
Abstract
Pulmonary arterial hypertension (PAH) is characterized by obstruction of pre-capillary pulmonary arteries, which leads to sustained elevation of pulmonary arterial pressure. Identifying those at risk through early interventions, such as genetic testing, may mitigate disease course. Current practice guidelines recommend genetic counseling and offering genetic testing to individuals with heritable PAH, idiopathic PAH, and their family members. However, it is unclear if PAH specialists follow these recommendations. Thus, our research objective was to determine PAH specialists’ knowledge, utilization, and perceptions about genetic counseling and genetic testing. A survey was designed and distributed to PAH specialists who primarily work in the USA to assess their knowledge, practices, and attitudes about the genetics of PAH.
Participants’ responses were analyzed using parametric and non-parametric statistics and groups were compared using the Wilcoxon rank sum test. PAH specialists had low perceived and actual knowledge of the genetics of PAH, with 13.2% perceiving themselves as knowledgeable and 27% actually being knowledgeable. Although these specialists had positive or ambivalent attitudes about genetic testing and genetic counseling, they had poor utilization of these genetic services, with almost 80% of participants never or rarely ordering genetic testing or referring their patients with PAH for genetic counseling. Physicians were more knowledgeable, but had lower perceptions of the value of genetic testing and genetic counseling compared to non-physicians (P < 0.05). The results suggest that increased education and awareness is needed about the genetics of PAH as well as the benefits of genetic testing and genetic counseling for individuals who treat patients with PAH.
Introduction
Pulmonary arterial hypertension (PAH) is a progressive disorder associated with high pulmonary artery pressure that has potential to cause right ventricular failure and death.1,2 Two subgroups of PAH are idiopathic PAH (IPAH) and heritable PAH (HPAH). PAH is considered heritable when there is at least one other family member who has or has had PAH or when a germline mutation is found in one of a number of known PAH risk genes including, but not limited to, BMPR2, ACVRL1, ENG, SMAD9, CAV1, and KCNK3.3–12 An individual is considered to have IPAH when there is neither an identified contributing risk factor nor family history of PAH.13,14 However, it has been found that upwards of 20% of those diagnosed with IPAH have identifiable germline mutations in a known risk gene and thus should be classified as HPAH.2,15
Through the use of genetic services, individuals at risk for PAH have the option to undergo pre-symptomatic genetic testing, begin clinical screening for the disease if necessary, and can make reproductive choices better suited for themselves and their families.16–18 All of these options could be a financial burden on a family. Clinicians may be better able to justify screening recommendations to health insurance companies for asymptomatic individuals with a predisposing genetic mutation for PAH than without genetic information. In the USA, the Genetic Information Nondiscrimination Act protects its citizens from discrimination in employment as well as cost and coverage of health insurance. 19
As early interventions have the potential to mitigate the disease course, current practice guidelines from the American College of Chest Physicians, in addition to other literature, recommend genetic testing and genetic counseling to individuals with HPAH, IPAH, and their family members.20–25 However, it is unclear if clinicians, specifically in the USA, follow these guidelines and recommendations that have been in existence for over ten years.20,26–28 Thus, it is important to determine not only the referral rates to genetic services (counseling and testing) but also to determine the reasons why physicians may not refer. There have been nearly 600 papers published about the genetics of PAH between 2010 and 2014, but it is unclear whether PAH specialists remain current in the dynamic field of genetics. Thus, the objective of this research is to determine the utilization, knowledge, and perceptions about genetic counseling and genetic testing of PAH specialists.
Methods
The survey created for this project was approved by the Institutional Review Board of Cincinnati Children’s Hospital Medical Center. Consent was assumed by participants returning the survey or by submitting the survey online.
Participants and distribution
Clinicians, healthcare coordinators, and researchers (PAH specialists) who are involved with patients with PAH were invited to complete the paper survey at the 2014 Pulmonary Hypertension Association (PHA) International PH Conference and Scientific Sessions from June 20th–22nd and also through a REDcap electronic survey sent to members of the Pulmonary Hypertension Clinicians and Researchers (PHCR) and the Pulmonary Hypertension Professional Network via an email listserv. Individuals who returned a survey were given a $15 gift card. Only surveys with the majority (≥ 51%) of questions completed were included in the analysis, leading to the removal of 12 surveys.
Survey content
A custom 32-question survey (see Appendix 1) was designed to assess participants’ current attitudes and practices of genetic counseling and genetic testing for PAH, knowledge on the genetics of PAH, and demographics. Physicians who treat patients with PAH reviewed and edited the survey before distribution. It comprised 14 Likert scale (10 point), 13 multiple-choice, four free-text, and one rank-order questions. A Likert scale is a common tool used to evaluate variables that are continuous in nature. 29 In this study, the Likert scale questions were designed to quantify the participants’ attitudes and practices about genetic counseling, genetic testing, and perceived knowledge about the genetics of PAH. The multiple-choice questions were used to discover the participants’ practices of genetic counseling and genetic testing as well as their demographics and knowledge about the genetics of PAH. The rank-order question allowed participants to rank six options from most important to least important regarding what would lead them to order genetic testing for PAH more frequently.
Statistical analysis
JMP version 9 statistical software was used to analyze the data collected. Results were analyzed descriptively with categorical data reported as percentages and frequencies, continuous data reported as mean ± standard deviations, and non-parametric data reported as medians and interquartile ranges (IQR). As Likert responses were not normally distributed, non-parametric statistics were used. Spearman’s rank correlation coefficient was used to find relations between frequencies and attitudes. Comparison of groups was performed with the Wilcoxon rank-sum test.
Results
Participants
Demographics of participants.
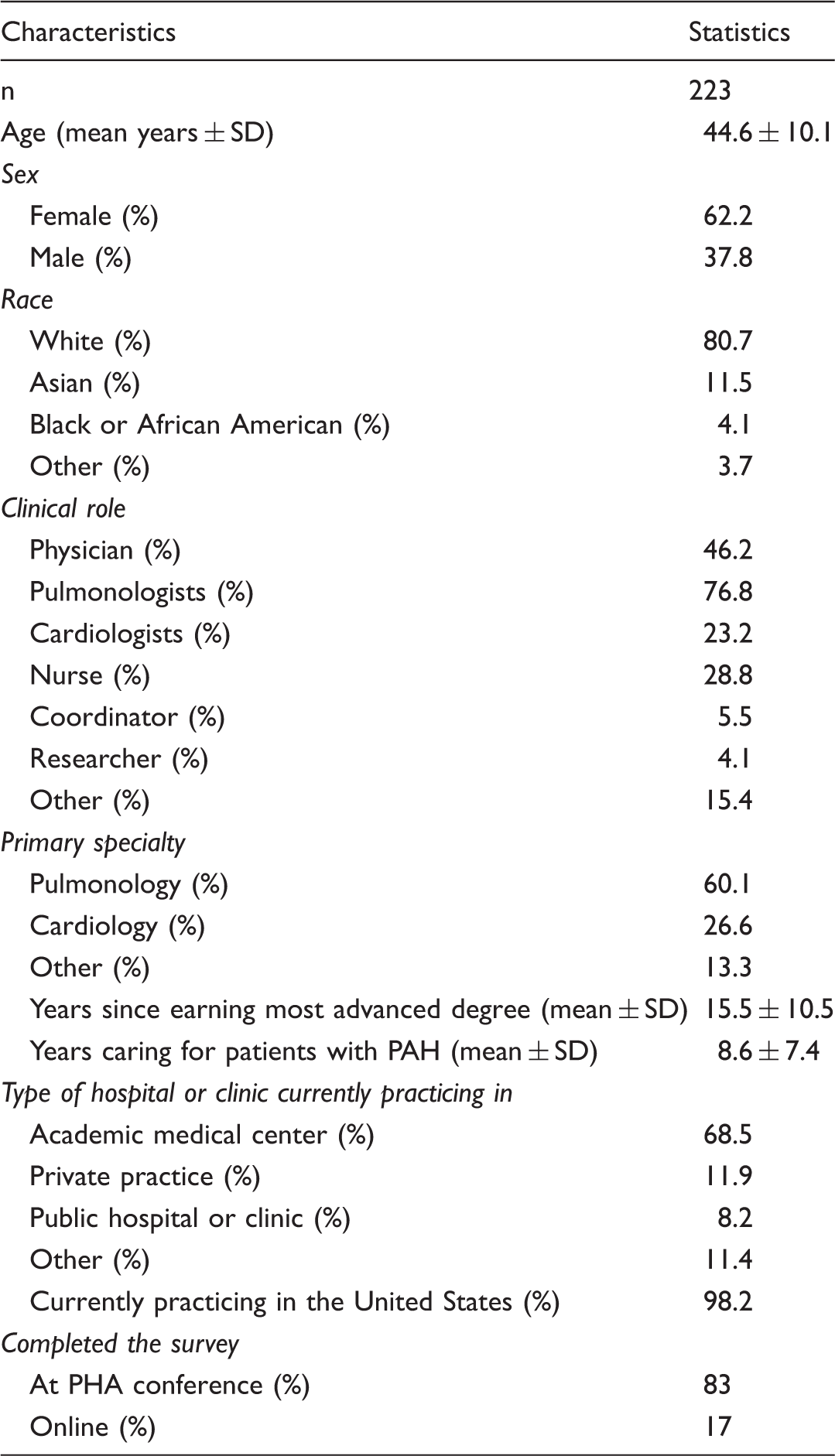
SD, standard deviation.
Knowledge of the genetics of PAH is low
Five survey questions were used to gauge the participants’ understanding of the genetics of PAH. When asked how knowledgeable they considered themselves on the genetics of PAH, only 13.2% felt that they were knowledgeable (8 or higher on the Likert scale) (Fig. 1a and b). Physicians (Fig. 1a) perceived themselves to be significantly more knowledgeable than non-physicians (Fig. 1b) with a median Likert score of 5 (IQR = 3.5–7) compared to non-physicians who responded with a median Likert score of 3 (IQR = 2–5) (P < 0.0001). The participants were given four questions to directly test their knowledge with only 27% of all respondents correctly answering three or more questions (high actual knowledge). Fig. 1c and d show how the high actual knowledge for physicians and non-physicians, respectively, compared to the perceived knowledge while Fig. 1e and f show the low actual knowledge as compared to perceived knowledge for the two subgroups. Of the physicians, 43.6% (45/103) answered three out of the four questions correctly which is significantly more than the 13.3% of non-physician participants (16/120) who answered three out of the four questions correctly (P < 0.0001).
Participants’ perceived and actual knowledge about the genetics of PAH. Perceived knowledge was generally low to moderate with more than 50% of the respondents having a perceived knowledge of 5 or less (a, b) with perceived knowledge less in non-physicians (b) than in physicians (a). However, among all respondents, individuals who got at least 75% of the objective questions correct (high actual knowledge) had significantly (P < 0.0001) higher perceived knowledge (median = 6, IQR = 4–7.8) than individuals who answered less than 75% of the objective questions correct (low actual knowledge) (median = 3, IQR = 2–5). There were some individuals who exhibited disparities between perceived and actual knowledge (e.g. low perceived but high actual and high perceived but low actual. For example, over 20% of physicians with low actual knowledge had a perceived knowledge of 8 or higher (e). On the other hand, over 30% of non-physicians with high actual knowledge had a perceived knowledge of 3 or less (d). Physicians (a, c) had a higher perceived and actual knowledge when compared to non-physicians (b, d).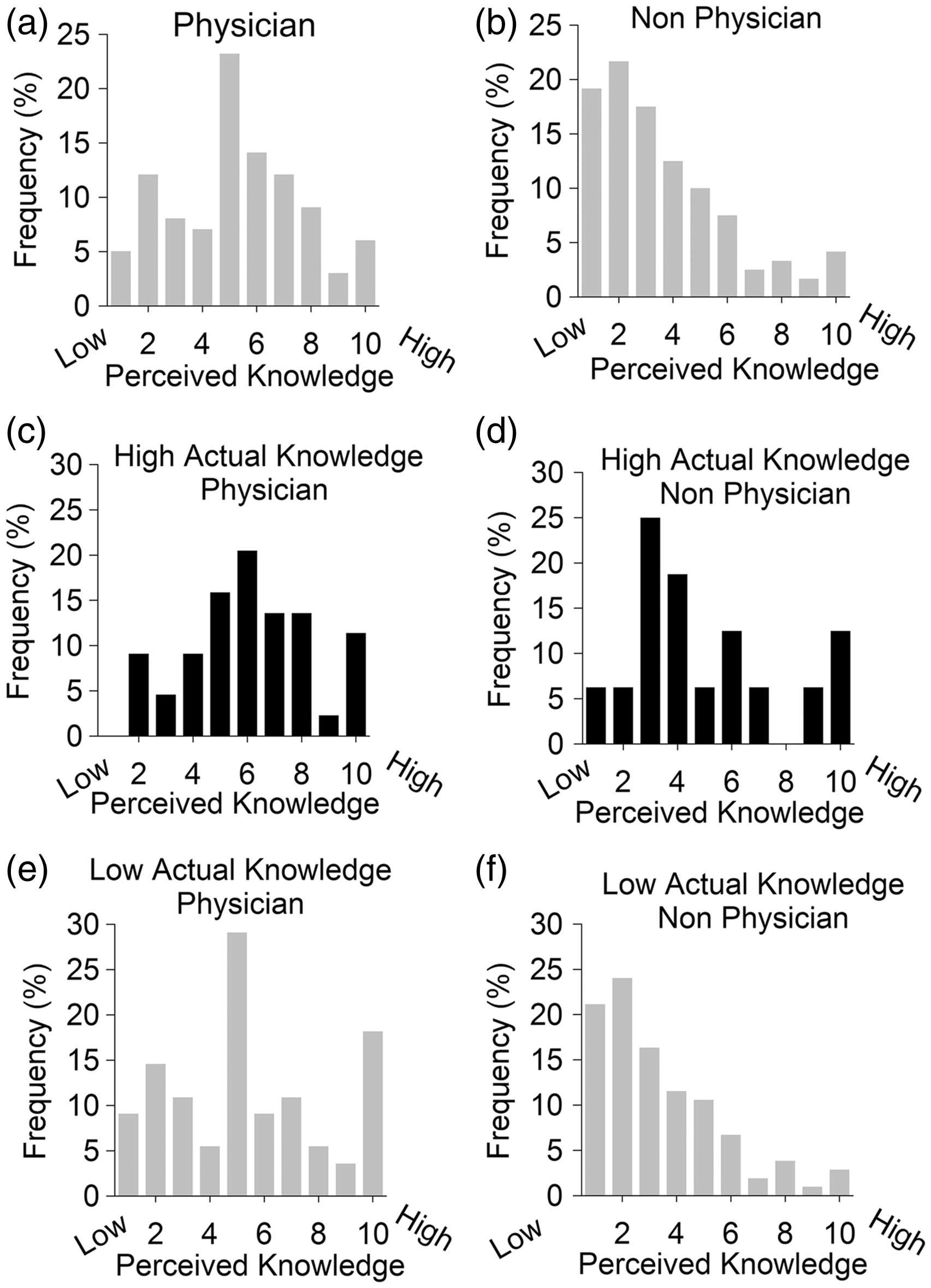
PAH specialists have poor practice patterns but positive attitudes about genetic counseling and genetic testing
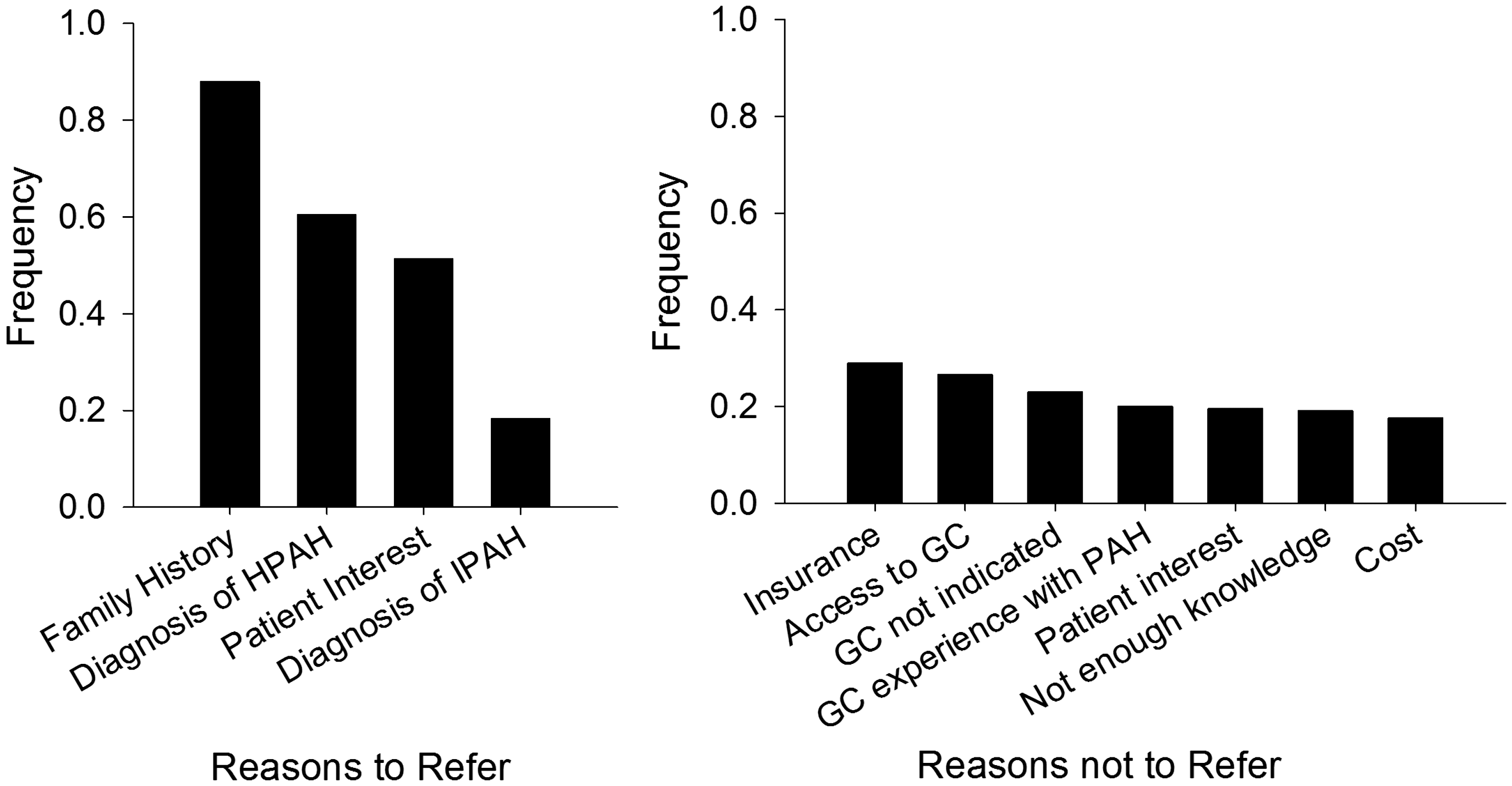
The majority (79.1%) of participants responded that they never or rarely (3 or lower on the Likert scale) refer their patients with PAH to a genetic counselor (Fig. 2). The two most common reasons for not referring their patients with PAH to genetic counselors were: (1) insurance companies not covering the cost; and (2) lack of access to genetic counselors at the participants’ institution. Of those who never refer their patients with PAH to genetic counselors, 20% feel this service is not indicated. Of those who do refer their patients to genetic counselors, the most common reasons were either the patient having a family history of PAH and/or the patient having a diagnosis of HPAH (Fig. 3). Over half of the participants (53%) stated that genetic counseling should always or almost always (8 or high on the Likert scale) be offered along with genetic testing.
Frequency of referrals to a genetic counselor and ordering genetic testing. Almost 80% of all participants never or rarely (1–3 on the Likert scale) refer their patients with PAH to a genetic counselor or order genetic testing for PAH. GC, genetic counselor; GT, genetic testing. Participants’ reasons for and for not referring their patients with PAH to a genetic counselor. The most common reason for participants to refer their patients with PAH to a genetic counselor was due to a family history of the disease. An insurance issue(s) was the biggest barrier though for our participants to refer. HPAH, heritable pulmonary arterial hypertension; IPAH, idiopathic pulmonary arterial hypertension; GC, genetic counselor.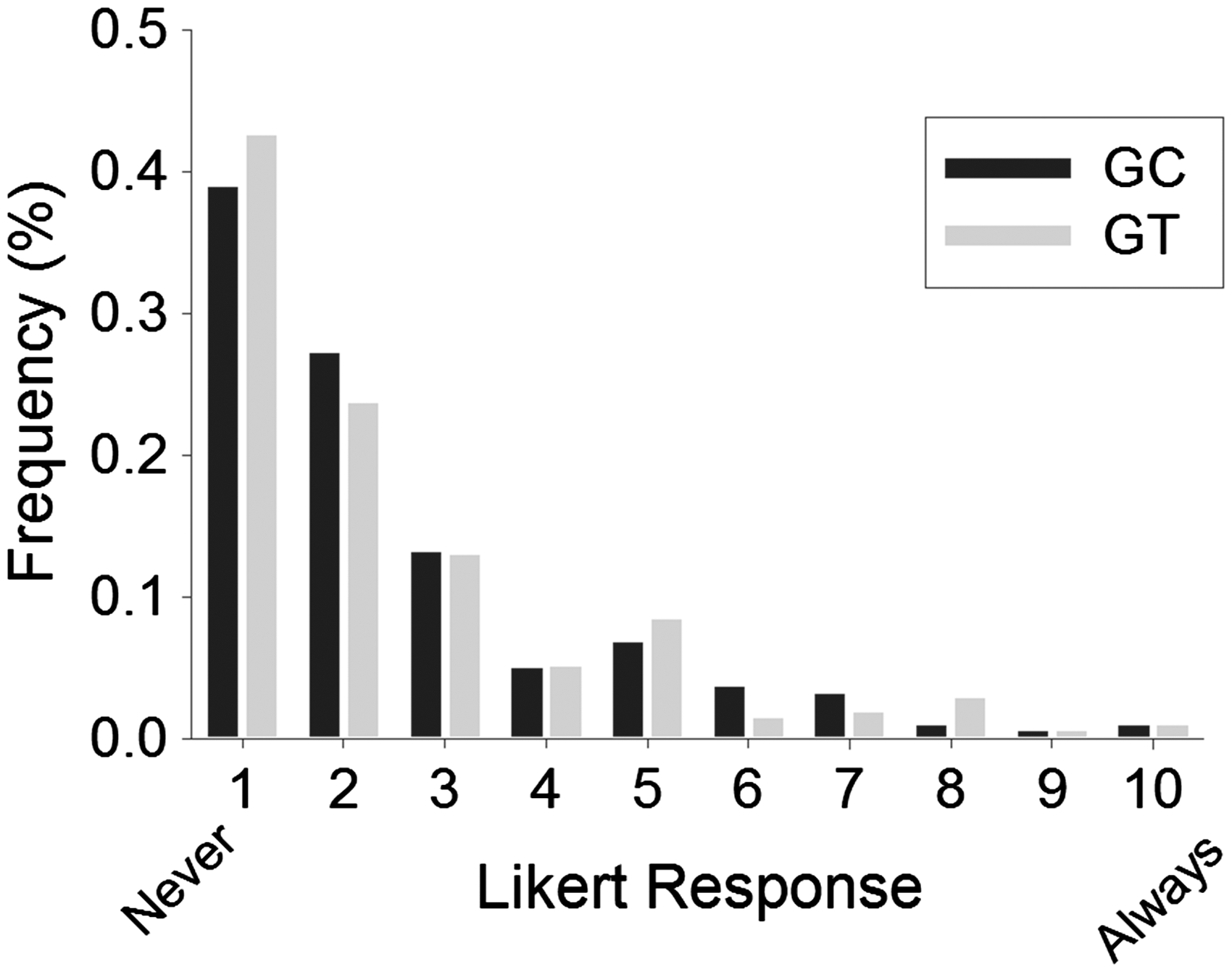
To understand the relationship between referral frequency and attitudes towards genetic counseling, correlation analyses were performed (Fig. 4a). Patients inquiring about genetic counseling was the most strongly correlated factor (ρ = 0.54, P < 0.0001) associated with genetic counseling referral frequency. This was followed by respondents viewing genetic counseling as an important component to medical management (ρ = 0.38, P < 0.0001).
Moderate to weak correlations found between perceptions of genetic services and referrals to genetic counselors (a) and ordering frequency of genetic testing (b). Patients asking and our participants seeing genetic counseling (a) and genetic testing (b) as an important component to medical management were the most strongly correlated factors when ordering genetic services.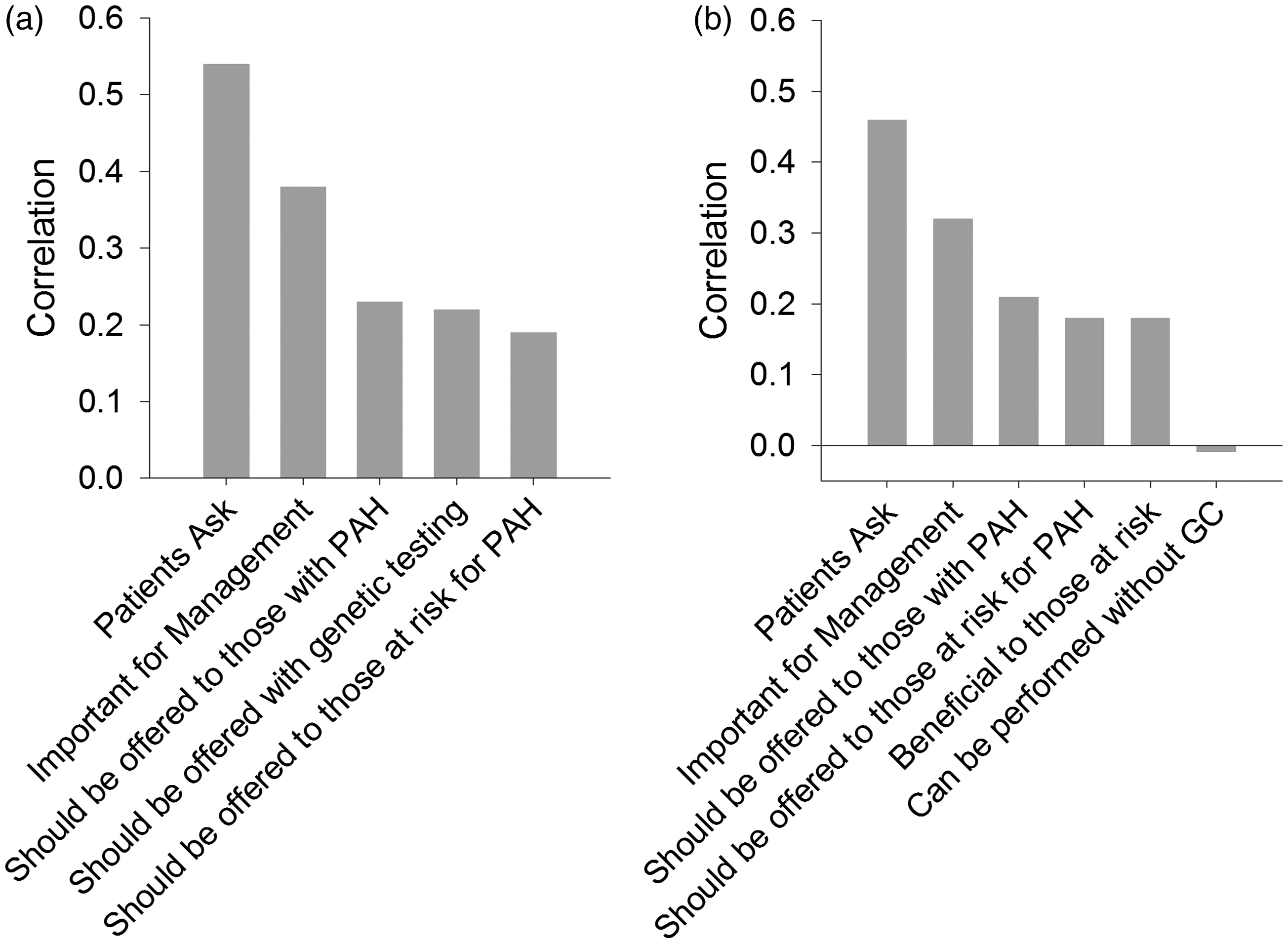
The majority (79.2%) of participants stated that they never or rarely (3 or lower on the Likert scale) order genetic testing (Fig. 2). The two most common reasons they do not order genetic testing were: (1) insurance companies not covering the cost; and (2) the tests being too expensive (Fig. 5). Nearly half (42.6%) of all survey participants completely disagreed that genetic testing can be offered without genetic counseling (1 on the Likert scale) with another 36.6% mostly disagreeing (2 or 3 on the Likert scale). Approximately 25% of the participants do not recommend genetic services because they do not feel it is necessary or warranted. The survey did not allow the reasons for this belief to be explored.
Participants’ reasons for not ordering genetic testing. Insurance issues and the cost were the two most common reasons preventing participants from ordering genetic testing for PAH.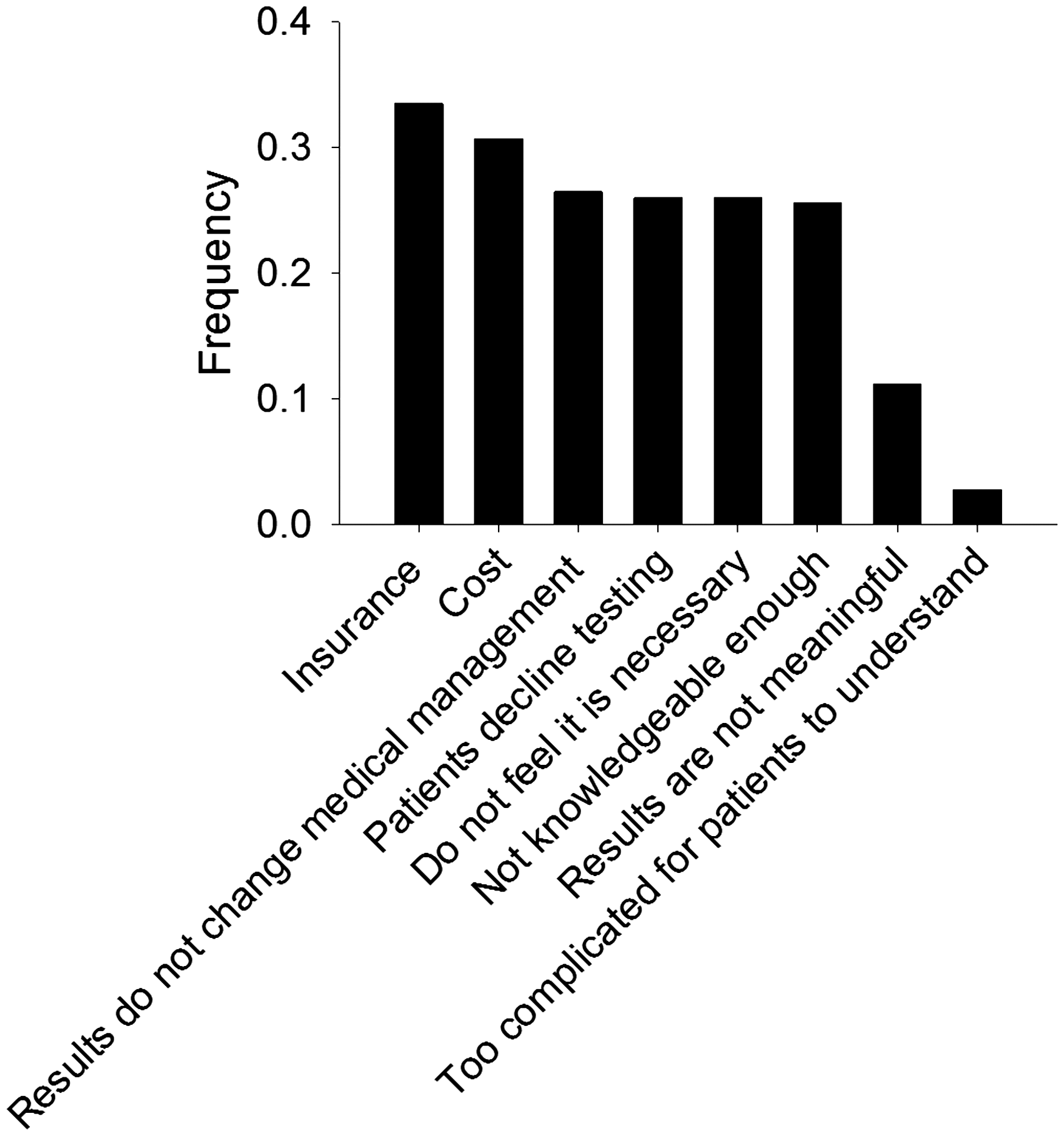
Correlation analyses were performed to identify relationships between the frequency that genetic testing for PAH is ordered and participants’ attitudes about genetic testing (Fig. 4b). Similar to the genetic counseling results, patients inquiring about genetic testing was the most strongly correlated factor associated with genetic testing ordering frequency (ρ = 0.46, P < 0.0001). This was followed by respondents viewing genetic testing for PAH as an important component to medical management (ρ = 0.32, P < 0.0001).
When asked to rank six options that would lead participants to order genetic testing for PAH more frequently, the majority felt that having better insurance coverage with minimal out-of-pocket expenses for the patients would be the most beneficial. This was followed by the availability of genetic counselors at their facilities, specifically genetic counselors that are knowledgeable about the genetics of PAH. The use of media resources such as an educational video or brochure and the ability to perform genetic testing for PAH on a saliva sample were found to be the least beneficial.
Physicians have low utilization and perception of the utility of genetic counseling and genetic testing
Likert genetic counseling and genetic testing responses between physicians and non-physicians.
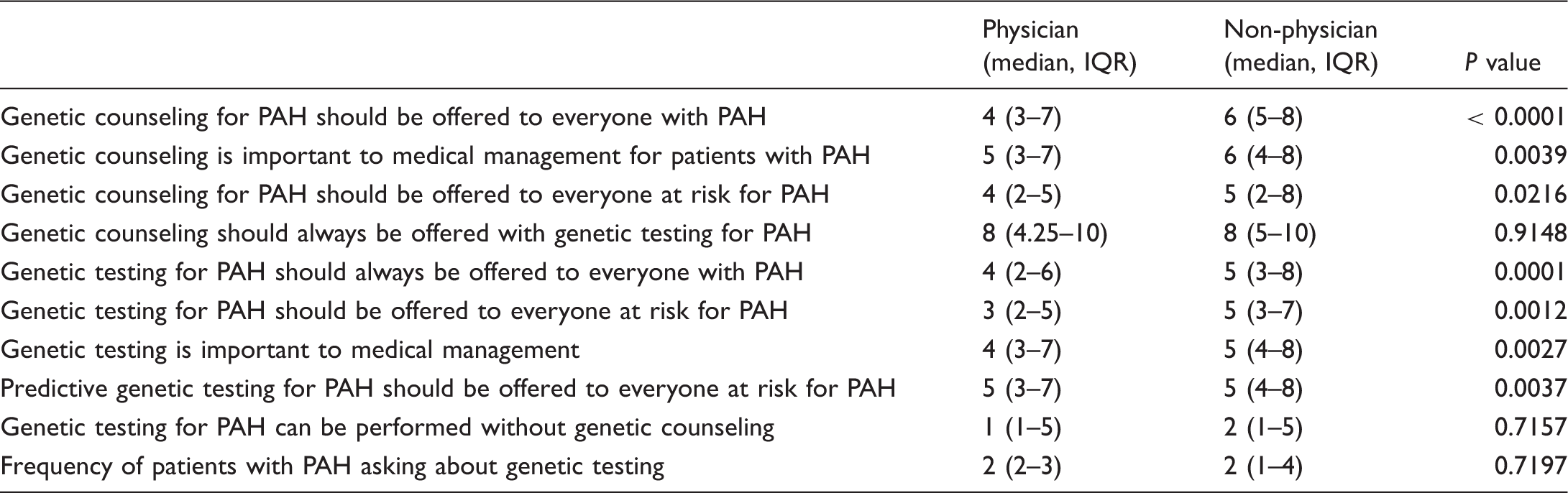
Tenpoint Likert scale: 1 = disagree, 10 = agree.
IQR, interquartile range; PAH, pulmonary arterial hypertension.
Likert genetic testing responses between cardiologists and pulmonologists.
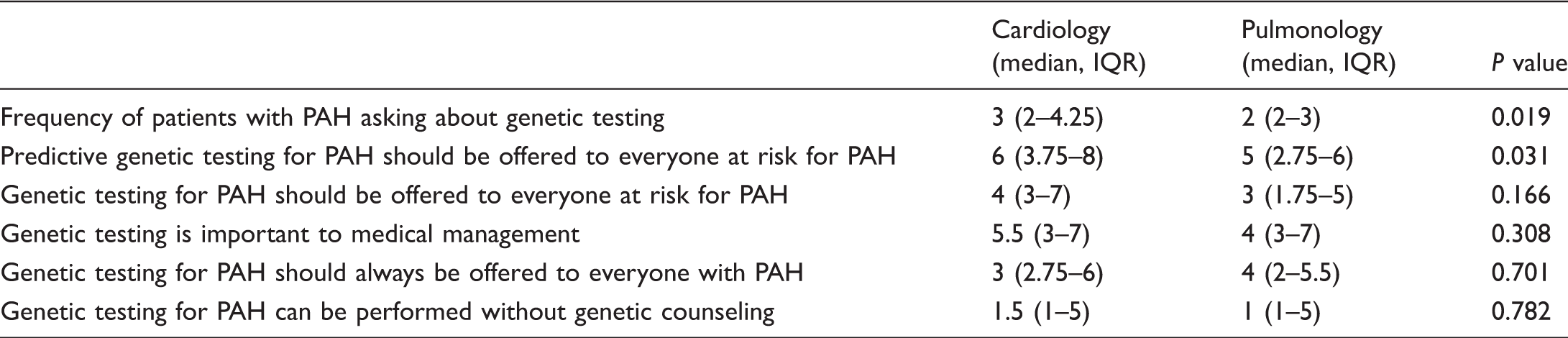
Ten-point Likert scale, 1 = disagree, 10 = agree.
IQR, interquartile range; PAH, pulmonary arterial hypertension.
Discussion
Current practice guidelines and literature recommend genetic counseling and offering genetic testing to individuals with HPAH, IPAH, and their family members.20–25 Although these guidelines exist, utilization frequency of genetic counseling and genetic testing for PAH is not known. Our study shows that there is a disparity between recommended guidelines and actual practice as well as low knowledge base about the genetics of PAH among clinicians practicing in the USA. Using a custom survey, we collected information from 223 PAH specialists. Only 27% of participants were knowledgeable about the genetics of PAH and nearly 80% of our participants stated that they never or rarely utilize genetic services for PAH. This apparent low utilization of genetic services and lack of knowledge about the genetics of PAH seem to be driven by a perceived lack of benefit of genetic counseling and genetic testing for patients with PAH. By these specialists becoming more knowledgeable about the genetics of PAH and the genetic services available, it might lead to a better standard practice of care.
We found that approximately 80% of participants stated that they never or rarely refer their patients to a genetic counselor or order genetic testing. This is in direct contrast of the guidelines that recommend genetic counseling to individuals with HPAH, IPAH, and their family members. For more than 20% of individuals diagnosed with PAH, it took more than two years for them to receive a diagnosis. 30 This two-year delay in treatment potentially allows symptoms to progress and result in a shorter life expectancy. 30 Treating patients with PAH when they are asymptomatic or just starting to show symptoms has been shown to delay further symptoms and improve pulmonary vascular resistance. 31 However, in order to start managing the care of asymptomatic individuals, their healthcare providers need to know who in a family is at risk for also developing the disease. PAH specialists can have family members who have a predisposing genetic mutation for PAH undergo a yearly echocardiogram and recommend they avoid certain drugs such as Aminorex, Fenfluramine, and selective serotonin reuptake inhibitors.13,14,24
Taking advantage of screening measures and recommendations early can help to discover the disease early and/or possibly delay symptoms. Other countries have implemented genetic services to all patients with PAH and PVOD into their clinics, most notably in France for the last 12 years. 16 Individuals in families in which PAH is segregating knowing whether they harbor a genetic mutation could have an impact on their reproductive choices including: deciding not to have children, adoption, in vitro fertilization with preimplantation diagnosis, or using a gamete donor.16–18 The use of pre-implantation diagnosis is used for preventing other severe incurable diseases such as Huntington’s disease. 16 However, using this technique for PAH is up for ongoing debate due to the disease’s unknown or incomplete penetrance depending on the disease-causing gene. It is through proper counseling that families can make informed reproductive decisions. Genetic testing can also be a useful tool in distinguishing between PAH and pulmonary venoocclusive disease (PVOD). 16
Physicians were significantly more knowledgeable about the genetics of PAH than non-physicians (P < 0.0001); however, only 43.6% of physicians were knowledgeable based on this study’s survey. Cardiologists and pulmonologists are not alone in this. Low genetics knowledge has been seen in other specialties such as oncologists and general care physicians regarding familial cancer syndromes.32–34 Low utilization of genetic services could be due to the survey participants’ self-acknowledged lack of knowledge about the genetics of PAH based on a moderate correlation found between perceived knowledge and genetic services referral frequency (ρ = 0.34 for genetic counseling, ρ = 0.30 for genetic testing). When patient access to genetic services is greatly dependent on referrals from physicians, the physicians need to become more aware of the constantly evolving genetic literature about PAH in order to meet the needs of their patients. A study that specifically looked at what patients think about genetic testing for the gene BMPR2 showed that 71% of people diagnosed with or at risk for PAH knew almost nothing or only a little bit about the genetic testing options available to them. 27 Of these individuals, only 50% learned about the genetic components of PAH from their doctor; the rest learned from other sources such as family members, research studies (including the one described), the PHA, and the Internet. 27 In order for individuals with PAH to receive the most accurate information about the genetics of this disease, PAH specialists need to remain fluent with the genetic aspects of the disease in order to best counsel families.
It was found that cardiologists have more favorable attitudes about genetic services when compared to pulmonologists. Genetic services have been widely adopted in the cardiology field for such conditions including but not limited to dilated and hypertrophic cardiomyopathy. This could be the reason why cardiologists had more favorable attitudes and practices because there has been more awareness made about the genetics of cardiac conditions. Although cardiovascular genetics is a rapidly growing field, cardiologists were found to be most concerned with how to properly interpret genetic testing results, specifically variants of uncertain clinical significance. 35 For pulmonary diseases, there are fewer commercial genetic testing options available compared to those options for cardiac diseases. This may make it more difficult for pulmonologists to have favorable attitudes and practices of genetic services if there is little opportunity to utilize the services. We believe that once there are more options available for pulmonologists to utilize genetic services, their attitudes and practices will improve.
In our survey targeting clinicians and researchers, participants had ambivalent or positive attitudes about genetic testing and genetic counseling. These attitudes led us to question what is influencing our participants’ practice patterns. The correlation analyses revealed that patients with PAH asking about genetic testing and genetic counseling was the most highly correlated factor on our participants’ referral and ordering frequency. This poses a problem since most individuals with PAH or at risk for PAH know almost nothing or only a small amount about the genetics of PAH. 30 When we asked our participants about their reasoning for not utilizing genetic services, the most common answers were the cost of the services and lack of insurance coverage. Today, there are genetic panels specifically designed for diagnosing HPAH offered by commercial labs. Some of these labs accept commercial insurances and Medicare in addition to having discounted prices for those who do not have insurance. Knowledge of insurance verification and out-of-pocket costs is the responsibility of the ordering providers. This should be discussed with the patient before testing is sent. If a genetic mutation is identified in a tested patient/individual, mutation specific testing can be ordered on family members that is typically a fraction of the cost of full gene sequencing or panel testing.
Although genetics research on PAH is relatively new compared to other genetic diseases, future treatments could be dependent upon the specific variants in an individual’s genome. Personalized medicine as a result of genetic testing is used in other genetic disorders such as cystic fibrosis and certain cancers.36,37 The ability to prescribe a specific therapy for PAH based on the presence/absence of a specific genetic alteration could be a possibility several years from now. Today, however, we are still learning about the different mutations that exist in at least seven genes associated with the development of PAH as well as discovering new genes and genetic associations/interactions. As additional genes and genetic associations are identified, it will be essential that PAH specialists become more knowledgeable about the genetics of PAH and the testing options available in order to one day better manage the care of their patients.
Limitations
Participants who returned the survey may have had more thorough understanding of the genetics of PAH as compared to other PAH specialists who may not have felt as knowledgeable and, therefore, did not return the survey. This could have led to a higher calculated knowledge than what is actually reflective of all healthcare providers who treat patients with PAH. We also surveyed researchers, nurses, and healthcare coordinators; however, typically only physicians are the ones who refer patients with PAH to genetic counseling or order genetic testing. This could mean that there is more genetic testing being ordered than what our results show even though we did not have any significant differences in ordering or referral frequency for genetic testing or genetic counseling between physicians and non-physicians. It is unknown how many of our respondents provided care to pediatric versus adult patients, which could potentially influence knowledge, practice, and attitudes. We could have had multiple respondents from the same institution who may potentially share a common discipline towards utilization of genetic services. Of our 223 respondents, 4.1% were researchers. Since researchers do not typically charge for genetic testing, this could influence the reason of “cost for testing” as a reason to not order it. Lastly, we did not keep track of how many surveys were distributed at the PHA conference thus preventing us from determining a response rate.
Conclusion
Our results suggest that increased education and awareness is needed about the genetics of PAH as well as the benefits of genetic testing and genetic counseling for PAH specialists. Currently, genetic services will not change the medical management for the individual with PAH, but it can help to discriminate between other similar disorders to PAH such as PVOD. If a disease causing genetic mutation associated with PAH is found in an unaffected family member, then he or she can manage their risk by undergoing yearly echocardiograms and avoiding certain drugs. By finding this information out earlier rather than later, asymptomatic individuals with a predisposing genetic mutation for PAH may have the ability to delay symptoms, make more informed reproductive choices, and potentially prolong their lives.