
Abstract
Background:
Cognitive models of post-traumatic stress disorder (PTSD) highlighted the effect of maladaptive cognitive processing in the development and maintenance of PTSD. PTSD is related to attentional bias (AB) toward threatening stimuli and greater attentional bias variability (ABV). Attentional bias modification (ABM) and attention control training (ACT) have demonstrated the effect of improving PTSD, but the results of randomized controlled trials (RCTs) are controversial.
Objectives:
The current study aimed to evaluate the extent of evidence supporting the efficacy of ABM in the treatment of PTSD.
Design:
Systematic review and meta-analysis.
Methods:
We searched PUBMED, PsycINFO, EMBASE, ClinicalTrials.gov, and the Cochrane Central Register of Controlled Trials for articles published between 1980 and 2022. RCTs of ABM for adult participants with PTSD symptoms were identified. The primary outcome was changes in PTSD severity, and the second outcome was changes in AB and ABV. Trial quality was assessed using the Cochrane Risk of Bias Tool. Publication bias was assessed using the Doi plot and Luis Furuya-Kanamori (
Results:
Eight RCTs comparing the effect of ABM to ACT were included in the review, and six studies were meta-analyzed. Meta-analysis favored ACT in improving PTSD symptoms and ABV, and the effect size was large. ABM and ACT demonstrated similar effects in improving AB.
Conclusion:
ACT should not only be seen as a control training condition but also has therapeutic values. However, since the current meta-analysis only included a limited number of studies, further research was still needed to examine the clinical value of ACT in PTSD treatment.
Plain language summary
We summarized and analyzed studies on attentional bias modification (ABM) and attention control training (ACT) in PTSD. Our findings indicated that ACT was a more effective treatment condition. This study highlights the therapeutic value of ACT.
Introduction
Post-traumatic stress disorder (PTSD) symptoms are characterized by maladaptive responses to traumatic events, including re-experience, avoidance, hyperarousal, and negative alterations in cognition and mood. 1 PTSD seriously interferes with the normal work and life of individuals and increases an individual’s suicide risk. 2 The lifetime prevalence estimate for PTSD using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) criteria is 6.8% for U.S. adults. 1
In the past 30 years, several information processing theories have been proposed to elucidate the development and maintenance of PTSD, and these theories highlighted dysfunctions in cognitive processes contributing to PTSD. In support of these cognitive models, accumulating evidence has shown that patients diagnosed with PTSD process information in biased ways during the attention process stage. 3 For example, studies have shown that participants diagnosed with PTSD respond more rapidly when they were faced with threatening stimuli compared to non-threatening stimuli, showing attentional toward threats [i.e. attentional bias (AB)]. 4 But other researchers have also found that participants with more severe PTSD symptoms were more likely to demonstrate attentional avoidance of threats and illustrated delayed responses to threats. 5
The traditional way of evaluating AB in PTSD was to compare the average reaction time (RT) of threatening stimuli to non-threatening ones, but as Zvielli et al. pointed out, this traditional view was based on the hypothesis that AB in PTSD was expressed stably or statically and that each subject might either express AB toward or away from threats. 6 However, this hypothesis has not been tested.7,8 Instead, they raised the concept of attentional bias variability (ABV), which provided a dynamic approach to the understanding of AB in PTSD. ABV illustrates the inconsistent attentional strategy that may reflect and/or lead to incomplete processing of trauma, as individuals oscillate between different attentional patterns (i.e. attentional toward threats and attentional away from threats).9,10 Studies have illustrated that ABV showed good reliability and validity in participants diagnosed with PTSD. 11 Researchers have also found that participants with PTSD exhibited significantly greater ABV than those without PTSD. 8
Fortunately, the biased attentional processing in PTSD could be modified. There was evidence that both AB and ABV could be modified with attentional bias modification (ABM).12,13 In ABM, negative AB was fixed by guiding subjects to unconsciously increase attention to non-threatening stimuli. In randomized controlled trials (RCTs), ABM was generally compared with the attention control training (ACT) for efficacy. ACT did not direct subjects’ attention to either threatening stimuli or non-threatening stimuli and allowed the subject to maintain his or her original attentional characteristics. There are already several meta-analyses that compared the effect of ABM and ACT and revealed the efficacy of ABM in anxiety and depression. These studies have contributed to the development and spread of ABM as a novel cognitive intervention method. 14 For example, Heeren et al. 15 found that ABM produced a small but significant reduction in social anxiety disorder (SAD) symptoms and AB. In another study of depression, researchers found that compared with ACT training, ABM had a greater effect on the improvement of depressive symptoms. 16 However, in previous meta-analyses, the efficacy of ABM on PTSD has not been discussed. Despite ACT traditionally being viewed as a control condition for ABM, there was evidence suggesting that ACT might have a more favorable impact on the improvement of PTSD compared to ABM. 17 These surprising findings needed to be summarized by meta-analysis. Also, in previous meta-analyses, the outcome of ABV was rarely mentioned. In the only meta-analysis and systematic review on ABV, researchers found that both ABM and control training showed similar levels of ABV change during the intervention. 18 However, this meta-analysis included not only PTSD but also other psychiatric disorders, 18 which might have an impact on the results. Taken together, the current meta-analysis aimed to compare the efficacy of ABM to ACT on the improvement of PTSD, AB as well as ABV.
Methods
Study selection
This meta-analysis was carried out following the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement (see Supplemental material for PRISMA statement of the present study). 19 This study was registered at the International Prospective Register of systematic reviews (PROSPERO; https://www.crd.york.ac.uk/PROSPERO/), and the registration number was CRD42021247012. The study was approved by the ethics review committee of Naval Medical University. The protocol of the current study was not prepared.
We conducted a comprehensive literature search strategy for RCTs of ABM in PTSD. The following databases were searched: PUBMED, PsycINFO, EMBASE, ClinicalTrials.gov, and the Cochrane Central Register of Controlled Trials. English-language articles published in peer-reviewed journals between 1980 (the year PTSD was first included in the DSM) and December 2023 were considered for inclusion. See Figure 1 for the detailed strategies.

Search strategy for the current study.
The flow of information from identification to inclusion of studies was summarized in the PRISMA diagram depicted in Figure 2. From the initial 205 emerging publications, duplicates were removed, and the abstracts from the remaining 104 publications were screened. Then we screened the title, abstract, and full text using the following criteria:
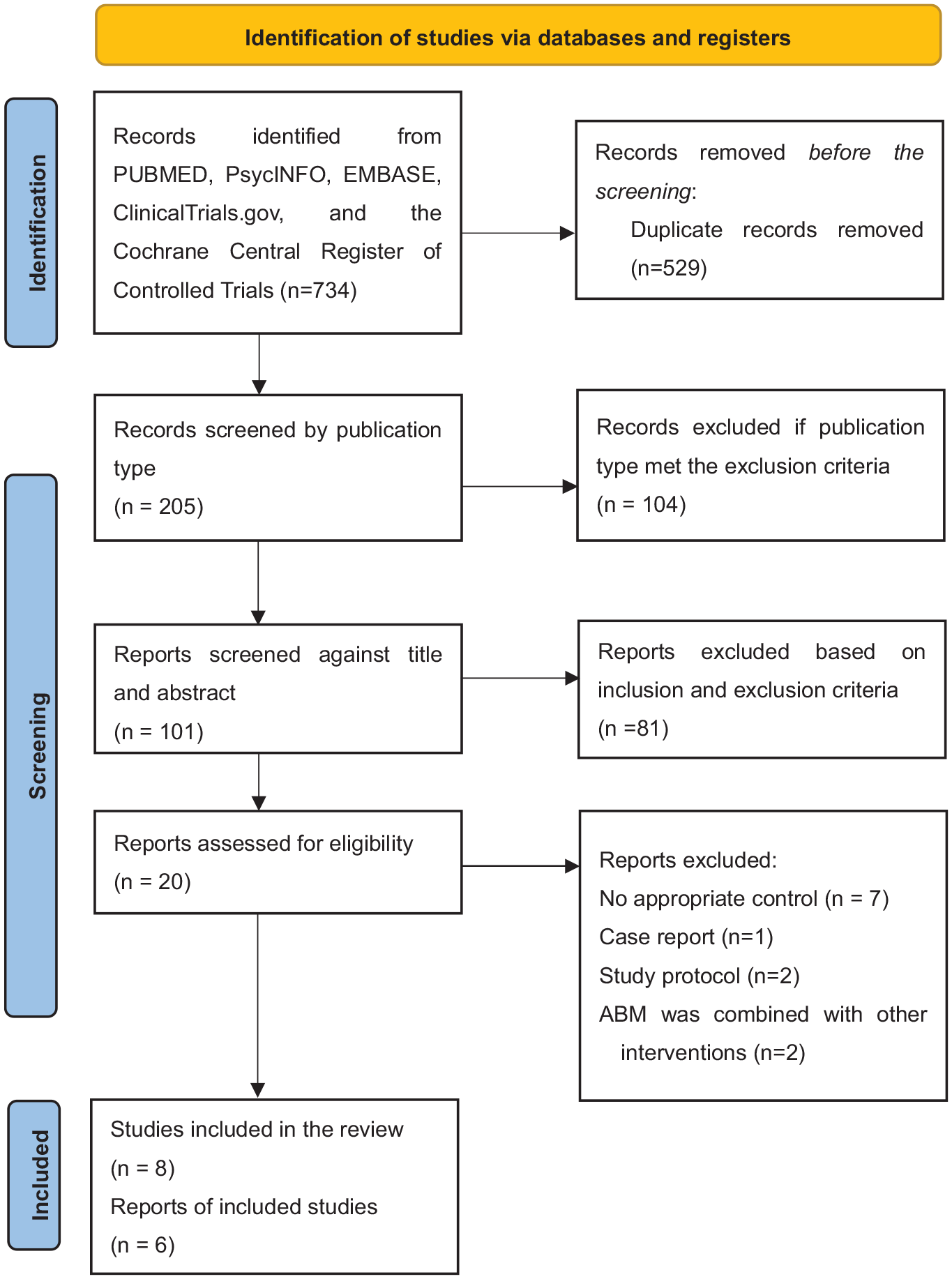
PRISMA flow diagram.
Inclusion criteria: (a) random assignment, (b) using ACT as the control condition, (c) subjects aged ⩾18, (d) standardized measures of symptoms, (e) one or more sessions of ABM during treatment, and (f) published in scientific journals in English.
Exclude criteria: (a) the study was not designed specifically to manipulate AB; (b) participants were not randomly allocated to training conditions; (c) control conditions were not used; (d) the studies designed ABM in combination with other treatment as intervention; (e) commentary, editorial, case report, study protocol, or review; and (f) articles that could not be retrieved in full-text.
The total search was conducted by two authors (C.H. and F.Z.) independently using the above search strategy. They also screened the title and the abstract independently to identify studies that met the above eligibility criteria (with 100% concordance). During the full-text stage, two authors had a disagreement about an article, which was eventually resolved by consulting a third author (W.L.). Finally, seven relevant articles (eight studies in total) were identified by reviewing their abstracts and full texts. They were published between 2013 and 2022. Two studies did not offer complete pre- or post-training data and were not included in the meta-analysis; however, for better review of current research progress, study design and results of the two studies were included in Table 1.
Intervention study of attentional bias modification training for PTSD.

These studies were not included in the meta-analysis for incomplete data.
AB, attentional bias; ABM, attentional bias modification; ABV, attentional bias variability; ACT, attention control training; CAPS, the clinician-administered PTSD scale; EST, the emotional Stroop task; PCL, the PTSD Checklist; PTSD, post-traumatic stress disorder; SRIP, the Self-Rating Inventory for Post-traumatic Stress Disorder.
Data extraction
Data on the following variables were collected: author, year of publication, characteristics of participants (age, gender, trauma types), treatment conditions, type of trauma, number of sessions, training materials, number of participants, and primary outcome measures (see Table 1). Among the k = 8 ABM versus ACT studies, k = 6 studies provided complete data and were analyzed. Follow-up data were not included, because only one study reported follow-up data. 23 Dependent variables were classified as PTSD, AB, and ABV. Each study’s characteristics were extracted by one author (F.Z.) and checked independently by a second author (C.H.).
Assessment of outcome variables
The current meta-analysis mainly focused on the efficacy of ABM training on three outcome variables: PTSD, AB, and ABV. PTSD severity was generally assessed by self-report scales like the clinician-administered PTSD scale (CAPS), the Self-Rating Inventory for Post-traumatic Stress Disorder (SRIP), the PTSD Checklist (PCL), etc. If PTSD severity was measured by more than one instrument, the primary outcome index was employed. Across studies, AB and ABV were both typically assessed through the dot-probe paradigm. In this paradigm, a pair of stimuli with one threatening stimulus (e.g. an angry face) and one neutral stimulus (e.g. a neutral face) showed first, and after they disappeared, a probe would occur in the same location as either the threatening stimulus (threat trials) or the neutral stimulus (neutral trials). AB was calculated for each participant as the differences between the mean RT on threat-incongruent trials (i.e. the probe appeared in the location previously occupied by the neutral stimulus) and mean RT on threat-congruent trials (i.e. the probe appeared in the location previously occupied by the threatening stimulus). Thus, the positive value of AB indicated an AB toward threats. In the current included studies, ABV was generally calculated following Naim et al.’s steps. 24 First, mean RTs for 10 successive neutral trial blocks and 10 successive threat trial blocks were calculated. Then, a series of bias indexes were calculated by subtracting the first threat block average from the first neutral block average, the second threat block average from the second neutral block, etc. After that, the standard deviation of these successive bias scores was then calculated and divided by the participant’s mean overall RT.
Quality assessment
To determine the quality of reporting and the presence of methodological bias, a systematic quality assessment was performed according to the seven criteria of the ‘Risk of Bias’ assessment tool developed by the Cochrane Collaboration. Two reviewers (C.H. and F.Z.) independently assessed the articles and any disagreements were resolved through discussion. Based on the seven criteria in Cochrane Collaboration’s tool: random sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective reporting and other bias; the risk of each study was assessed as ‘low’, ‘high’, or ‘unclear’.
Meta-analysis
Meta-analyses were conducted with Review Manager 5.4 and MetaXL. 25 Due to the expected heterogeneity of these studies, the random effect models were used with standardized mean differences applied to measure the effect with 95% confidence intervals (95% CIs).
Each result of the meta-analyses was illustrated by one forest plot. For each comparison between ABM and ACT training, effect sizes (ESs) were calculated by subtracting (at post-test) the mean value of the ABM group from the mean value of the control group and dividing the result by the pooled standard deviations of the two groups.
26
We adjusted the ESs with Hedges’s g developed by Hedges and Olkin due to small sample sizes.
27
Hedges’ g measures ESs in the following way: g ⩽ 0.20 indicated a small ES, g = 0.2–0.5 indicated a moderate ES, and g ⩾ 0.70 indicated a large ES. The homogeneity of ES was assessed with the I2 index. I2 indicates the percentage of observed heterogeneity and is not sensitive to the number of studies.
28
A value of 0% indicates no heterogeneity and larger values indicate increasing heterogeneity: 25% as low, 50% as moderate, and 75% as high heterogeneity.
29
Publication bias was assessed using the Doi plot and Luis Furuya-Kanamori (
Result
Study characteristics
A total of 329 participants were included in our analyses (ABM, N = 163, ACT, N = 166). Nearly all participants were clinic patients (N = 310, 94.2%). Among the included studies, k = 5 studies reported self-rated PTSD severity, k = 6 studies reported AB and k = 4 reported ABV scores.
Quality of the evidence
The overall quality of the articles varied (see Figure 3). k = 3 studies explicitly reported an adequate random sequence generation.13,23 Beyond two criteria related to selection bias, Badura-Brack et al.’s study 17 and Alon et al.’s study 12 met other criteria. Buodo et al.’s study 20 did not exactly mention that the trial staff were adequately blind to allocation to condition and blinding of outcome assessment. In one study, outcome variables were assessed by the first author. 23

Risk of bias. (a) risk of bias for each study. (b) sum of bias scores.
Effect of ABM versus ACT on PTSD symptoms, AB, and ABV
Five out of the eight included studies illustrated that the ACT and ABM were equally effective in reducing PTSD symptoms.12,21–23 Two favored the efficacy of ACT,13,17 and none study supported that ABM could be a more effective therapeutic method for PTSD than ACT. Complete data were available for 5 studies and 310 participants. Meta-analyses showed that there was a significant difference in efficacy between ABM and ACT (g = 1.21, 95% CI = [0.05–2.38]), favoring the efficacy of ACT and the ES was large. Heterogeneity among all studies for post-treatment ESs was high (I2 = 95%). See Figure 4(a) for detailed results.
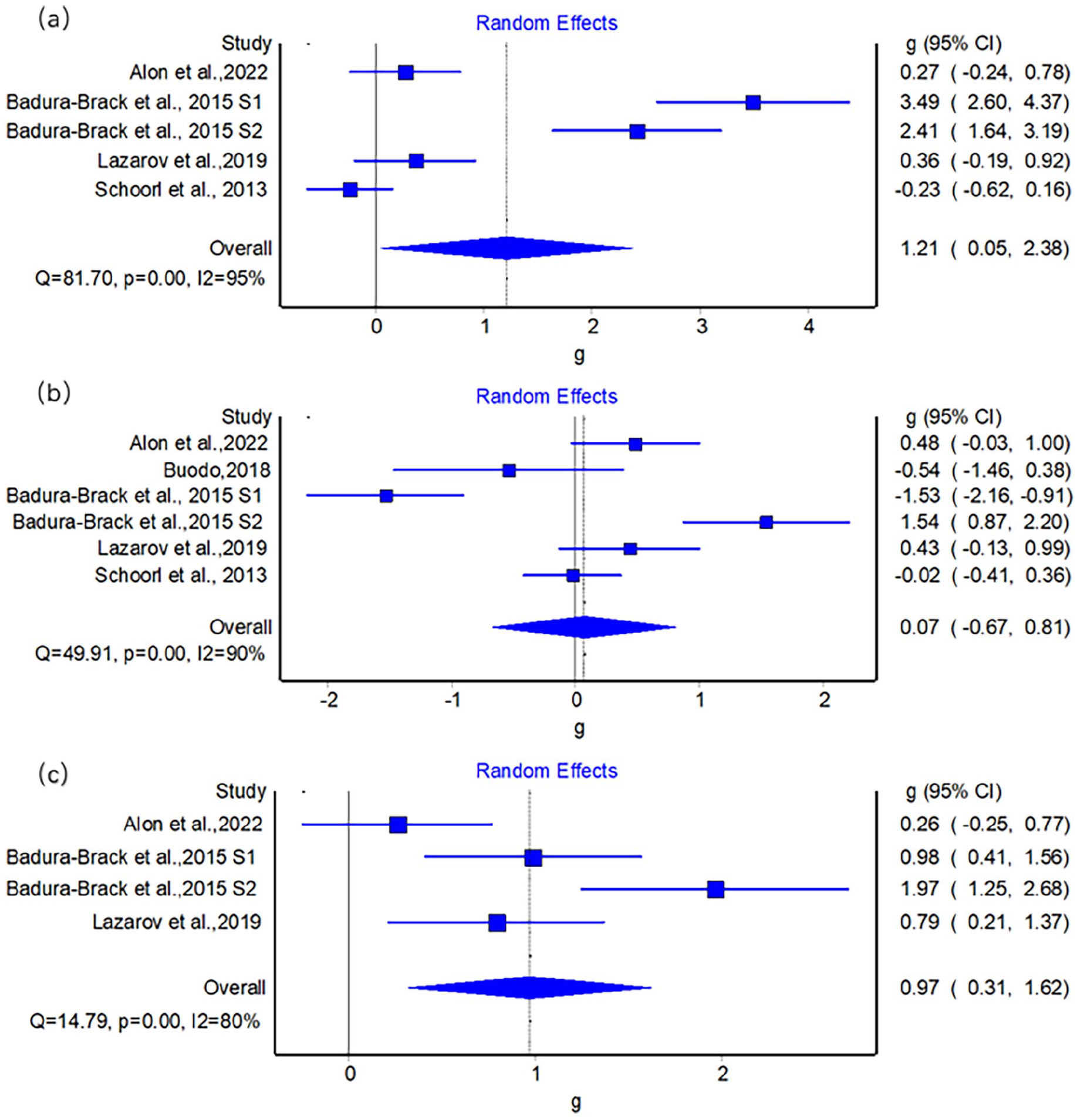
Forest plot of comparison between ABM and ACT on PTSD severity (a), AB (b) and ABV (c).
Schoorl et al., 23 Badura-Brack et al., 17 and Alon et al. 12 all showed that ABM had little effect in improving negative AB. But another three studies favored the effectiveness of ABM on reducing AB, and they showed that the effect of ABM surpassed that of ACT.13,20,22 Of noted, two of out the three studies favored the effect of ABM used non-clinical samples, and the three researches finding negative results all used clinical samples. The meta-analysis of the training effect on threat-related AB was calculated. k = 6 studies with 329 participants were included. Results showed no significant group difference between ABM and ACT (g = 0.07, 95% CI = [−0.67, 0.81]). Heterogeneity was high (I2 = 90%). See Figure 4(b) for detailed results.
Badura-Brack et al., 17 Lazarov et al., 13 Niles et al., 22 and Alon et al. 12 measured ABV in pre- and post-training tests, and Badura-Brack et al. 17 illustrated that only ACT could effectively improve ABV. The meta-analysis of training effect on threat-related ABV illustrated a significant between-group difference with a large ES, g = 0.97, 95% CI = [0.31–1.62]. Heterogeneity was high (I2 = 80%). See Figure 4(c) for detailed results.
Publication bias
The Doi plots for publication bias (see Figure 5) showed major asymmetry (LFK index = 3.08) in meta-analyses for reduction in PTSD severity and minor asymmetry in meta-analyses for AB (LFK index = −1.03) and ABV reductions (LFK index = 1.25; see Figure 5). The publication bias indicated that studies with positive (i.e. favoring ABM) or equal outcomes are lacking for PTSD reduction. However, due to the limited number of included studies, these results should be interpreted with caution.

Doi plots and Luis Furuya-Kanamori (
Possible moderators
For the reduction of PTSD, none of the included studies reported that the efficacy of ABM surpassed that of ACT. Although the studies varied in training types and training sessions, they all used clinical patients as research subjects. The only study on non-clinical subjects did not assess change in PTSD severity. 20 In both studies, Badura-Brack et al. found that only ACT but not the ABM group showed significant change in ABV using both dot-probe tasks with face and word, 17 but in another two studies that assessed ABV, researchers reported no group differences.12,13 In Badura-Brack et al.’s study, they studied male subjects who had been exposed to military trauma, whereas in Alon et al.’s and Lazarov et al.’s study, subjects included females who had experienced mixed trauma. For the change in AB, most of the included studies did not find that ABM or ACT training could change AB, but Buodo et al. 20 reported that only ABM could change AB significantly, whereas Khanna et al. reported opposed results. 21 There were no clear moderators for training on AB change.
Discussion
The current study identified that only 8 RCTs with a total of 329 participants met the inclusion criteria. These studies differed in sample characteristics, training sessions, and trauma types, and the results were highly variable. The current finding that ACT was more effective in improving PTSD, as well as ABV, might be due to its function of enhancing attentional control, which is the ability to willfully direct attention toward or away from specific stimuli. 31 ABV could reflect an individual’s inconsistent attention toward or away from threats 11 and was associated with attentional control. 32 Deficient-attention control was also linked with PTSD by diminishing patients’ ability to direct attention away from threatening stimuli, causing greater anxious arousal and maintaining the symptoms. 33 In ACT, probes appeared equally often after threatening and neutral stimuli. This required them to ignore irrelevant threat-related contingencies and focus on the task at hand. In this way, ACT training helped to normalize strong within-task fluctuations and enhance attentional control. 17 With improved attentional control abilities, clinical benefits would show. 34 In line with previous research that considered ACT a training condition rather than a control condition for ABM, 34 the current study highlighted the therapeutic potential of ACT in PTSD treatment.
Our meta-analyses found that ACT and ABM were similarly effective in improving AB. This result was interesting because ACT was originally been used as the control training of ABM in reducing AB. Previous meta-analysis of anxiety supported the efficacy of ABM for improving AB and anxiety symptoms in adults. 14 Differences between our study and previous studies may stem from the differences between PTSD and anxiety disorders. In PTSD, no specific direction of attention bias has been ascertained. Studies have supported both AB toward and away from threats, and there was even evidence of no AB in PTSD.4,5,35 This was also the case in the currently included studies: Buodo et al., 20 Lazarov et al., 13 and Khanna et al. 21 reported AB toward threats in the bassline assessment of AB, but Niles et al. 22 found no attentional bias, and in Badura-Brake et al.’s studies, three out of four groups even showed negative AB scores (i.e. attention away from threats) in pre-training tests. 17 There was evidence that only people who showed elevated AB toward threats at baseline were likely to benefit from ABM, 36 and lack of baseline AB might underlie the current negative result. Another underlying reason for the negative result might be that the number of included studies was small, and there was only one study using healthy adults as participants. Evidence has shown that studies conducted on healthy participants could boost the effect of cognitive bias modification, including ABM. 37 In accordance with this finding, the only research on healthy participants in the present meta-analysis was also the only one to support ABM for AB reduction. 20 Future studies could recruit traumatized individuals who fail to meet diagnostic criteria and explore the effect of ABM in samples with mild PTSD symptoms.
There were some discrepancies between our findings and results in Todd et al.’s meta-analyses. 18 Todd et al. reported that both ABV and PTSD symptoms reduced from pre- to post-intervention, but the group differences between active intervention and ACT were not significant. 18 In their meta-analysis of ABV, not only traumatized personnel were included, but they also included participants with depressive symptoms, anxious symptoms, and alcohol dependence. And in their meta-analysis of PTSD symptoms, they compared the efficacy of various intervention conditions (ABM, treatment as usual) to ACT, whereas the current study only focused on ABM and ACT. Of note, the number of included studies in both the present study and Todd et al.’s study was relatively small, and further work was still needed to explore the efficacy of ACT on reducing ABV and PTSD.
Our meta-analysis has several limitations. We only included published articles, and this might lead to some omissions (e.g. dissertations, unpublished manuscripts, etc.). Some data in the retrieved studies were still not available and might affected the results of meta-analyses. In the field of attention bias training, the majority of studies relied on self-report measures, which may lead to self-report bias. Future studies might benefit from recording physiological data and provide more robust data for the efficacy of training. Although we had tried our best to search articles, only a limited numbers of studies met eligibility criteria and were included in meta-analyses, rendering it impossible to compute meaningful subgroup analyses. The meta-analyses only considered post-training values and did not take into account baseline values. For all outcomes, I2 was large, indicating high levels of between-study heterogeneity. However, subgroup analysis was inappropriate due to the small number of studies included.
Conclusion
The current study compared the intervention effect of ABM and ACT. Results favored ACT in improving PTSD symptoms and AB variability and the ES was large. ABM and ACT demonstrated similar effects on improving AB. These results indicated the therapeutic value of ACT. However, since the current meta-analysis only included a limited number of studies, further research was still needed to examine the clinical value of ACT in PTSD treatment.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253241243260 – Supplemental material for Attentional bias modification and attention control training in PTSD: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tpp-10.1177_20451253241243260 for Attentional bias modification and attention control training in PTSD: a systematic review and meta-analysis by Fan Zhang, Chenwei Huang, Wenjie Yan, Hui Ouyang and Weizhi Liu in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.