
Abstract
Background:
Inadequate adherence to antipsychotic medication remains a major driver of relapse, hospitalization, and chronic disease progression in schizophrenia. Long-acting injectable (LAI) antipsychotics may reduce healthcare costs and the risk of relapse. However, evidence regarding the switch from paliperidone palmitate once every month (PP1M) to paliperidone palmitate once every 3 months (PP3M) remains limited.
Objectives:
To examine the utilization of LAI antipsychotics and investigate the effect of transitioning from PP1M to PP3M on adherence and healthcare utilization.
Design:
This retrospective, 12-month mirror-image study used nationwide, population-based data from Taiwan to examine changes in healthcare resource utilization and costs after the transition from PP1M to PP3M.
Methods:
Individuals with schizophrenia who were newly prescribed PP3M after receiving PP1M for at least 12 months between 2016 and 2021 were included. Healthcare resource utilization and costs during the 12 months before PP3M initiation were compared with those during the 12 months after initiation. Risk factors for an unsuccessful transition from PP1M to PP3M were also identified.
Results:
Among the 4001 patients with schizophrenia spectrum disorders included in this study, 2790 (69.7%) continued PP3M treatment. A younger age, residence in suburban or rural areas, lower concomitant use of other antipsychotics, and higher use of benzodiazepine were independent risk factors for an unsuccessful transition. At 12 months after PP3M initiation, hospitalization costs decreased from NT$38,469.0 to NT$20,062.8 and emergency room visit costs from NT$692.1 to NT$360.9 (both p < 0.001). The rates of outpatient visits, emergency room visits, and hospitalizations, the length of hospital stay, and total healthcare costs also decreased significantly (all p < 0.001).
Conclusion:
Transitioning from PP1M to PP3M for schizophrenia treatment can significantly reduce healthcare resource utilization and costs. Notably, hospitalization and emergency room visit costs were reduced by approximately half.
Plain language summary
1. Significant outcomes
This study demonstrated that transitioning from PP1M to PP3M treatment for schizophrenia can significantly reduce healthcare resource utilisation and costs. Notably, both hospitalisation and emergency room visit costs were reduced by approximately half. Furthermore, this study showed that even among patients who discontinued PP3M, healthcare costs were still reduced in the 12 months after the initiation of PP3M treatment compare with the 12 months before.
2. Limitations
This retrospective mirror-image study lacked a contemporaneous comparator group.
Potential biases such as temporal and selection biases cannot be rules out.
Each patient in the mirror-image study serves as their own control, and observed changes from pre- to post-introduction may partly reflect regression to the mean.
Introduction
Schizophrenia is widely regarded as a severe, chronic mental illness that affects nearly 24 million (0.32%) people globally. 1 In addition, it ranks among the 20 most prominent causes of disability because its relapse-prone nature and chronic course place a considerable burden on patients, carers, and healthcare systems.2–4 Inadequate adherence to antipsychotic therapy is a key factor underlying relapse, hospitalization, and the chronic progression of schizophrenia; up to 50% of patients experience difficulty maintaining consistent adherence to daily oral antipsychotic regimens.5–7
As a clinically effective alternative to once-daily oral antipsychotics, long-acting injectable antipsychotics (LAIs) are associated with improved adherence because they provide sustained drug delivery and require less frequent administration.8–10 Paliperidone palmitate is a second-generation antipsychotic that can be administered once per month (PP1M), once every 3 months (PP3M), or once every 6 months, and it has demonstrated efficacy in preventing relapse and supporting functional stabilization in schizophrenia cases.11–13 Transitioning from PP1M to PP3M constitutes an advancement in LAI therapy because it reduces the injection frequency from 12 to 4 times per year, which may improve patient convenience and satisfaction and simultaneously maintain therapeutic continuity.
The economic burden of schizophrenia includes direct healthcare costs, such as those related to hospitalization, emergency room visits, outpatient department visits, and pharmacy expenses; direct non-healthcare costs, such as those related to law enforcement and shelters for homeless individuals; and indirect costs, such as those arising from care provision, decreased productivity, unemployment, and premature death. 14 In the United States, schizophrenia is associated with an estimated annual economic burden of over US$150 billion, with hospitalization accounting for the largest proportion of direct healthcare costs.14,15 A previous study reported that the use of LAIs instead of oral antipsychotics is associated with lower hospitalization rates and healthcare resource utilization. 16 Furthermore, compared with PP1M, PP3M requires fewer injections, which may reduce administrative workload, transportation demands, and the frequency of clinical visits. 17 Several real-world studies have demonstrated that the use of PP3M instead of PP1M in schizophrenia treatment is associated with improved clinical outcomes and reduced healthcare resource utilization.18–21 However, evidence regarding PP3M treatment for schizophrenia in Asian populations remains limited.22–24 Although several studies have evaluated the cost-effectiveness of PP3M in schizophrenia,17,23–31 only one small pilot study specifically examined healthcare costs related to the switch from PP1M to PP3M in an Asian population. Hence, additional studies on this topic are warranted. 31
To address the aforementioned research gap, we conducted a 12-month mirror-image study using Taiwan’s National Health Insurance Research Database (NHIRD), a nationwide, population-based claims dataset, to examine clinical and economic outcomes associated with the transition from PP1M to PP3M for schizophrenia treatment. This study also identified risk factors for an unsuccessful transition from PP1M to PP3M.
Methods
Data sources and ethics statement
We collected from the NHIRD (a comprehensive real-world database) deidentified, population-level, claims-based data covering the 2016–2022 period. The NHIRD provides detailed information on the clinical characteristics of individuals covered by Taiwan’s National Health Insurance program; this program has included >99.6% of Taiwanese population (nearly 23 million individuals) since its inception on March 1, 1995. 32 The Taiwan Ministry of Health and Welfare’s Health and Welfare Data Science Center manages the data used in this study.
Study design and patients
We conducted a retrospective 12-month mirror-image study comparing healthcare resource utilization and costs during the 12 months before and the 12 months after the initiation of PP3M treatment in individuals with schizophrenia between 2016 and 2022. Patients were enrolled if they had a diagnosis of a schizophrenia spectrum disorder at any time during the study period and had received at least one new prescription of PP3M between January 1, 2016, and December 31, 2022. Diagnoses were identified using International Classification of Diseases, Ninth Revision, Clinical Modification code 295 or International Classification of Diseases, Tenth Revision, Clinical Modification codes F20 and F25. To enhance diagnostic validity, only patients with an inpatient record listing a schizophrenia spectrum disorder as a primary or secondary diagnosis or with at least three consistent outpatient diagnoses of a schizophrenia spectrum disorder were included.
Patients were excluded if they were younger than 15 years, lacked complete outpatient data for the 12 months before and 12 months after PP3M initiation, died during the study period, or initiated PP3M between January 1 and December 31, 2016. The mirror point (index date) was defined as the date of PP3M initiation. All patients had received PP1M for at least 12 months before the index date and thus underwent a transition from PP1M to PP3M. Transition was considered successful if a patient received three to five PP3M injections during the 12 months after receiving a PP3M prescription. In this study, a rate of administration of more than three to five injections indicates a regimen closer to PP1M, and anything less indicates medication nonadherence. Patients who successfully transitioned from PP1M to PP3M were defined as successful transition users (PP3M continuers); they were those prescribed three to five PP3M injections within the 12-month follow-up period. Patients who did not meet these criteria were defined as unsuccessfully transition users, including PP3M discontinuers and PP3M improper users. PP3M discontinuers were defined as patients who received one or two PP3M injections during the follow-up period, whereas PP3M improper users were defined as patients who received more than five PP3M injections during the same period.20,25 All patients received standard clinical care, and PP3M prescribing decisions were independently made by the treating physician. The reporting of this case study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 33
Variables examined in this study
The variables examined were the demographic characteristics of the patients, diagnosis of schizophrenia spectrum disorder, concomitant use of oral psychiatric medications, number of PP3M injections, level of healthcare resource utilization, healthcare costs incurred, and other relevant medical information. Healthcare costs were defined as direct healthcare expenditures, including pharmacy and medical service costs. Medical costs were defined as expenses related to emergency room visits, outpatient department visits, hospitalizations, home visits, and other medical services.14,17
Sensitivity analysis
To evaluate the robustness of our primary findings and address potential temporal or secular-trend biases inherent in the mirror-image design, we conducted three sensitivity analyses. First, we used a multiple linear regression model with adjustment for relevant covariates, including age, sex, diagnosis, urbanization level, and concomitant use of benzodiazepine and other antipsychotics (Table S1). Second, we shortened the observation window to 6 months before and after the index date to reduce potential time-varying confounding (Tables S3 and S4). Third, to examine the potential effects of the COVID-19 pandemic and other system-level fluctuations, we include only patients whose index dates occurred on or after January 2020 (Tables S5 and S6).
Statistical analysis
Herein, we summarized categorical and continuous variables as frequencies (percentages) and means (standard deviations), respectively. Because continuous variables were observed to be nonnormally distributed in Student’s test, paired t-tests were conducted. A two-side p value of <0.05 was considered statistically significant, and all statistical analyses were conducted using SAS, version 9.4 (SAS Institute, Cary, NC, USA).
Results
Clinicodemographic characteristics
In this study, 4001 individuals with schizophrenia who received at least one new prescription of PP3M during the 2016–2021 period were identified. Figure 1 presents the patient selection flowchart, and Table 1 presents a summary of their baseline clinicodemographic characteristics. The mean age of the study population was 44.7 ± 12.1 years. Of the included individuals, 1982 (49.5%) were men, 3756 (93.9%) were unemployed, and 2330 (58.2%) resided in urban areas. Schizophrenia was the most common diagnosis (69.8%), followed by schizoaffective disorder (30.2%). In addition to receiving PP1M and PP3M prescriptions, 3709 (92.7%) patients received prescriptions for concomitant oral psychiatric medications. The most commonly prescribed medications were benzodiazepines (84.5%), other antipsychotics (74.3%), antidepressants (36.2%), and mood stabilizers (30.6%). During the 12-month study period, 1685 (42.1%) patients received five PP3M injections, 831 (20.8%) received one injection, and 812 (20.3%) received four injections.

Flowchart of the participants’ selection process for the study.
Baseline characteristics of study population (N = 4001).

43 (1.1%) participants were unable to provide residence information.
ADR, adverse drug reaction; SD, standard deviation.
Comparison between successful and unsuccessful transition users from PP1M to PP3M
The baseline characteristics of successful and unsuccessful transition (from PP1M to PP3M) users are presented in Table 2. Of the 4001 included individuals, 2790 (69.7%) were classified as successful transition users and 1211 (30.3%) as unsuccessful transition users. Compared with the successful transition users, the unsuccessful transition users were significantly younger (43.5 vs 45.2 years), had a higher proportion of schizoaffective disorder diagnoses (32.5% vs 29.3%), were more likely to reside in suburban or rural areas (53.3% vs 41.6%), had lower rates of concomitant use of other oral antipsychotics (68.0% vs 77.0%), and had higher rates of mood stabilizer (37.6% vs 27.6%) and benzodiazepine use (86.5% vs 83.6%). In the multiple linear regression analysis, unsuccessful transition was significantly associated with a younger age (p = 0.0275), residence in suburban or rural areas (p < 0.001), lower use of other oral antipsychotics (p < 0.001), and higher use of benzodiazepines (p < 0.001; Table S1).
Baseline characteristics of successful transition users and unsuccessful transition users from PP1M to PP3M.
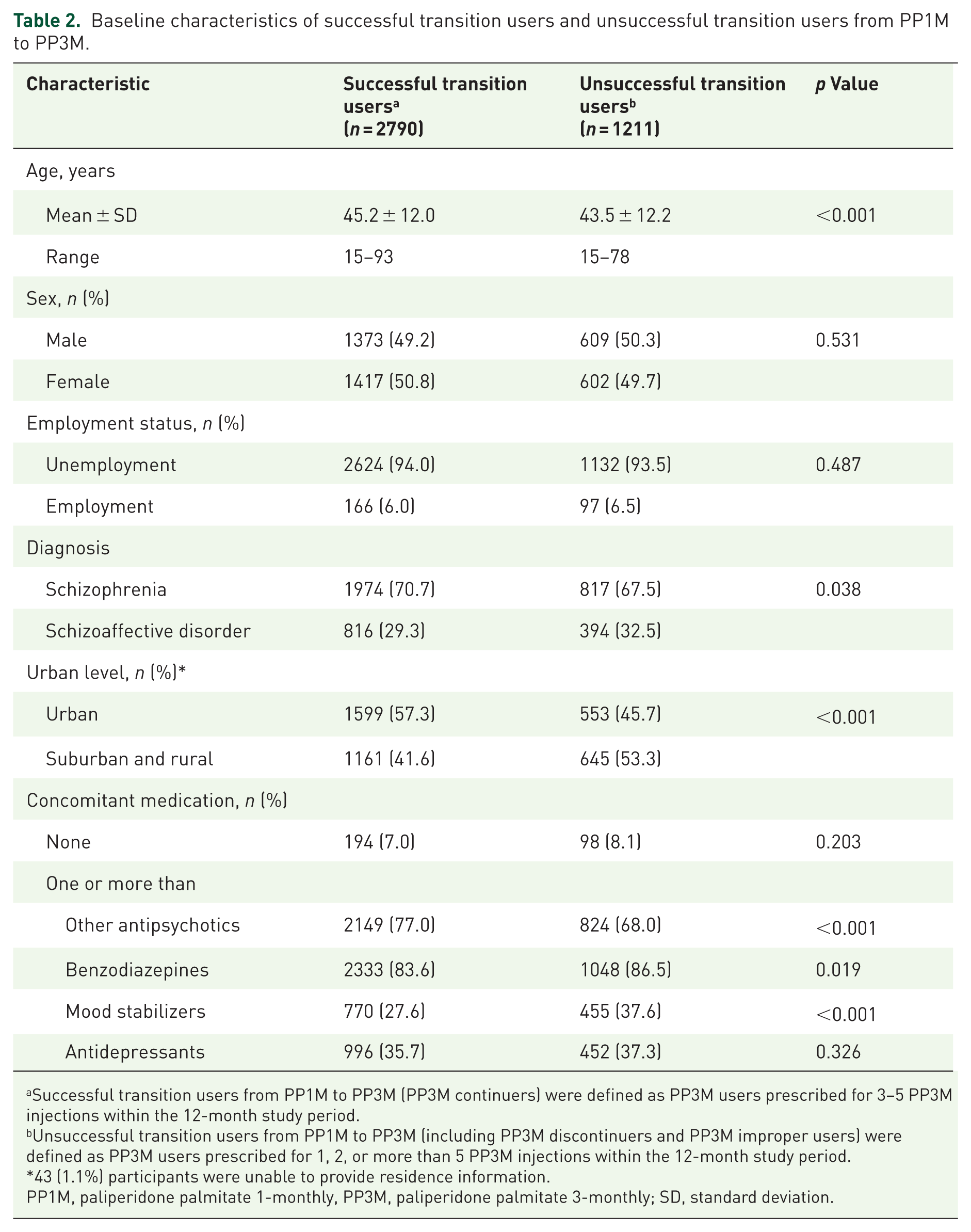
Successful transition users from PP1M to PP3M (PP3M continuers) were defined as PP3M users prescribed for 3–5 PP3M injections within the 12-month study period.
Unsuccessful transition users from PP1M to PP3M (including PP3M discontinuers and PP3M improper users) were defined as PP3M users prescribed for 1, 2, or more than 5 PP3M injections within the 12-month study period.
43 (1.1%) participants were unable to provide residence information.
PP1M, paliperidone palmitate 1-monthly, PP3M, paliperidone palmitate 3-monthly; SD, standard deviation.
Resource consumption outcomes
During the 12 months before and after PP3M initiation, the successful transition users made an average of 12.0 and 9.3 outpatient visits, respectively (p < 0.001), and incurred outpatient visit costs of NT$104,886.5 ± NT$63,061.2 and NT$113,130.5 ± NT$49,866.6, respectively (p < 0.001). The average numbers of emergency room visits were of 0.2 and 0.1 during the 12 months before and after PP3M initiation, respectively (p < 0.001), with corresponding costs of NT$692.1 ± NT$2672.9 and NT$360.9 ± NT$2380.2 (p < 0.001). The average numbers of hospitalizations were 0.5 and 0.3 during the 12 months before and after PP3M initiation, respectively (p < 0.001), and the mean lengths of hospital stay were 12.5 ± 34.5 and 7.4 ± 32.4 days, respectively (p < 0.001); hospitalization costs were NT$38,469.0 ± NT$99,105.7 and NT$20,062.8 ± NT$81,846.1 during the corresponding periods (p < 0.001). Total healthcare costs were NT$144,047.6 ± NT$110,315.5 and NT$133,554.2 ± NT$94,990.0 during the 12 months before and after PP3M initiation, respectively (p < 0.001). These findings are summarized in Tables 3 and 4.
Healthcare resource utilization and healthcare costs of successful transition users before and after PP3M injection initiation within 12 months (n = 2790).

The USD/TWD exchange rate is 31.12 on November 13, 2025.
ER, emergency room visits; NT$ [TWD], New Taiwan dollars; OPD, outpatient department visits; PH, psychiatric hospitalization; PP3M, paliperidone palmitate 3-monthly; SD, standard deviation.
Healthcare resource utilization and healthcare costs of unsuccessful transition users before and after PP3M injection initiation within 12 months (n = 1211).

The USD/TWD exchange rate is 31.12 on November 13, 2025.
ER, emergency room visits; NT$ [TWD], New Taiwan dollars; OPD, outpatient department visits; PH, psychiatric hospitalization; PP3M, paliperidone palmitate 3-monthly; SD, standard deviation.
During the 12 months before and after PP3M initiation, the successful transition users made an average of 9.1 and 8.1 outpatient department visits, respectively (p < 0.001), and they incurred outpatient department visit costs of NT$61,614.0 ± NT$62,245.6 and NT$49,591.9 ± NT$54,963.5, respectively (p < 0.001). Total healthcare costs curing the 12 months before and after PP3M initiation were NT$129,226.3 ± NT$145,399.1 and NT$110,448.7 ± NT$144,690.8, respectively (p = 0.03). The number of hospitalizations, duration of hospitalization, and costs incurred from emergency room visits and hospitalization decreased nonsignificantly from the 12 months before to the 12 months after PP3M initiation, whereas the number of emergency room visits increased nonsignificantly.
Discussion
This study is the first to evaluate changes in healthcare costs associated with the transition from PP1M to PP3M for schizophrenia treatment using nationwide, population-based data from Taiwan; this study analyzed 4001 patients who received at least one new prescription of PP3M between 2016 and 2021. Approximately 70% of these patients continued PP3M treatment during the study period. An unsuccessful transition from PP1M to PP3M was independently associated with a younger age, residence in suburban or rural areas, lower concomitant use of other antipsychotics, and higher use of benzodiazepines. Among the successful transition users, all measures of healthcare resource utilization and healthcare costs, except for outpatient department visit costs, decreased significantly at 12 months after PP3M initiation. Notably, costs related to hospitalization and emergency room visits were reduced by approximately half.
Successful transition from PP1M to PP3M
The PP3M continuation rate of 69.7% observed in the present study is consistent with rates reported in three previous studies examining the transition from PP1M to PP3M.20,22,25 Specifically, a UK study reported a continuation rate of 81.5% over a 1-year follow-up period among 132 individuals with schizophrenia, 20 an open-label study reported a continuation rate of 71% over 17 weeks among 210 individuals, 22 and a large-sample Spanish study reported a continuation rate of ⩾90% over a 12-month follow-up period. 25 These findings indicate that the transition from PP1M to PP3M is associated with a high rate of treatment continuation when used as maintenance therapy for chronic schizophrenia. However, evidence regarding potential risk factors for an unsuccessful transition from PP1M to PP3M in patients with schizophrenia remains limited.
In the present study, several baseline characteristics were determined to be associated with an unsuccessful transition from PP1M to PP3M, including a younger age, residence in suburban or rural areas, lower concomitant use of other antipsychotics, and higher use of benzodiazepines. This phenomenon indicates that patients with lower cognitive function or poorer disease control are likely to unsuccessfully transition from PP1M to PP3M. The identified factors affecting PP3M transition are consistent with the findings from a survey conducted in China. In that survey, early improvements in Clinical Global Impression–Severity and Positive and Negative Syndrome Scale scores during the initial phase of PP3M treatment predicted a successful transition from PP1M to PP3M in patients with schizophrenia. 22 Overall, baseline clinical characteristics and early improvements in symptom control and functional outcomes may serve as useful clinical indicators of a successful transition from PP1M to PP3M.
Healthcare resource utilization
Schizophrenia is characterized by a high risk of relapse that is often accompanied by visits to medical facilities, including the emergency department. 34 Such visits require considerable healthcare resources. In the present study, we determined that a transition to PP3M was associated with a lower rate of emergency room visits, a finding consistent with those of previous studies.23,25,29–31 Although we could not investigate the underlying causes of recurrent emergency room visits, PP3M may help reduce emergency room utilization among patients with schizophrenia, thereby alleviating emergency department overcrowding, increasing hospital revenue, and reducing overall healthcare costs.35,36 On the basis of these findings, we conclude that PP3M may be an effective treatment option for managing schizophrenia from a healthcare resource utilization perspective, particularly among patients with poor adherence to antipsychotic treatment.
In addition to emergency room visits, hospitalization is a substantial component of direct healthcare costs and constitutes the largest contributor to such costs in the United States.14,15 Previous studies conducted in several developed countries have reported that PP3M treatment for chronic schizophrenia considerably reduced hospitalization rates.22,23,28–30 In the present study, a transition to PP3M was associated with a reduced frequency and duration of hospitalization. In our previous pilot study involving 46 patients with schizophrenia, a transition to PP3M was associated with a 46.8% reduction in hospital length of stay over a 24-month follow-up period. 31 A survey of US veterans with schizophrenia reported a 47.8% shorter hospitalization duration at 6 months after a transition to PP3M. 28 These findings are consistent with our results, which reveal a 40.8% reduction in hospital length of stay during the 24-month observation period after the transition to PP3M. These findings indicate that patients with schizophrenia who transition to PP3M are likely to have more effective symptom control, have a lower risk of relapse or decompensation, and experience greater functional remission.
Healthcare costs
Few studies have quantified the monetary gains associated with reductions in healthcare resources and utilization,23,25,28 and evidence remains particularly limited for PP3M transition in patients with schizophrenia.27–31 In our previous pilot study involving a small sample, individuals with schizophrenia receiving PP3M incurred 46% lower healthcare costs than did those receiving PP1M. 31 In addition, a study of 324 US veterans with schizophrenia reported healthcare cost savings of approximately 14.3% after their transition to PP3M. 28 A Dutch study reported 15.5% lower costs (€8781 vs €10,325) associated with PP3M compared with PP1M in the treatment of chronic schizophrenia. 30 Moreover, a Spanish study using data from the Spanish National Health System reported approximately 8.8% lower expected costs (€4780 vs €5244) with PP3M compared with PP1M. 29 These findings are in line with the 7.3% reduction in healthcare costs observed in the present study. Furthermore, even among PP3M discontinuers, healthcare costs decreased by 14.5% at 12 months after PP3M initiation when compared with costs during the 12 months before initiation. This finding may be due to delayed relapse or hospitalization after PP3M use relative to oral antipsychotic or PP1M use, even after treatment discontinuation. 37
Strengths and limitations
First, a key strength of the present study is its analysis of a nationwide, population-based cohort. Second, this study conducted a naturalistic, nonrandomized, open-label assessment of clinical utilization and healthcare costs. Third, this study’s mirror-image design allowed each patient to serve as their own control, thereby eliminating the need for a matched comparator group and reducing potential biases related to study participation. Overall, the findings of the current study may inform health policy decisions regarding the use of LAI antipsychotics for schizophrenia, particularly among ethnic Chinese populations.
This study has several limitations. First, a retrospective mirror-image study, it lacked a contemporaneous comparator group, which limited our ability to examine relative treatment efficacy. Second, temporal confounding, selection bias, and inflation effects could not be controlled for because the study population was limited to patients who had received PP1M for at least 3 months. The cohort included only outpatients who transitioned from PP1M to PP3M and had complete outpatient data for the 12 months before and after the 12 months after PP3M initiation. Although potential temporal, selection, and regression-to-the-mean biases were considered in this study, we performed a sensitivity analysis to provide more objective data. Third, changes observed between the preintervention and postintervention periods in mirror-image studies may indicate regression to the mean because each patient serves as their own control. Nonetheless, mirror-image designs are widely used to compare two treatments in the same individual. Fourth, differences in cultural and healthcare systems may limit the generalizability of the findings beyond Taiwan or other Asian settings. Finally, clinical outcomes were evaluated using indirect measures, namely emergency room visit frequency and hospitalization duration; that is because the NHIRD does not provide information on direct clinical outcomes, such as Positive and Negative Syndrome Scale (PANSS) or Clinical Global Impression–Severity (CGI-S) scores.
Conclusion
Our findings based on real-world data in Taiwan reveal that the switch from PP1M to PP3M in patients with schizophrenia was associated with lower healthcare resource utilization and healthcare costs. Notably, costs related to hospitalization and emergency room visits were halved after this transition. In addition, an unsuccessful transition from PP1M to PP3M was independently predicted by a younger age, residence in suburban or rural areas, lower concomitant use of other antipsychotics, and higher use of benzodiazepines.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253261419626 – Supplemental material for Healthcare resource savings from administering paliperidone palmitate once every 3 months instead of once every month for schizophrenia: a 12-month mirror-image analysis of real-world population-based data
Supplemental material, sj-docx-1-tpp-10.1177_20451253261419626 for Healthcare resource savings from administering paliperidone palmitate once every 3 months instead of once every month for schizophrenia: a 12-month mirror-image analysis of real-world population-based data by Ke-Fei Wu, Ya-Hui Yang, Chuan-Sheng Hung, Jui-Hsiu Tsai and Hung-Yi Chuang in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-2-tpp-10.1177_20451253261419626 – Supplemental material for Healthcare resource savings from administering paliperidone palmitate once every 3 months instead of once every month for schizophrenia: a 12-month mirror-image analysis of real-world population-based data
Supplemental material, sj-docx-2-tpp-10.1177_20451253261419626 for Healthcare resource savings from administering paliperidone palmitate once every 3 months instead of once every month for schizophrenia: a 12-month mirror-image analysis of real-world population-based data by Ke-Fei Wu, Ya-Hui Yang, Chuan-Sheng Hung, Jui-Hsiu Tsai and Hung-Yi Chuang in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.