
Abstract
Background:
The effectiveness of long-acting injectable (LAI) antipsychotics in preventing relapses of first-episode psychosis is currently debated.
Objectives:
The study aimed to investigate the number of psychiatric hospitalizations comparing the LAI cohort versus the oral cohort during different phases of the illness, pre-LAI treatment, during LAI treatment, and after LAI treatment.
Design:
A naturalistic study was conducted on two independent cohorts of early psychosis patients receiving treatment from a specific early intervention service. The first cohort comprised 228 patients who received LAIs, while the second cohort comprised 667 patients who had never received LAIs.
Methods:
This study was designed as a longitudinal observational study conducted within a naturalistic clinical setting in two cohorts of early psychosis patients. Repeated series ANCOVA (ANCOVA-r) was used to study the number of hospitalizations in the different study periods (T1 = from the date of the first psychiatric record to the beginning of the mirror period; T2 = the mirror period; T3 = from the LAI implementation to the LAI discontinuation; and T4 = from the LAI discontinuation to the end). In all cases, discontinuation of LAI involved the return to oral treatment. In all, 35 patients had not T4 as they were still on LAI treatment at the time of database closing (September 2020), and their data were not included in the analysis of the effect of the LAI discontinuation.
Results:
The patients in the LAI cohort were younger, more frequently males, presented more schizophrenia diagnoses, and had a higher number of hospitalizations (2.50 ± 2.61 versus 1.19 ± 1.69; p < 0.001) than the oral cohort. The number of hospitalizations at the end of the follow-up was higher in the LAI cohort [0.20 (standard deviation (SD)) = 0.79] versus 0.45 [SD = 0.45 (SD = 1.13); F(23.90), p < 0.001]. However, after the introduction of LAIs, the differences in hospitalization rates between the two cohorts became less pronounced. Once LAI treatment was ceased, the hospitalization rate increased again.
Conclusion:
In our study, early psychosis patients receiving LAIs experienced a greater decrease in hospitalizations after introducing the LAI treatment than those treated solely with oral medication. These findings support using LAIs as a viable strategy for preventing rehospitalization and improving the overall course of treatment for individuals with early psychosis.
Introduction
Psychosis is a severe condition associated with high personal and familial burden,1,2 with an incidence of a first-time episode of psychosis of approximately 50 in 100,000 people, while schizophrenia is globally about 15 in 100,000 people. 3 The peak age of onset is around 20.5 years (median = 25), with a trend toward younger ages for males (median = 1 year earlier). 4 Earlier onset correlates with poorer outcomes,5,6 although early intervention correlates with better results 7 and preventive approaches are available.8–10 Effective management of schizophrenia requires early intervention and continuous long-term treatment to reduce symptoms, maintain function, improve quality of life, 11 and prevent relapses.12–14 After a first episode of psychosis, without pharmacological treatment, 67.4% to around 80% of patients will relapse in the following 5 years.15–17 This may be attributed to antipsychotic medication discontinuation 18 or poor adherence19,20 and relates to a worse long-term course of the psychotic disorder. 21
Long-acting injectable (LAI) antipsychotic treatments have been available since 1966, and LAI presentations of atypical antipsychotics were developed after 2000. 22 Certain advantages of LAI antipsychotics over oral presentations have been pointed out. Specifically, it has been stated that LAIs maintain more stable plasma concentrations than oral formulations, which could minimize side effects and prevent loss of efficacy.23,24 In addition, LAIs have been associated with reducing relapses by guaranteeing treatment adherence.25,26 The use of LAIs demonstrated, in some studies, a significant reduction in the incidence rate of hospitalizations in early psychosis patients27–31 and is associated with lower healthcare costs. 32
Different clinical guidelines recommend using LAI antipsychotic treatment in patients with poor adherence33–38 with heterogeneous use across countries. 39 Nevertheless, evidence regarding the impact of LAI use on the illness is contradictory. Some meta-analyses of randomized controlled trials (RCTs) report a lack of differences in efficacy between LAI versus oral presentation of antipsychotics,40–45 whereas others had suggested the superiority of LAIs. 46 On the other hand, some meta-analyses of cohort studies, including mirror studies, support the superiority of LAIs in preventing hospitalizations.42,47
This study proposes to provide more information on LAI antipsychotic treatments in a large cohort of young patients in the early stages of psychosis, representing our region, over an extended follow-up period. It involves incorporating data from everyday clinical practice into research, offering a matter-of-fact perspective tailored to the needs of our patients. So, we aimed to investigate the effect of LAI antipsychotic treatment on the incidence of hospitalizations in the real world throughout the illness by comparing it to oral antipsychotics in a large sample of early psychosis patients. We hypothesized that LAI treatments would lower hospitalization rates than oral atipsychotics (AP) during follow-up in early psychosis patients.
Methods
We considered the STROBE statement for the realization of this study (STrengthening the Reporting of OBservational studies in Epidemiology) 48 for observational studies (https://strobe-statement.org/index.php?id=strobe-home) (Supplemental Material).
Study setting
This study was conducted as part of the Lehenak program, a clinical community initiative of the Public Health Service of the Basque Country in Northern Spain. Launched in September 2011, the program is a specific service that offers treatment for the early phases of psychosis. Its population comprises roughly 1 million individuals, representing a vast majority of Biscay province, and hence is considered epidemiologically representative. This study was designed as a longitudinal observational study conducted within a naturalistic clinical setting in two different cohorts of early psychosis patients, one cohort with patients who took only oral antipsychotics and the other with patients on LAI treatment during the follow-up.
Sample
We used an electronic health register (EHR) to retrospectively identify individuals who had attended the service. Since 2011, the Basque Country Health System has implemented an EHR known as Osabide Global, which automatically captures health data, including sociodemographic variables. This study enrolled all patients who met the diagnosis criteria (Diagnostic and Statistical Manual of Mental Disorders-5) 49 for a psychotic disorder (including brief psychosis, schizophrenia, non-specified psychosis, schizoaffective disorder, schizotypal disorder, and affective psychoses, as shown in Table 1) with less than 5 years from the first psychotic symptoms 50 and attended the program from its inception (September 2011) until September 2020. From 1213 patients originally derived to the program within this period, 201 were not included because diagnostic confirmation was still pending at the time of the article preparation. Another group of 117 patients received non-psychosis diagnostic and were consequently excluded.
Sociodemographic and clinical characteristics of the sample.

Number of hospitalizations per person before the mirror period (severity proxy). Includes recorded hospitalizations before the date established for mirror beginning. The statistic employed is F because sex, age, and diagnostic have been covaried.
Days elapsed from the first hospitalization to LAI implementation.
Days elapsed on LAI treatment.
Total number of hospitalizations per person along the whole clinical follow-up.
LAI, long-acting injectable; SD, standard deviation.
The oral cohort comprised 667 patients who had never received LAI treatment, whereas the LAI cohort included 228 patients who received LAI antipsychotics during the follow-up. Demographic and clinical characteristics of the sample are detailed in Table 1.
Variables
The main outcome for all cases in this study was the number of hospitalizations documented in the electronic records of public health services. It is important to note that longer follow-up periods are associated with more hospitalization events. To address this potential bias, we divided the illness course of each patient into distinct periods based on the implementation of LAI treatment. We then compared the number of psychiatric hospitalizations during each of these periods to assess any differences.
(a) LAI cohort: A mirror period for each patient before the implementation of LAI treatment, which was equal in length to the LAI treatment period, was calculated (Figure 1). The number of hospitalizations that occurred during each period was then studied. T1 represents the period elapsed from the date of the first psychiatric record to the date that represents the beginning of the mirror period. In T1, all patients received oral antipsychotics. The T1 period was used as a proxy to estimate the initial severity of the illness to covariate, if necessary, in ulterior analyses. T2 represented the mirror period. T3 represented the LAI treatment period and was calculated from the LAI implementation to the date of LAI discontinuation. Finally, T4 represented the period defined from the date of LAI discontinuation to the closing of the database. In all cases, discontinuation of LAI involved the return to oral treatment. In all, 35 patients did not have T4 as they were still on LAI treatment at the time of database closing (September 2020), and their data were not included in the analysis of the effect of the LAI discontinuation.
In addition, a secondary analysis was conducted on a subset of patients (N = 158) who had sufficient follow-up time (defined as a time equal or greater in duration to T3) after discontinuing LAI treatment to enable the calculation of a post-LAI mirror period (Figure 2).
(b) Oral cohort: Since patients who receive LAI treatment may not be representative of early psychosis patients, a cohort composed of patients who never used LAI antipsychotics was studied. The course of the oral cohort was divided into the same periods as the LAI cohort. To create simulated LAI implementation and discontinuation dates for each patient in the oral cohort, the first step was to assign these participants a time beginning from the date of the patient’s first psychiatric record. The duration of this period was randomized for each patient but had the same mean and standard deviation (SD) as the LAI cohort’s T1 + T2. Microsoft Excel software was used to assign random periods for individual patients while maintaining the given mean and SD for the whole cohort, which allowed for assigning a simulated LAI implementation date for each patient. The same procedure was used to allocate a simulated LAI discontinuation date, with the same mean and SD as T3 in the LAI cohort. Once the LAI implementation and discontinuation dates were defined, mirror periods were established as in the LAI cohort. A T4Bis mirror period was also studied after simulated LAI discontinuation for long follow-up in those patients where data allowed it.
(c) Subgroup analyses: The study was repeated only considering patients with schizophrenia diagnosis since schizophrenia is the most common diagnosis among those receiving LAI treatment.
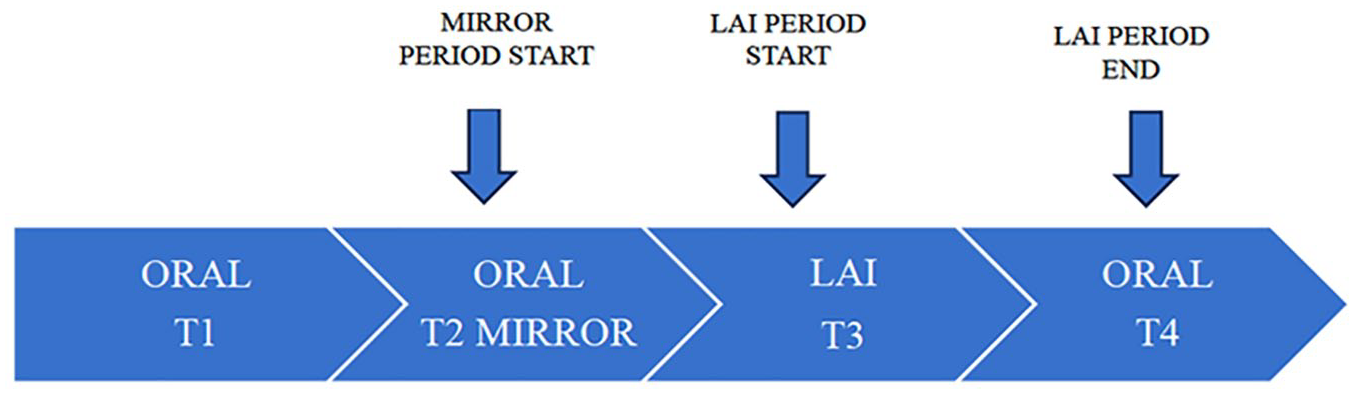
Study periods.

Study periods on a subset of patients.
Statistical analysis
Sociodemographic data were examined using independent sample Student’s t (quantitative variables) and χ2 (qualitative variables). Repeated series ANCOVA (ANCOVA-r) was used to study the number of hospitalizations in the different periods. The first analysis included the two cohorts between-group factor and three moments (T2, T3, and T4) as within-group factor (time). We used T1 as a covariate to represent the initial severity of illness, which was determined by the number of previous hospitalizations. Other confounding factors, such as age, sex, and diagnosis, were also considered. A repeated series of ANOVA-r analyses were conducted on the LAI cohort of 158 patients, using T1, T2, T3, T3Bis, and T4Bis periods as the within-group factor. All analyses were repeated for the schizophrenia subsample. We considered significant statistical results when p < 0.05. Version 25 of the SPSS software 5 (IBM, Armonk, NY, USA) was used to perform the analyses. 51
Results
Baseline descriptive variables
Table 1 shows the clinical and sociodemographic characteristics of the sample. In total, 667 participants were included in the oral cohort and 228 in the LAIS cohort. Patients in the LAI cohort were younger (30.94 versus 34.14), more frequently men (71.49% versus 56.82%), and had a higher rate of diagnoses of schizophrenia (57.01% versus 28%) than patients in the oral cohort. A total of 196 people received clozapine at some point: 66 in the oral group (9.89%) and 39 in the LAI group (17.10%) (χ2 = 53; p = 0.003).
In the oral cohort, 653 patients (97.90%) were on second-generation APs (the most frequently prescribed were olanzapine 36.1% and aripiprazole 15.3%) and 14 with first-generation AP. In the LAI cohort, 95 patients (41.67%) were with one monthly long-acting aripiprazole and 133 (58.33%) with one monthly long-acting paliperidone.
Hospitalization rates
The number of psychiatric hospitalizations in T1 was significantly higher in the LAI cohort than in the oral cohort (2.50 ± 2.61 versus 1.19 ± 1.69; p < 0.001). Table 2 and Figure 3 show the results of repeated series ANCOVA-r over the number of hospitalizations in every period in both cohorts. The between-group comparison showed that, during the T2 period, the oral cohort had significantly fewer hospitalizations than the LAI cohort. However, this difference vanished during the T3 period following the implementation of LAI, only to reappear during T4 after LAI was ceased (Figure 3).
Number of hospitalizations.
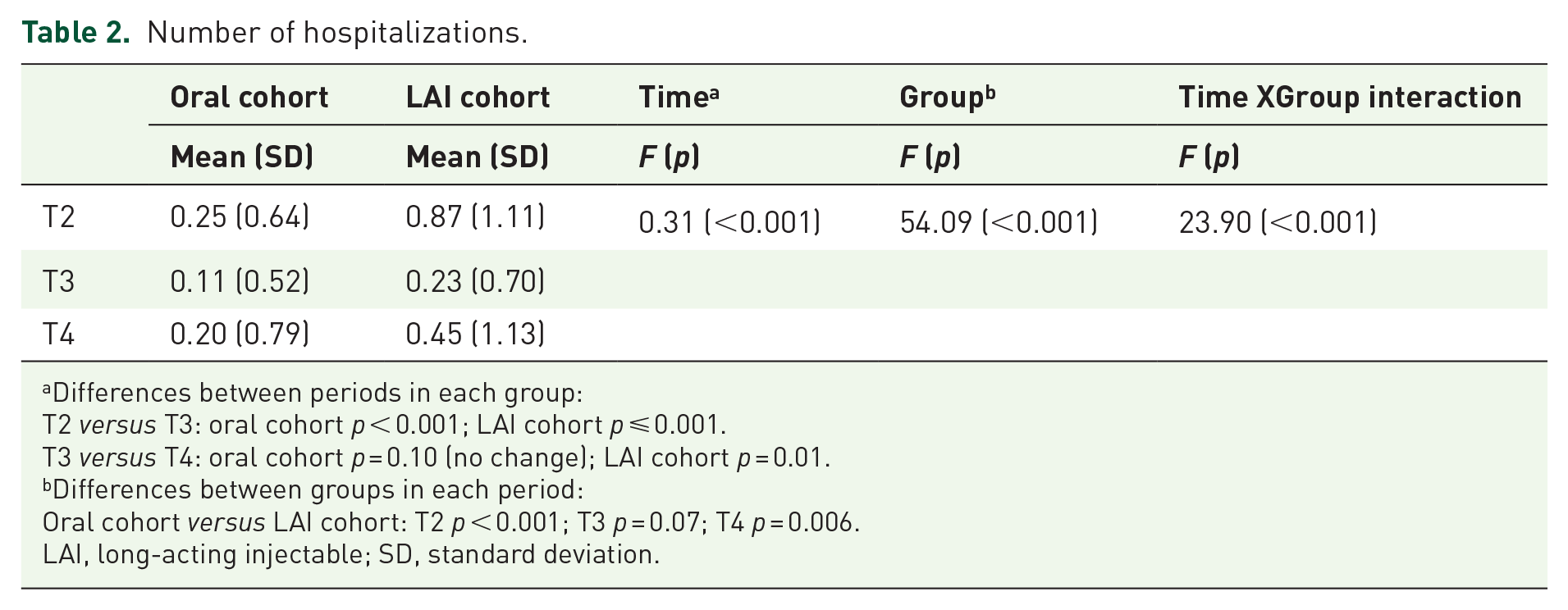
Differences between periods in each group:
T2 versus T3: oral cohort p < 0.001; LAI cohort p ⩽ 0.001.
T3 versus T4: oral cohort p = 0.10 (no change); LAI cohort p = 0.01.
Differences between groups in each period:
Oral cohort versus LAI cohort: T2 p < 0.001; T3 p = 0.07; T4 p = 0.006.
LAI, long-acting injectable; SD, standard deviation.
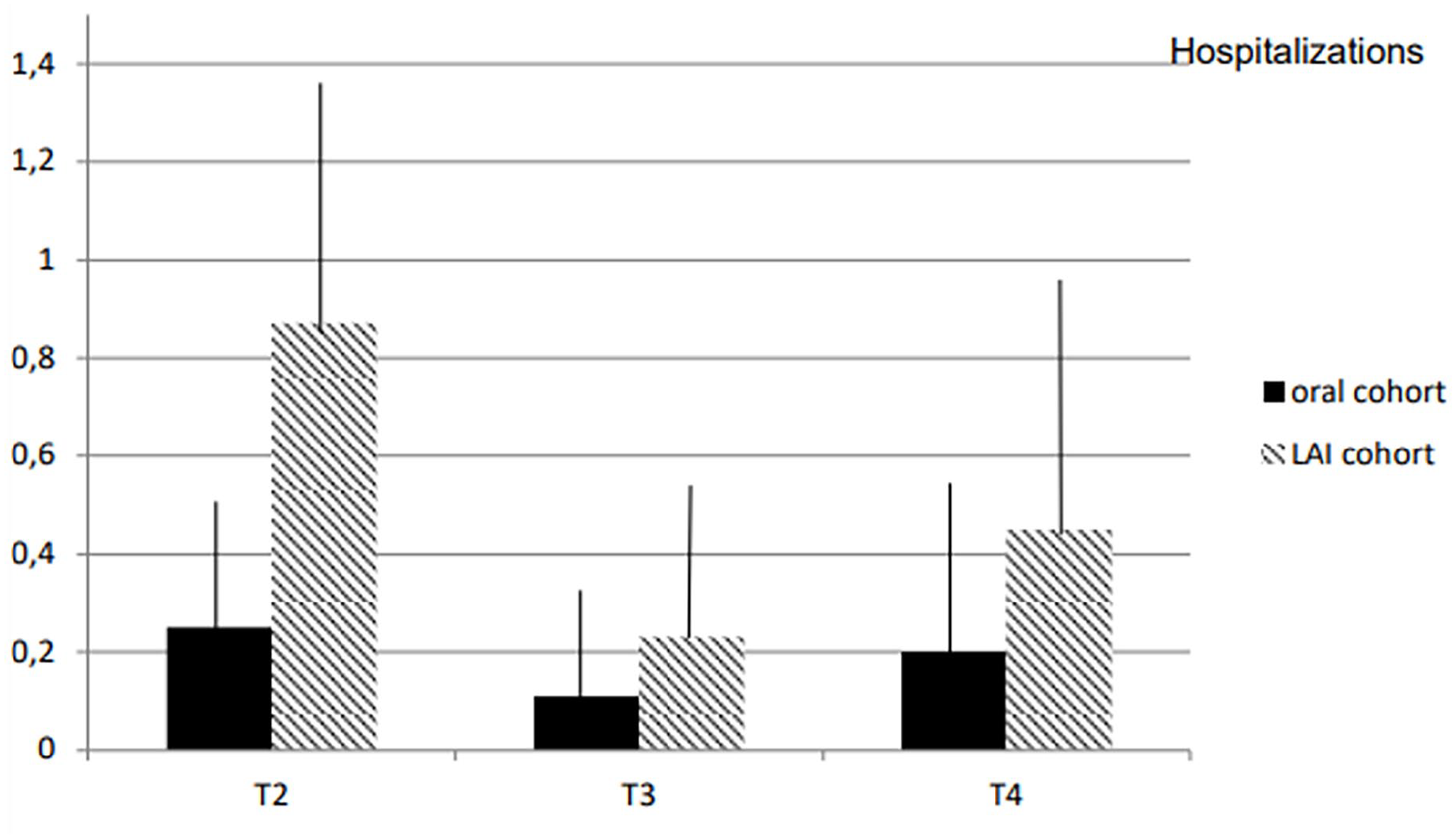
Number of hospitalizations.
Complementary results of the ANOVA-r analysis conducted on the 158 patients from the LAI cohort who had sufficient observation time to calculate a post-LAI mirror period demonstrated consistent outcomes. The mean hospitalization in T1 for the LAI cohort was 0.90 (SD = 1.36) and 0.66 (SD = 0.86) in T2. Then, the number of hospitalizations decreased abruptly at T3 (mean = 0.23, SD = 0.67) following the implementation of LAI. The reduced number of hospitalizations persisted during the post-LAI mirror period (T3Bis, mean = 0.16, SD = 0.54) after LAI discontinuation. However, during the last stage (T4Bis, mean = 0.44, SD = 1.16), there was a slight upward trend in the number of hospitalizations, which was not statistically significant [T1 = T2 (p = 0.73); T2 > T3 (p ⩽ 0.001); T3 = T3Bis (p = 1); T3Bis = T4Bis (p = 0.07), F = 20.5; p < 0.001].
Sensitivity analyses in the schizophrenia subsample
The sociodemographic characteristics of the schizophrenia subsample are displayed in Table 3. In total, 190 patients had a diagnosis of schizophrenia in the oral cohort versus 130 in the LAI cohort. There were more male schizophrenia patients in the LAI cohort (79.23% versus 67.37%), and they were younger than in the oral cohort. Results of ANCOVA-r showed that the mean number of hospitalizations was 0.86 (SD = 1.37) in T1, 0.87 (SD = 1.14) in T2 (p = 0.1), 0.25 (SD = 0.71) in T3 (p < 0.0001), 0.13 (SD = 0.40) in T3Bis (p = 0.66), and 0.38 (SD = 1.16) in T4Bis (p = 0.22) (F = 18.2; p < 0.001).
Sociodemographic characteristics of a subsample of patients with schizophrenia.

Number of hospitalizations before the mirror period (severity proxy). Includes recorded hospitalizations before the date established for mirror beginning. The statistic employed is F because sex has been covaried.
Days elapsed from the first hospitalization to LAI implementation.
Days elapsed on LAI treatment.
LAI, long-acting injectable; SD, standard deviation.
Complementary results of ANOVA-r performed over the 152 patients of the LAI cohort that had enough observation time to calculate a post-LAI mirror period showed consistent results (Table 4). Results replicate accurately those already seen in the whole sample: the number of hospitalizations abruptly decreases after LAI implementation; the decrease is maintained in the post-LAI mirror and starts to increase (without reaching statistical significance) afterward.
A number of hospitalizations of a subsample of patients with schizophrenia.

F = 20.5 (p < 0.001); T1 = T2 (p = 0.73); T2 > T3 (p ⩽ 0.001); T3 = T3Bis (p = 1); T3Bis = T4Bis (p = 0.07).
SD, standard deviation.
Discussion
The study examined two cohorts of early psychosis patients: one treated exclusively with oral antipsychotics and the other receiving LAI treatment at some point during their course of treatment. Both cohorts experienced decreased hospitalizations from baseline to follow-up, but the LAI cohort experienced a more significant reduction in hospital admissions than the oral cohort. It is noteworthy that the LAI cohort had more hospitalizations initially, and the greater decrease meant that the LAI cohort reached a level comparable to the oral cohort. However, after the discontinuation of LAI, the hospitalization rate increased again for this group. The higher number of hospitalizations before the implementation of the LAI treatment may imply a higher severity of these patients. 52 Although cohort studies do not allow for random assignment of treatments, they provide a more accurate picture of the patient population receiving LAI treatment in clinical practice. 53 To address the limitation of bidirectional mirror designs in cohort studies, a subsample of the LAI cohort was examined, focusing on two mirror periods: prior and post-LAI treatment. Consistently, hospitalizations decreased during the LAI treatment period compared to the prior mirror period but increased again in the post-LAI treatment mirror. In our study, the analysis in the subsample of schizophrenia patients yielded the same results.
Meta-analysis of cohorts 54 and mirror studies47,55 reported the superiority of LAIs over oral treatments for hospitalization rates. However, in our study, hospitalizations in the LAI cohort decreased significantly only once LAI was implemented. That is, the only period when the number of hospitalizations was comparable between cohorts was the LAI treatment period. In all other periods, hospitalizations were significantly greater in the LAI cohort than in the oral cohort. The higher severity of the LAI cohort could explain this fact. There was a more frequent diagnosis of schizophrenia in the LAI cohort, more males and patients were younger than in the oral cohort. Other studies described that the LAI option treatment is still used more in patients with an expected worse prognosis. 52 However, there are encouraging findings with the use of LAI treatments, Garcia-Carmona et al. 56 described the reduced necessity of daily benzodiazepines, and fewer visits to the emergency department and hospitalizations in patients with LAIs over oral antipsychotics. On the other hand, some meta-analyses of RCT studies42,57,58 reported similar hospitalization rates between LAI and oral-treated patients.
This disparity may be because RCT design may not be the best strategy to evaluate the efficacy of LAIs. Due to recruitment criteria, patients assigned to LAI treatment in RCTs may not be representative of those receiving this kind of treatment in real clinical practice 59 because they could be more adherent to treatment, and even the RCT could improve the adherence rate, masking the possible benefits of the LAI treatment. 58 Conversely, unlike real clinical practice, RCT studies guarantee adherence to oral treatment, which may affect results. 60
Limitations
This study has several limitations, one of the most significant being the naturalistic design. Nonetheless, naturalistic studies are a common approach for observing real clinical practice, 61 effectively minimizing biases in prescription patterns. These studies are conducted in real-world clinical settings, ensuring high clinical representativeness. Moreover, these studies include patients with comorbidities, and treatment decisions are made based on clinical requirements. 62 However, the absence of randomization likely contributes to a prescription indication bias, where patients with better insight are more likely to receive oral antipsychotics more frequently, while patients with poorer insight may refuse LAIs from the outset. Consequently, subgroups of patients categorized by their initial antipsychotic treatment may exhibit clinical characteristics or disease severity variations, making these groups less comparable. A reflection of this is that patients with LAI treatment presented with more hospitalizations at baseline than patients with oral APs. Similarly, the abrupt reduction of hospitalizations once LAI was implemented was likely due to greater efficacy in symptom reduction or better therapeutic adherence. Another limitation is that we did not consider other important factors for relapses and therapeutic adherence, for example, drug abuse. Besides, the change in the different APs in the follow-up should have been considered. Moreover, the registration of the data did not allow to specify the cause of the discontinuation of the medication. Due to the period of time included in the study, only one monthly LAI was included; hence, new formulations with longer duration (e.g. three-monthly) may change these results. A recent study described that three-monthly formulations presented lower mean rates of psychiatric hospitalization and emergency room visits and showed higher retention treatment rates at 18 months than one monthly formulation (including aripiprazole and paliperidone). 63 Finally, the potential effect of wash-out after LAI discontinuation (given the differences in time to reach a steady state among these patients) could not be controlled. However, its potential impact was minimized by the use of a long T4Bis mirror period (i.e. a long follow-up after LAI ceases) for most patients.
We introduce an innovative methodology for examining the correlation between utilizing LAIs and relapse occurrences within a naturalistic setting. This approach mitigates the potential bias stemming from the mere passage of time, which might otherwise impact the frequency of hospitalizations. Besides, this is a real-world study with a large sample of early psychosis patients attending early intervention services, which may make the conclusions valuable.
Our data show reduced hospitalizations after implementing LAI treatment in early psychosis patients. Considering all this, it could be hypothesized that LAI’s superiority may not involve a greater clinical efficacy in symptom reduction but in adherence warranty. To clarify this aspect, further studies should address this question. Consistently, Weiser et al. 64 found that the use of LAI was associated with a lower risk of discontinuation and concluded that it might be due to more acceptability of this treatment.
Conclusion
Our study is naturalistic, which does not provide the level of control of RCT and, therefore, is more representative of real clinical practice. However, unlike previous evidence with cohort studies and RCTs, we do not find a global superiority of LAIs over oral antipsychotics in general terms. This could be explained partially by the psychiatrists’ ‘selection bias’ in using LAI; more severe patients are candidates for using LAIs, and patients with expected better prognoses are treated with the oral AP options. Rather, as long as they are present, LAI seems to provide a ‘normalization’ of the clinical course of the most severe patients. Therefore, LAI treatment may be superior to oral treatment in patients with more severe presentations of the illness. LAIs can also be considered an effective treatment strategy for improving adherence and a tool for detecting early non-adherence in the follow-up.65,66
Supplemental Material
sj-docx-1-tpp-10.1177_20451253241243273 – Supplemental material for Effect of long-acting antipsychotic treatment on psychiatric hospitalization rate in early psychosis patients: a naturalistic study
Supplemental material, sj-docx-1-tpp-10.1177_20451253241243273 for Effect of long-acting antipsychotic treatment on psychiatric hospitalization rate in early psychosis patients: a naturalistic study by Raúl Sancho-Echeverria, Claudia Aymerich, José Manuel Rodríguez-Sánchez, Patxi Gil, Borja Pedruzo, Miguel Ángel González-Torres, Paolo Fusar-Poli, Celso Arango and Ana Catalan in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.