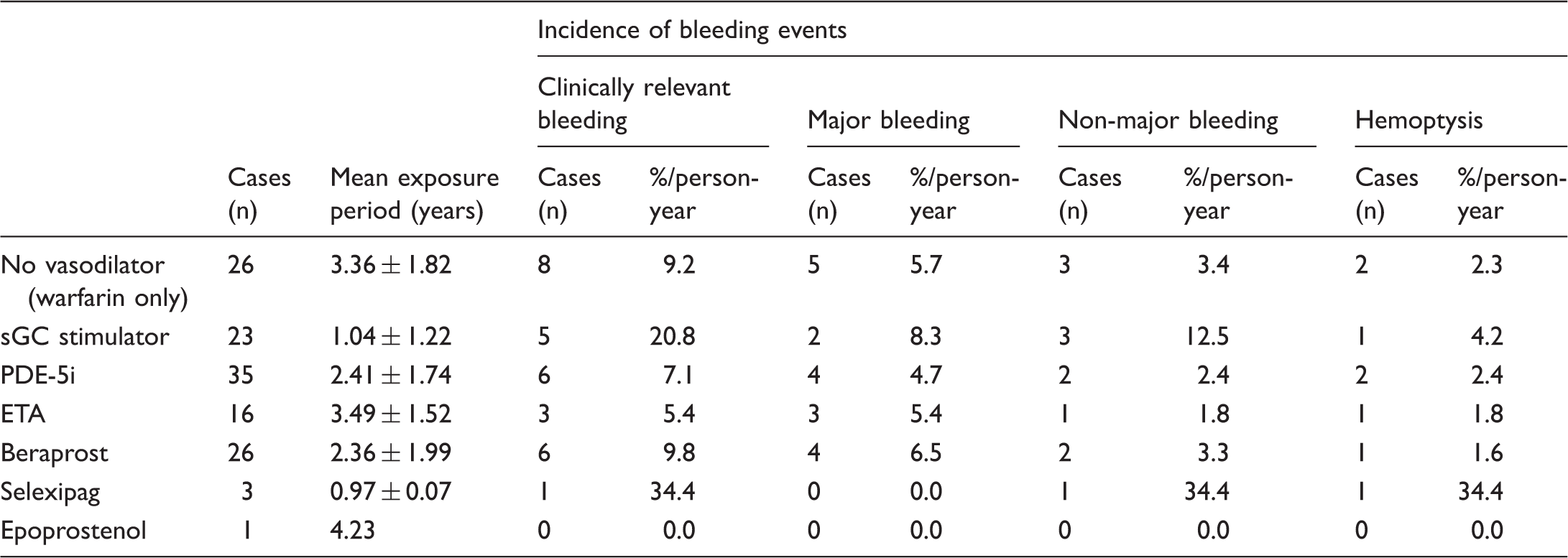
Pulmonary vasodilators and bleeding events
Fig. 3 illustrates the use of pulmonary vasodilators for CTEPH patients at our institution. Table 3 summarizes the medical therapies used for CTEPH and the incidence of bleeding events during each exposure period. The incidence of clinically relevant bleeding events during the periods when pulmonary vasodilators were not used was 9.2%/person-year (Table 3). Five (21.7%) of 23 patients who were treated with an sGC stimulator experienced clinically relevant bleeding events and the incidence was 20.8%/person-year. Two major bleeding events occurred during sGC stimulator treatment that required blood transfusions: one was gastrointestinal; and one was genital. Three non-major bleeding events occurred: one was nasal; one comprised hemoptysis; and one was subcutaneous. The incidence of clinically relevant bleeding events during monotherapy with an sGC stimulator was 22.2%/person-year. The incidence rates for clinically relevant bleeding events during dual and triple combination therapy were 9.5%/person-year and 0%/person-year, respectively (Supplementary Table 2).
Usage of pulmonary vasodilators for CTEPH patients at our institution. Epo, epoprostenol; Sel, selexipag; ERA, endothelin receptor antagonist; PDE-5i, phosphodiesterase-5 inhibitor. Medical therapy and the incidence of bleeding events. sGC, soluble guanylate cyclase; PDE-5i, phosphodiesterase-5 inhibitors; ETA, endothelin receptor antagonists.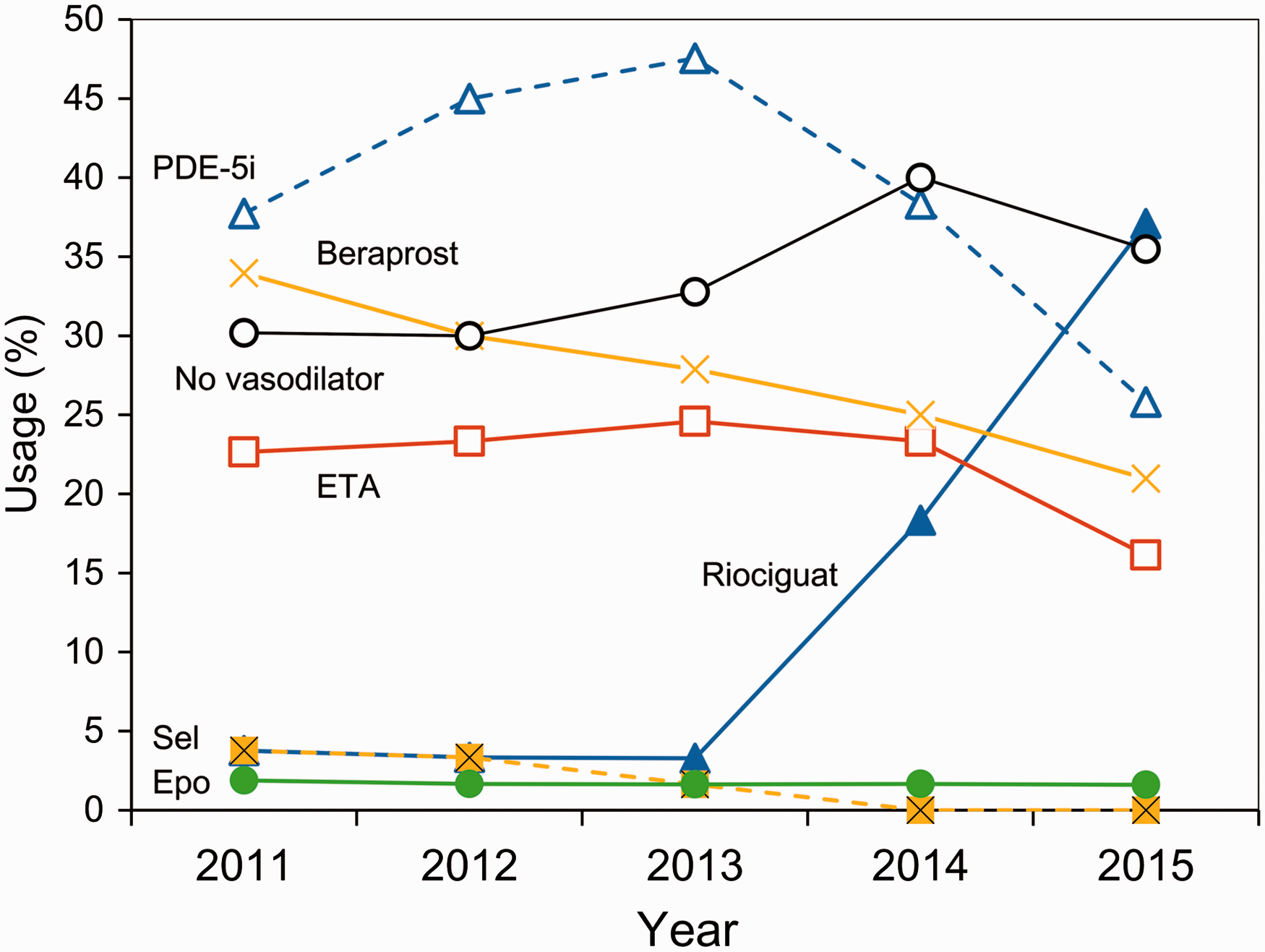
The incidence of hemoptysis after pulmonary endarterectomy and balloon pulmonary angioplasty
Anticoagulation effect and bleeding risk of warfarin after interventional treatments.
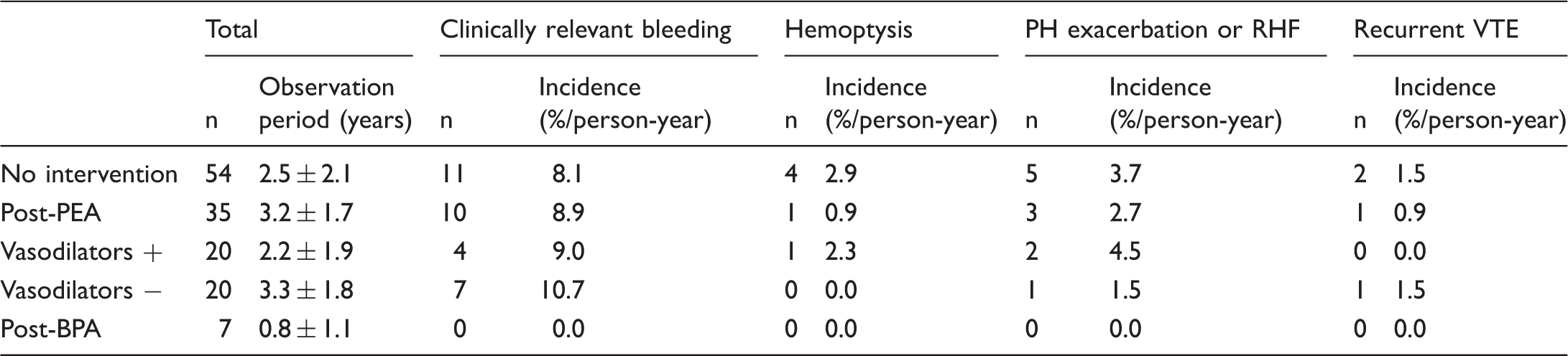
PH, pulmonary hypertension; RHF, right heart failure; VTE, venous thromboembolism; PEA, pulmonary endarterectomy; BPA, balloon pulmonary angioplasty.
Discussion
In this study, we evaluated the occurrence of bleeding, RHF, and VTE events in patients with CTEPH treated with warfarin. We found that while anticoagulation therapy using warfarin was effective at preventing recurrent VTEs in CTEPH patients, it was associated with a considerable bleeding risk.
Comparison between the current study and a previous study.
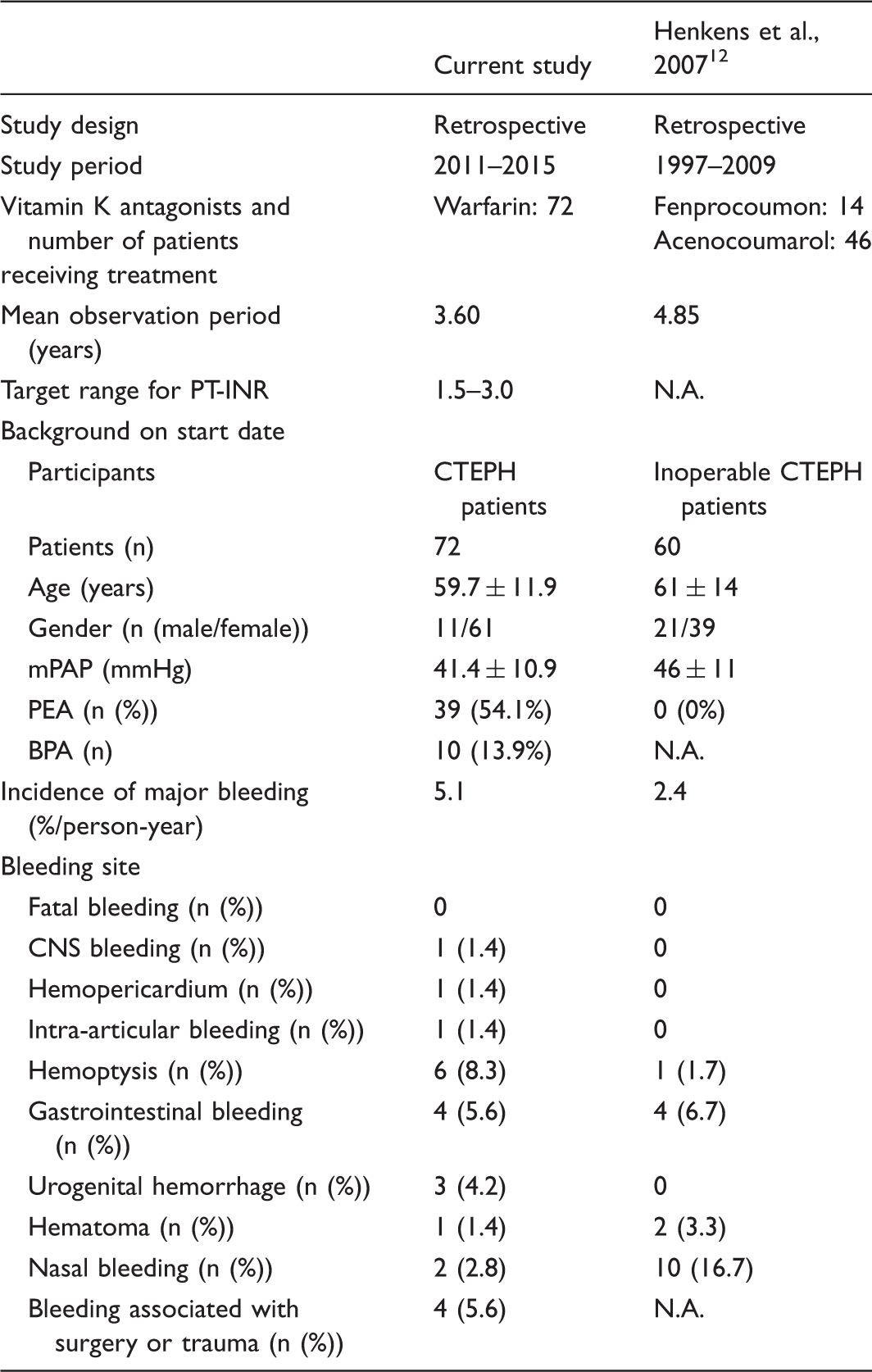
PT-INR, prothrombin time-international normalized ratio; mPAP, mean pulmonary arterial pressure; CNS, central nervous system; N.A., not analyzed; CTEPH, chronic thromboembolic pulmonary hypertension; PEA, pulmonary endarterectomy; BPA, balloon pulmonary angioplasty.
Some selective pulmonary vasodilators might be associated with increases in the bleeding risk during anticoagulation by warfarin. The present study revealed that the frequency of bleeding events was higher during combined sGC stimulator and warfarin therapy than that during treatment with warfarin alone. The findings of the present study also showed that the incidence of clinically relevant bleeding events increased during the observation period, and that the use of sGC stimulators increased during the latter half of the study period. The findings from the CHEST-2 study showed that hemoptysis or pulmonary hemorrhage occurred in 5% of patients over a two-year period.13,14 The findings from clinical studies of CTEPH patients treated with bosentan or sildenafil showed that nasal hemorrhage occurred in 5.2% and 7.5% of patients, respectively.15,16 Epoprostenol and beraprost may increase the bleeding risk, 17 but the precise bleeding incidence has not yet been evaluated in any study, including clinical trials investigating epoprostenol18,19 and beraprost 20 in the treatment of patients with CTEPH. In a clinical trial of selexipag, which is a prostacyclin receptor agonist, it was reported that 2.4% of patients treated with selexipag experienced major bleeding events, and the occurrence was similar to that of the placebo group. 14 Bleeding events were neither primary nor secondary endpoints, nor were the bleeding event criteria clearly defined in any of the clinical studies that have investigated the use of pulmonary vasodilators in CTEPH patients.5,15,18–20 It is possible that the investigators might have failed to report the bleeding events and that the bleeding risk might have been underestimated in previous clinical studies. Hence, the hemodynamic changes as well as detailed assessments of bleeding risk should be included in future clinical trials.
The risk of hemoptysis during the post-PEA or BPA periods might not be high. The luminal structure of the pulmonary arteries can drastically change after PEA or BPA. After PEA, organized thrombi can be removed after PEA and media of pulmonary arteries can be exposed to blood flow. 4 It was reported that the microscopic dissection of pulmonary arteries occurred after BPA. 21 It is also thought that hemoptysis in CTEPH patients might be associated with the development bronchial arteries that may connect with pulmonary arteries and organized thrombi.22,23 We hypothesized that the risk of hemoptysis might be increased after PEA and BPA. The results suggested that the risk might be lower than expected. Simonneau et al. reported that hemoptysis occurred in 8% of patients who were treated with sGC stimulator riociguat for residual PH after PEA. 14 In the current study, hemoptysis occurred in one of 35 patients (2.9%) during the postoperative periods and in none of seven patients during the post-BPA period. 14 To the best of our knowledge, very little information is available regarding bleeding events during the periods of stabilization after PEA and BPA; hence, further investigations to address this gap in knowledge are required.
Hyperanticoagulation tends to be associated with an increase in the bleeding risk. Certain antibiotics, anti-inflammatory drugs, fruits (such as grapefruit and mango), and alcohol can increase the anticoagulant effect of warfarin, resulting in a high risk of bleeding. 24 In particular, acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs) have antiplatelet effects and can induce gastric erosion, which increases the risk of gastrointestinal bleeding. 24 In the present study, two patients with major gastrointestinal bleeding and prolonged PT-INRs had received NSAIDs (data not shown). However, 86% of the clinically relevant bleeding events were not associated with hyperanticoagulation in the current study. Bronchiectasis is a major cause of hemoptysis. 25 In the current study, three of six patients with hemoptysis had bronchiectasis. Both patients who experienced major genital bleeding had histories of repeated prolonged menstruation that was associated with uterine myomas and endometrial hyperplasia. We believe that a patient’s co-morbidities are associated with the risk of bleeding risk.
The incidence of recurrent VTE was 1.2%/person-year in this study. To the best of our knowledge, the incidence of recurrent VTE in CTEPH patients during anticoagulation therapy has not been clearly determined as yet. The findings from clinical trials of DOACs for the treatment of acute VTE showed that the incidence of recurrent VTE was 1.3–3.5% per half year in patients in the conventional treatment groups who were administered unfractionated or low-molecular-weight heparin followed by warfarin.10,26–28 Three recurrent VTE events occurred when PT-INR values were < 2 in this study. It seems that the dose of warfarin in these cases might be sub-therapeutic. Further study to investigate the appropriate target dose of warfarin for CTEPH patients is needed.
In this study, the incidence of hospitalization due to the deterioration of PH or RHF was 3.1%/person-year. During the treatment of patients with inoperable CTEPH or those with residual PH after PEA with an sGC stimulator, the incidence of clinical worsening was 22% over an observation period of two years. 14 The present study included patients who did not have residual PH after PEA; hence, the discrepancy between the current study and the aforementioned study in relation to the incidence of deterioration of PH or RHF might be associated with differences in the characteristics of the participants.
The impact of polymorphisms of vitamin K epoxide reductase 1 (VKORC1) and cytochrome P450 2C9 (CYP2C9) on anticoagulant effect and bleeding risk was unclear. The polymorphisms of VKORC1 and CYP2C9 could be affected by the dose of warfarin.29,30 However, it seems that the impact of polymorphisms of VKORC1 and CYP2C9 on anticoagulant effect and bleeding risk was unclear in the clinical setting. Kimmel et al. reported that there was no difference in the therapeutic range of PT-INR and the incidence of major bleeding or thromboembolism between genotype-guided and clinically guided groups. 31 In this study, the mean dose of warfarin in patients with or without clinically relevant bleeding at the end of observation period was 3.3 ± 1.0 or 3.8 ± 1.5 mg/day, respectively, and the difference was not significant (P = 0.2, data not shown).
The present study has several limitations. First, the study was retrospective and observational. Second, the study was performed at a single institution. Third, the sample size was relatively small. Therefore, precise evaluations of the bleeding event rates in large prospective studies are necessary. Finally, the polymorphisms of VKORC1 and CYP2C9 were not investigated in this study. However, the results of this study still shed light on the potential bleeding risk associated with anticoagulation in CTEPH patients.
In conclusion, warfarin effectively prevents VTE recurrence in CTEPH patients, but this may be associated with a considerable bleeding risk. Pulmonary vasodilators and co-morbidities might be associated with increases in the bleeding risk.
Footnotes
Conflict of interest
The authors declare the following conflicts of interest: TJ is a member of an endowed department sponsored by Actelion Pharmaceuticals Ltd.; NT is a member of an endowed department sponsored by Actelion Pharmaceuticals Ltd. and received lecture honoraria from Bayer AG, Daiichi-Sankyo Company, Limited, and Actelion Pharmaceuticals Ltd.; RN is a member of an endowed department sponsored by Actelion Pharmaceuticals Ltd.; RS received a research grant from GlaxoSmithKline plc; FK and RS received a research grant from GlaxoSmithKline plc; and KT received lecture honoraria from GlaxoSmithKline plc and Pfizer Inc. The other authors had no conflicts of interest.
Funding
This study was supported by Japanese Ministry of Health, Labour and Welfare research grants specifically designated to the Respiratory Failure Research Group and Cardiovascular Diseases, and the Pulmonary Hypertension Research Group from the Japan Agency for Medical Research and Development (No. 16ek0109127h0002). The funder had no role in the study’s design, collection of data or their analysis, decision to publish, or the preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.