
Abstract
The conceptualization and empirical knowledge base related to major depression has increased dramatically in recent years. We now have well-developed and validated models of depression from a range of theoretical perspectives. These models have significantly enhanced the development of effective treatments and preventative interventions. Although various prevention programs are available, Web-based protocols can enhance accessibility to evidence-based prevention programs. The current study involved a randomized controlled trial focused on the prevention and treatment of depression in high-risk first- and second-year undergraduate students. Three Internet-delivered preventative programs were compared: cognitive behavioral therapy (CBT; MoodGym), attentional bias modification, and an active attentional control condition. Participants (n = 350) completed symptom measurement pre- and post-intervention (6 weeks) and again at a 4-month follow-up, when they were also administered a structured diagnostic interview. Participants in the CBT condition showed more dramatic and continuous depressive symptom improvement between baseline and follow-up than did participants in the other two conditions. In addition, significantly fewer individuals in CBT condition met diagnostic criteria for major depression at follow-up than in the other conditions. These findings have important implications for future early intervention research and practice.
Major depressive disorder (MDD) is one of the most common and costliest psychological disorders (Chisholm et al., 2016; Kessler et al., 2007). Depression accounts for the greatest proportion of the world’s burden of disease as indexed by years lost to disability (Smith, 2014). Despite the high financial and personal costs associated with MDD, treatment is often unavailable or insufficient (Chisholm et al., 2016; Trivedi et al., 2006). Even with sufficient treatment, approximately 30% of individuals with MDD fail to remit (DeBattista, Solvason, Poirier, Kendrick, & Schatzberg, 2003). In addition, with each successive episode, the risk of another episode increases (see Dozois & Bieling, 2010) and the time between episodes decreases (Keller & Boland, 1998).
When depressive interventions occur earlier, with less chronic individuals, outcomes are often better (Curry et al., 2006). Early intervention could substantially reduce the societal and personal impact of this disorder (cf. Cuijpers, 2017). Indeed, even a prevention program that was successful only at delaying first onset would have a measurable impact, as early onset is associated with poorer prognosis (Burcusa & Iacono, 2007).
Depression prevention and early intervention research
A number of prevention and early intervention trials have been conducted, with the majority finding positive, significant results (see Muñoz, Cuijpers, Smit, Barrera, & Leykin, 2010). A recent meta-analysis found effect sizes incident risk ratio (IRR) for depression prevention trials ranging from .68 to .82 (van Zoonen et al., 2014). Several studies have also targeted young adults (Braithwaite & Finchmam, 2007; Cukrowicz & Joiner, 2007; Geisner, Neighbors, & Larimer, 2006; Seligman, Schulman, & Tryon, 2007) who represent a particularly high risk group for first-onset depression (Buchanan, 2012).
The Internet provides a particularly cost-effective and accessible dissemination tool for early intervention. Richardson, Stallard, and Velleman (2010) reviewed the use of computerized cognitive behavioral therapy (CBT) interventions for the prevention and treatment of depression. These authors referenced a number of distinct advantages to using computerized interventions (e.g., easily accessible, inexpensive; structured yet flexible delivery). Computerized therapies may also diminish barriers associated with stigma (Gega, Marks, & Mataix-Cols, 2003; MacGregor, Hayward, Peck, & Wilkes, 2009) and the demand for trained CBT providers (Griffiths & Christensen, 2007).
Current study
This article describes a randomized controlled trial that compared the effectiveness of two Internet-delivered interventions, CBT and attentional bias modification (ABM), in the prevention and early intervention of depression in at-risk undergraduate students. CBT and ABM are broad categories of interventions comprised of a number of more specific treatments. In the current study, MoodGYM (CBT) and the modified face-in-the-crowd-task (ABM; Dandeneau & Baldwin, 2004) were chosen as the interventions.
Cognitive behavioral therapy
MoodGYM, the CBT intervention, is an Internet-delivered, brief intervention aimed at reducing affective symptoms. MoodGYM has wide empirical support and has been used for the prevention (Lintvedt et al., 2013; O’Kearney, Gibson, Christensen, & Griffiths, 2006; O’Kearney, Kang, Christensen, & Griffiths, 2009) and treatment of mild-to-moderate depression (Christensen, Griffiths, Mackinnon, & Brittliffe, 2006; Mackinnon, Griffiths, & Christensen, 2008).
Lintvedt et al. (2013) examined the efficacy of MoodGYM as a preventative intervention in a sample of undergraduate students. The authors found that MoodGYM was effective at reducing depressive symptoms; however, due to both sample size and design, there was no investigation of whether CBT reduced the prevalence of MDD. O’Kearney and colleagues integrated MoodGYM into the school curriculum and explored its effect on adolescent male (O’Kearney et al., 2006) and female (O’Kearney et al., 2009) students. Adolescent males in the MoodGYM condition showed a slight reduction in depressive symptoms over the care-as-usual controls at post-intervention, but these effects were not maintained at follow-up. The authors referenced poor adherence in the sample as a possible complication. O’Kearney, Kang, Christensen, and Griffiths (2009) found that MoodGYM was more effective for female students than was the control condition at follow-up but not post-intervention. A notable limitation is that none of these trials measured diagnostic outcomes. This is an important outcome measure, as symptoms and diagnostic outcomes are not synonymous and the primary aim of prevention and early intervention is to reduce the prevalence of disorder.
Attention bias modification
Preventative CBT strategies have been effectively implemented over the past decade (Carlbring, Ekselius, & Andersson, 2003; Spek, Cuijpers, et al., 2007). ABM, on the other hand, is relatively new and has not yet acquired a large empirical base. Individuals with emotional disorders have a tendency to over-attend to negative information, that is, they exhibit negative attentional biases. ABM acts by training individuals to attend away from negative information and to actively engage with positive or neutral information (a pattern of attention often seen in healthy individuals; Mogg, Bradley, & Williams, 1995).
Attentional biases are causally related to the maintenance of depression (McDermott & Dozois, 2015). When individuals attend predominantly to negative information, they are more likely to consolidate that information into short-term and long-term memory (Koster, De Raedt, Leyman, & De Lissnyder, 2010). Thus, attention bias can contribute to an altered view of the world, and modifying these biases through ABM may improve information processing and perception. ABM techniques are developed from tasks originally designed to measure attentional biases. Through slight modifications to the original paradigms, ABM tasks have been able to modify, rather than simply measure, attentional allocation in individuals with anxiety and depression (Mathews & MacLeod, 2002; Wells & Beevers, 2010). Two tasks that are commonly modified are the dot-probe and the “face-in-the-crowd” task.
A number of studies have successfully used ABM for the treatment of anxiety disorders (e.g., Amir, Beard, Burns, & Bomyea, 2009; Amir, Beard, Taylor, et al., 2009). Using the dot-probe task, Wells and Beevers (2010) demonstrated that training a positive attentional bias effectively reduced depressive symptoms post-intervention and at follow-up. Dandeneau, Baldwin, Baccus, Sakellaropoulo, and Pruessner (2007) found that a group of telemarketers who underwent positive attention training, using the modified face-in-the-crowd task, experienced less stress, demonstrated higher self-esteem and sold more products than did controls. Browning, Holmes, Charles, Cowen, and Harmer (2012) used a modified dot-probe task to reduce relapse in individuals with recurrent depressive episodes. These results are impressive, particularly when cost-effectiveness is considered. Traditional psychosocial treatments are expensive to implement because they require trained professionals and treatment facilities. Even online interventions typically require a considerable amount of reading and extra-therapy tasks. In contrast, ABM can be conducted electronically, over the Internet, with little facilitator involvement. In addition, ABM is largely passive in administration, requiring less engagement and effort on the part of participants.
Information processing
Biased information processing is a common and modifiable vulnerability factor in depression (Dozois, Seeds, & Collins, 2009) and is targeted by both ABM and CBT. Individuals with depression have been shown to have biases at early levels of processing—trouble disengaging from negative content (Mogg et al., 1995) and at higher levels of information processing—interpretation (Leppänen, Milders, Bell, Terriere, & Hietanen, 2004) and memory (Dalgleish & Watts, 1990). Dual-system models have been used to describe the cognitive systems involved in processing negative content in depression (Beevers, 2005; Haeffel et al., 2007). These models suggest that there are two competing processes—associative and rule-based—which compete to direct the way information is processed (also see Ouimet, Gawronski, & Dozois, 2009). The associative system is described as a spreading pattern of associations that are rapidly activated. In contrast, the rule-based system involves applying a system of rules to the processing of information and the factual relationships among concepts. Unlike the rule-based processing system, the associative system is based on a bottom-up processing system. The associative system processes incoming information directly, making decisions based on the available data.
Many of the early processing biases, previously conceptualized as “automatic,” represent processes of the associative system. The attentional biases seen depression (Mogg et al., 1995) would be conceptualized as biases of the associative system. By contrast, dysfunctional attitudes, core beliefs, and maladaptive thinking patterns are functions of the rule-based system. Thus, CBT targets information using top-down or rule-based level processing, whereas ABM targets information processing from a bottom-up process, at the associative level. CBT and ABM are thought to prevent, or lower the risk of, depression by altering biased information processing and thus are both good candidates for transdiagnostic preventions. One purpose of this trial was to assess whether targeting these different processing systems (top-down vs. bottom-up) is differentially effective at preventing depression symptoms and onset.
Although the potential of ABM is promising, previous studies have been short-term, and no prevention studies have measured MDD diagnostic outcomes. In addition to representing the first study to directly compare CBT and ABM as preventative/early interventions, this research contributes significantly to the depression prevention literature using an active control group, measuring diagnostic outcomes, and directly addressing attrition. Most prevention and early intervention trials have used wait-list or care-as-usual controls. Although these conditions are economical, they do not effectively control for the influence of performance bias, demand characteristics, and placebo effects (Mohr et al., 2009). To establish that the results of the current study were not influenced by such biases, an active control condition was included.
Although Internet-delivered interventions have purported advantages, few prevention and early intervention studies have measured diagnostic outcomes. Such measurement is important because reducing the frequency of an MDD is the primary target of these interventions. Finally, Internet-delivered prevention research has had considerable rates of attrition; on average, only 50% of participants remain in a given study at follow-up (Lintvedt et al., 2013; Spek et al., 2008; Spek, Nyklicek, et al., 2007). Warmerdam, van Straten, Jongsma, Twisk, and Cuijpers (2010), for instance, found that only 37.5% of participants completed all five Internet sessions. High attrition rates can significantly affect the validity of outcome trials. To address this issue, the current study implemented a structured participant reminder system to increase participant adherence.
Research has not yet determined whether Internet-delivered CBT or ABM is more effective at reducing depressive symptoms and preventing disorder onset. Given support from past research, both conditions were expected to reduce MDD frequency and symptom severity. In addition to providing a direct comparison of the preventative potential of CBT and ABM, this study was also the first to use ABM as an early intervention for depression. An attentional control condition was also introduced, and the attentional training condition was expected to outperform this condition.
Method
Participants
Participants were first- or second-year undergraduates, fluent in English, able to access to an Internet-connected computer or touch screen device, and between the ages of 17 years and 64 years. Participants also had to score 22 or higher on the Kessler Distress Scale (K-10) (Kessler et al., 2002) or 35 or higher on the NEO Five-Factor Inventory (NEO-FFI) neuroticism index (McCrae & Costa, 2004).
Measures
Kessler Distress Scale
The Kessler Distress Scale (K-10) is a 10-item, multiple-choice measure designed to screen for nonspecific psychological distress (Kessler et al., 2002). The K-10 has been used over the Internet to screen for depression (Donker, van Straten, Marks, & Cuijpers, 2009) and has demonstrated high internal reliability (α = .90). In this study, a lower cutoff (i.e., scores > 22) was used to create a high-risk group rather than a likely pathological group, similar to previous studies (e.g., Christensen, Griffiths, & Jorm, 2004). Cronbach’s α was .81 in the current sample.
NEO Five-Factor Inventory
The neuroticism subscale from the NEO Five-Factor Inventory (NEO-FFI) is a 12-item, Likert-type scale (McCrae & Costa, 2004). The NEO-FFI neuroticism scale typically has coefficient αs ranging from .79 to .85 (McCrae & Costa, 2004; Sherry, Hewitt, Flett, Lee-Baggley, & Hall, 2007). A cutoff score of 35 was selected which corresponds to the 60th percentile of young adults (McCrae & Costa, 2010). In the current sample, the internal reliability was acceptable (α = .88).
Beck Depression Inventory II
The Beck Depression Inventory-II (BDI-II) is a 21-item measure that assesses presence and degree of depressive symptoms consistent with the description of MDD (Beck, Steer, & Brown, 1996). This instrument has strong empirical support for its use in clinical (Beck et al., 1996) and nonclinical (Dozois, Dobson, & Ahnberg, 1998) populations. Storch, Roberti, and Roth (2004) found excellent internal consistency for the BDI-II with a Cronbach’s α coefficient of .90 in an undergraduate university sample. The internal consistency (Cronbach’s α) was excellent (α = .90) in the current sample.
Depression Anxiety and Stress Scale 21
The Depression Anxiety and Stress Scale 21 (DASS-21) is a shortened version of the DASS-42 (Lovibond & Lovibond, 1995a). The DASS-21 and the DASS-42 have very consistent psychometric properties and high convergent validity (Dozois, Wilde, & Dobson, In Press). The depression subscale, used in this study, exhibits high internal consistency (α = .88; Lovibond & Lovibond, 1995b). Cronbach’s α for the DASS-21 depression subscale was .86 in this sample.
Structured Clinical Interview for the DSM-IV, I, non-patient version
The Structured Clinical Interview for the DSM-IV, I, non-patient version (SCID-I/NP) is a semi-structured interview designed to assess psychiatric diagnoses in nonpsychiatric populations. The SCID-I is considered the “gold standard” for diagnostic assessment in research studies (First, Spitzer, Gibbon, & Williams, 1997b). SCID-Is were administered by senior, clinical PhD students either in-person or over the phone at follow-up. Participants were interviewed about current and past depressive episodes at this time. All interviewers were blind to participant condition (First, Spitzer, Gibbon, & Williams, 1997a). 1
Interventions
MoodGYM/CBT
MoodGYM is an empirically supported, Internet-administered, intervention (Christensen, Griffiths, & Korten, 2002). MoodGYM (http://moodgym.com.au) consists of five individual modules containing 29 exercises and assessments, an interactive game, and resource downloads (see Appendix A). Each module is intended to take participants between 40 min and 1 hr to complete (see Christensen et al., 2002, for a detailed description).
ABM task
In the modified face-in-the-crowd task (Dandeneau & Baldwin, 2004), participants repeatedly search through arrays of facial images displaying a mix of negative emotions (angry, sad, and disgust) to find an image that depicts a happy expression. In the training condition, participants were always asked to search for a positive face and thus the target face always displayed a happy expression.
The facial stimuli for this task were adopted from the Montreal Set of Facial displays of emotion (Beaupré & Hess, 2005). Four sets of gray-scale facial expressions were selected: happy, sad, angry, and rejecting. Faces displaying happy expressions were classified as positive, whereas the faces displaying sad, angry, or rejecting faces were classified as negative faces. There were four Caucasian female, Caucasian male, Hispanic female, and Hispanic male models. Thibault, Bourgeois, and Hess (2006) coded each face using the Facial Action Coding System and found that participants correctly identified the emotion displayed 85% of the time.
The faces were displayed in a four by four matrix containing all 16 models. The location assignment of each face was random with the restriction that the same model would never display the target face in the same location on two consecutive trials. In the training trials, 15 models displayed a negative facial expression (sad, angry, or disapproving), while one model, the target face, displayed a positive facial expression. Each model displayed the target face nine times, but the order was randomized, as was the type of facial expression (sad, angry, or disapproving) displayed by the nontarget faces. Each training session included 6 blocks of 24 trials for a total of 144 trials. Participants completed this task semiweekly, and each session was designed to take 20 min to complete. This task has been validated for positive attentional training over the Internet (Dandeneau & Baldwin, 2004).
Attentional control condition
Participants in the control condition completed a task that was nearly identical to the ABM condition; however, instead of consistently searching for a positive face, participants were asked to search for both positively- and negatively valenced faces in equal proportion (on alternating blocks). When searching for negatively valenced faces, any of the three negative emotions were equally likely to appear. Participants completed 6 blocks of 24 trials. As in the ABM task, the control task was completed twice a week and took approximately 20 min. The same facial stimuli were used. The control task mimicked the original face-in-the-crowd task (Hansen & Hansen, 1988), which measures information processing and attention allocation although purportedly does not alter attentional bias or mood.
Procedure
Recruitment and compensation
Participants were recruited via posters, in class presentations, and a mass e-mail sent to all first- and second-year students. Participants were paid for each portion of the study that they completed, for a total available compensation of CAN$130.
Screening
Before enrolment, participants completed brief online screening questionnaires (i.e., the K-10 and the NEO-FFI) to assess eligibility. Individuals scoring above the cutoff on either questionnaire were invited to participate. Emotional distress and neuroticism were selected over symptom criteria to capture individuals who were at risk but not necessarily currently symptomatic. Both the NEO-FFI and the K-10 were used to target two different types of risk factors; the NEO-FFI was intended to target individuals who exhibited personality factors that put them at risk for depression, whereas the K-10 tracked individuals who might currently be in distress and thus could capture more situational or environmental risk factors. Participants who agreed to participate in the study were randomly assigned, by computer, to one of the three conditions (CBT, ABM, or attentional control) and were later contacted by a researcher for study orientation.
Baseline
Week 1: After providing electronic, informed consent, participants completed two interactive tasks (not included in this study 2 ), the BDI-II: (Beck et al., 1996), the DASS-21 (Lovibond & Lovibond 1995a), and some additional questionnaires that were not the focus of the current investigation. These questionnaires were delivered randomly to participants in four preset orders. This session took participants approximately 75 min.
Interventions
Week 2–7: Participants completed their assigned intervention during the 6 weeks following their baseline session. Participants in the CBT condition underwent six weekly sessions of MoodGYM. For the first 5 weeks, a new module became available every week, and the sixth week afforded participants the opportunity to complete remaining portions of sessions or review previously covered material. Participants were asked to spend 40 min a week on MoodGYM, complete sessions in one sitting, and only log on to MoodGYM when prompted.
Participants in the ABM and control intervention completed 12, 20-min, semiweekly sessions of a modified face-in-the-crowd task. Participants were prompted to complete these tasks every 3–4 days. Participants were asked to complete the tasks in one sitting and to use the same device each time.
Post-intervention
Week 8: During the post-intervention phase, participants completed the same tasks and questionnaires as at baseline.
Structured reminder schedule
If participants did not complete each session within 24 hr they received an automated reminder and those who still had not completed the task 48 hr later received reminder phone calls and/or personalized e-mails. Participants received repeat promptings until (1) they completed the task; (2) they indicated an intention to withdraw from the study; or (3) 2 weeks elapsed, at which time they were deemed non-contactable. To encourage timely completion of tasks, participants were placed in a draw for CAN$100 every time they completed the weekly task on time.
Follow-up
Week 23–25: Sixteen weeks after completing the intervention participants were instructed to complete the same series of questionnaires as at baseline and post-intervention. Completion of these questionnaires took approximately 45 min. Participants were also administered an SCID-I interview (First et al., 1997a). With permission, these interviews were audio recorded to establish inter-rater reliability. Participants who endorsed suicidal ideation were screened for risk and referred to appropriate resources, if necessary. After the interview, participants were debriefed and compensated. All participants were informed about available mental health resources as part of the debriefing process. Participants who completed the entire study received CAN$130 in compensation, whereas those who only completed a portion were compensated proportionally.
Results
Participant enrolment
Eight hundred and sixty-six participants completed the screening questionnaire and provided demographic information. Of those participants, 564 met criteria for the study and were invited to participate. Only 456 actually enrolled in the study and completed the baseline questionnaire. A Consolidated Standards of Reporting Trials diagram is displayed in Figure 1.
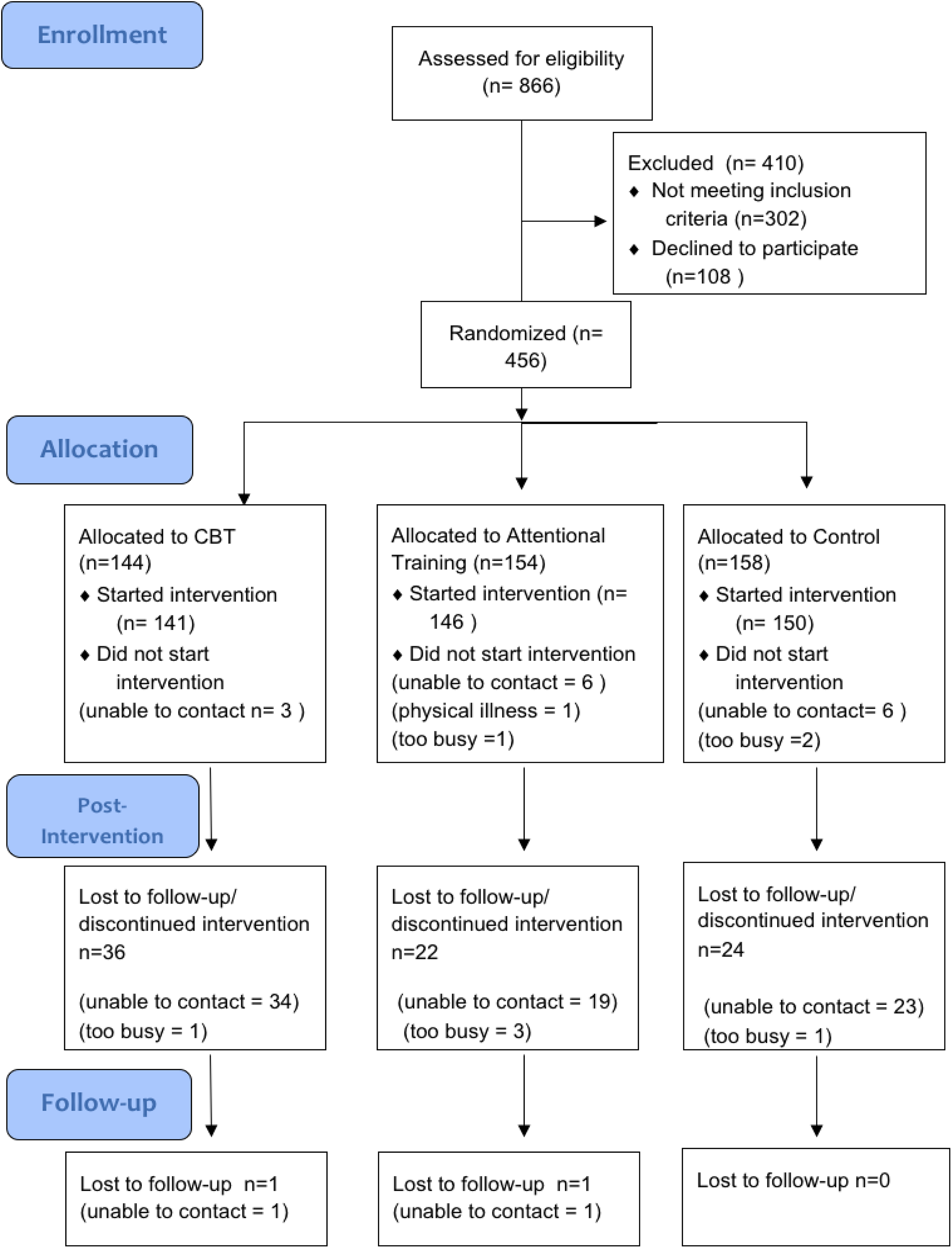
CONSORT diagram. CONSORT: Consolidated Standards of Reporting Trials.
Baseline characteristics and demographics
Demographic information and symptom scores by condition are presented in Table 1. There were no significant differences across the three conditions in age, F(2, 453) = 0.12, p = .89; gender, χ2(1, 465) = 1.96, p = .38; or ethnicity, χ2(6, 465) = 13.61, p = .33. There were also no significant symptom differences across the three conditions based on the BDI-II, F(2, 450) = 1.68, p = .19; DASS-21, F(2, 450) = 1.89, p = .15; K-10, F(2, 448) = 1.25, p = .29; and NEO-FFI-neuroticism, F(2, 449) = 0.89, p = .41.
Sample characteristics by condition.
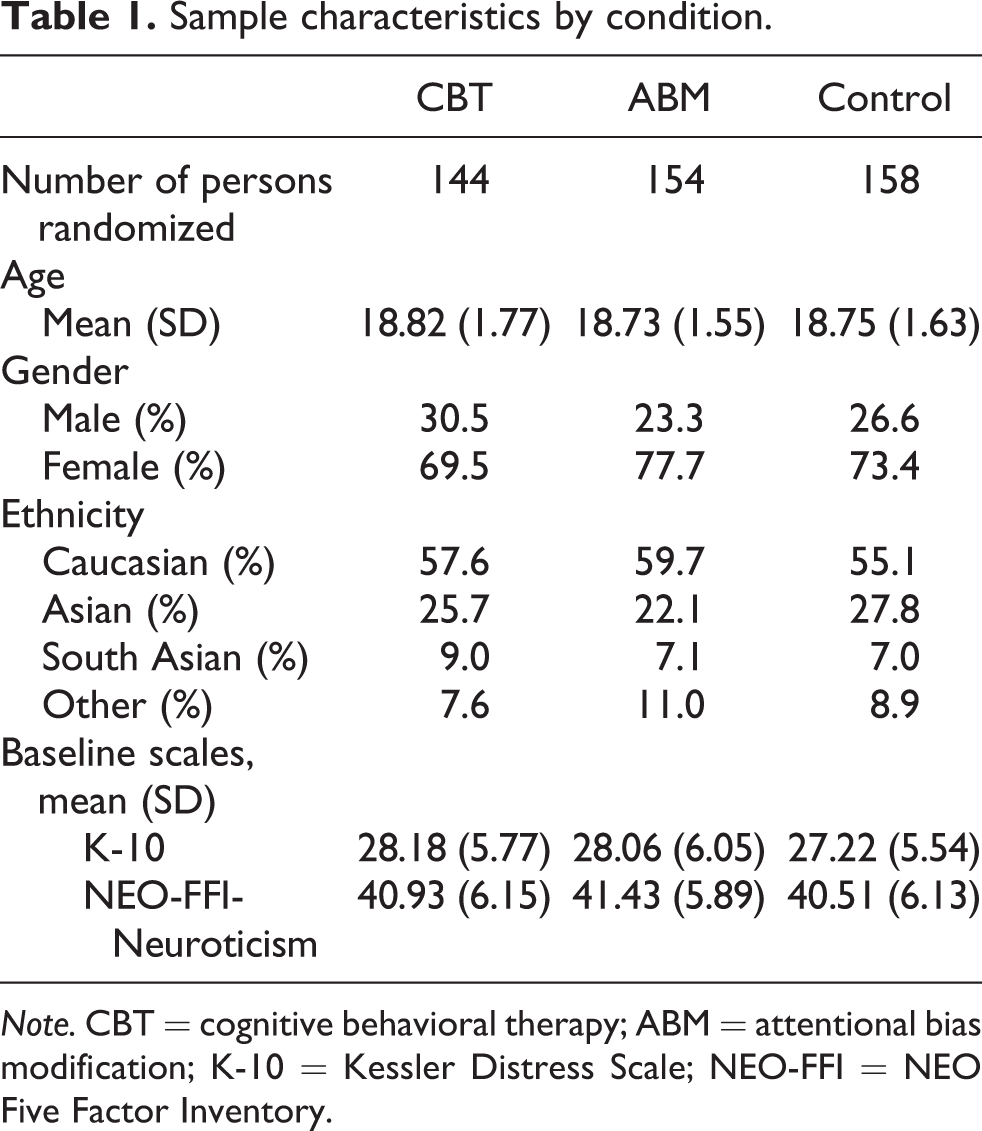
Note. CBT = cognitive behavioral therapy; ABM = attentional bias modification; K-10 = Kessler Distress Scale; NEO-FFI = NEO Five Factor Inventory.
Attrition
The rate of attrition between baseline and follow-up was 22.8% in this study with most dropouts occurring between baseline and post-intervention. Indeed, only two participants (one in the CBT and one in the ABM condition) left the study between post-intervention and follow-up. Thirty-eight participants withdrew from the CBT, 30 from the ABM, and 32 from the attentional control condition. There was no significant difference in attrition across the three conditions, χ2(2, 456) = 2.78, p = .25. There was no significant difference between completers and dropouts in age, F(1, 451) = 0.03, p = .85, or gender, χ2(1, 456) = 0.58, p = .44. However, there was a significant difference between the attrition and the completer groups in ethnicity, χ2(6, 456) = 17.11, p < .01. Follow-up analysis revealed that Caucasians were more likely to remain in the study (60% vs. 48.5%), χ2(1, 456) = 2.43, p < .05, whereas individuals who identified themselves as South Asians were less likely to remain in the study, (6.0% vs. 13.9%), χ2(1, 456) = 7.01, p < .01. Participants who withdrew were more likely to have lower scores on the BDI-II, F(1, 451) = 5.63, p < .05. To account for the impact of attrition, the depression outcome measures were analyzed using multiple imputation intent to treat analysis.
Beck Depression Inventory-II
The mean BDI-II scores are included in Table 2. An omnibus, split-plot analysis of variance (ANOVA) comparing Condition (CBT, ABM, Control) and Time (Baseline, Post-intervention, Follow-up) was conducted with the intent-to-treat data. 3 There was a significant main effect of Time, F(1.98, 895.43) = 38.31, p < .001, indicating that participants’ BDI-II scores improved overall (the Greenhouse-Geisser adjustment was used due to violations in the assumption of sphericity). There was no significant main effect of Condition, F(2, 895.43) = 1.54, p = .21. There was a significant two-way interaction of Condition by Time, F(3.95, 895.43) = 2.783, p < .05, indicating that there were group differences in how participants’ symptoms improved over time. A graphical representation of results is presented in Figure 2.
Mean and standard deviations of depression symptom scores.
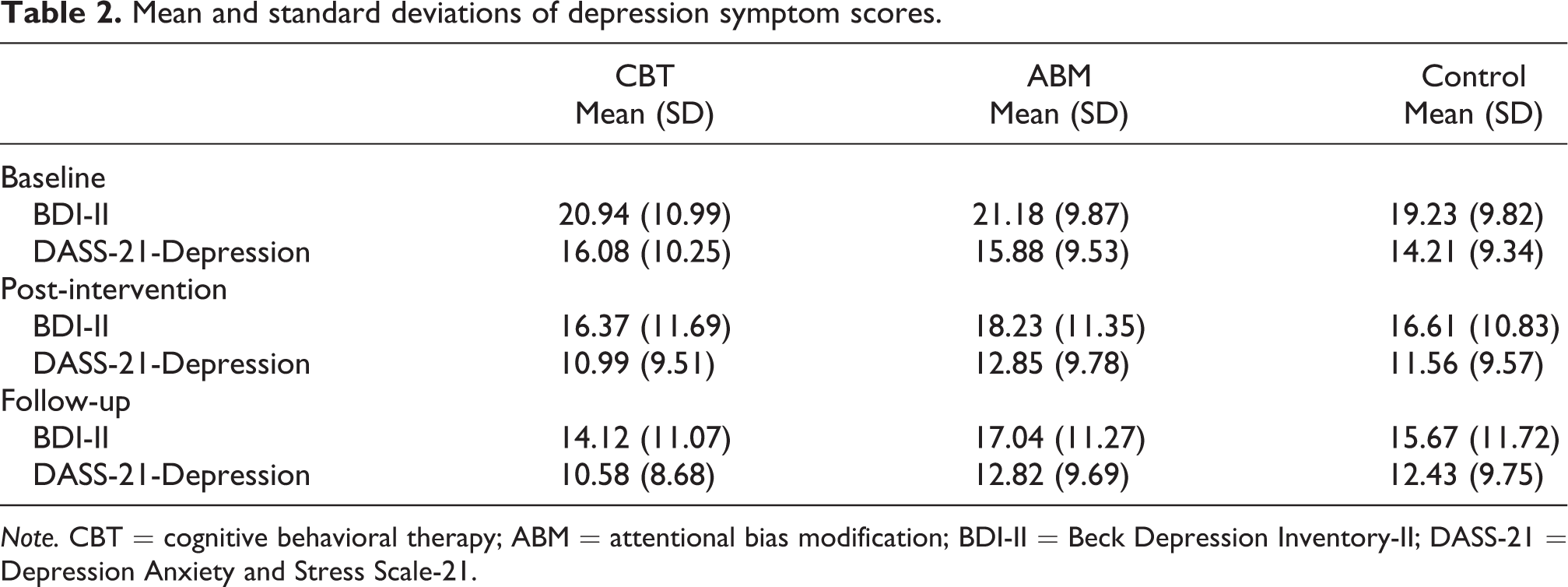
Note. CBT = cognitive behavioral therapy; ABM = attentional bias modification; BDI-II = Beck Depression Inventory-II; DASS-21 = Depression Anxiety and Stress Scale-21.
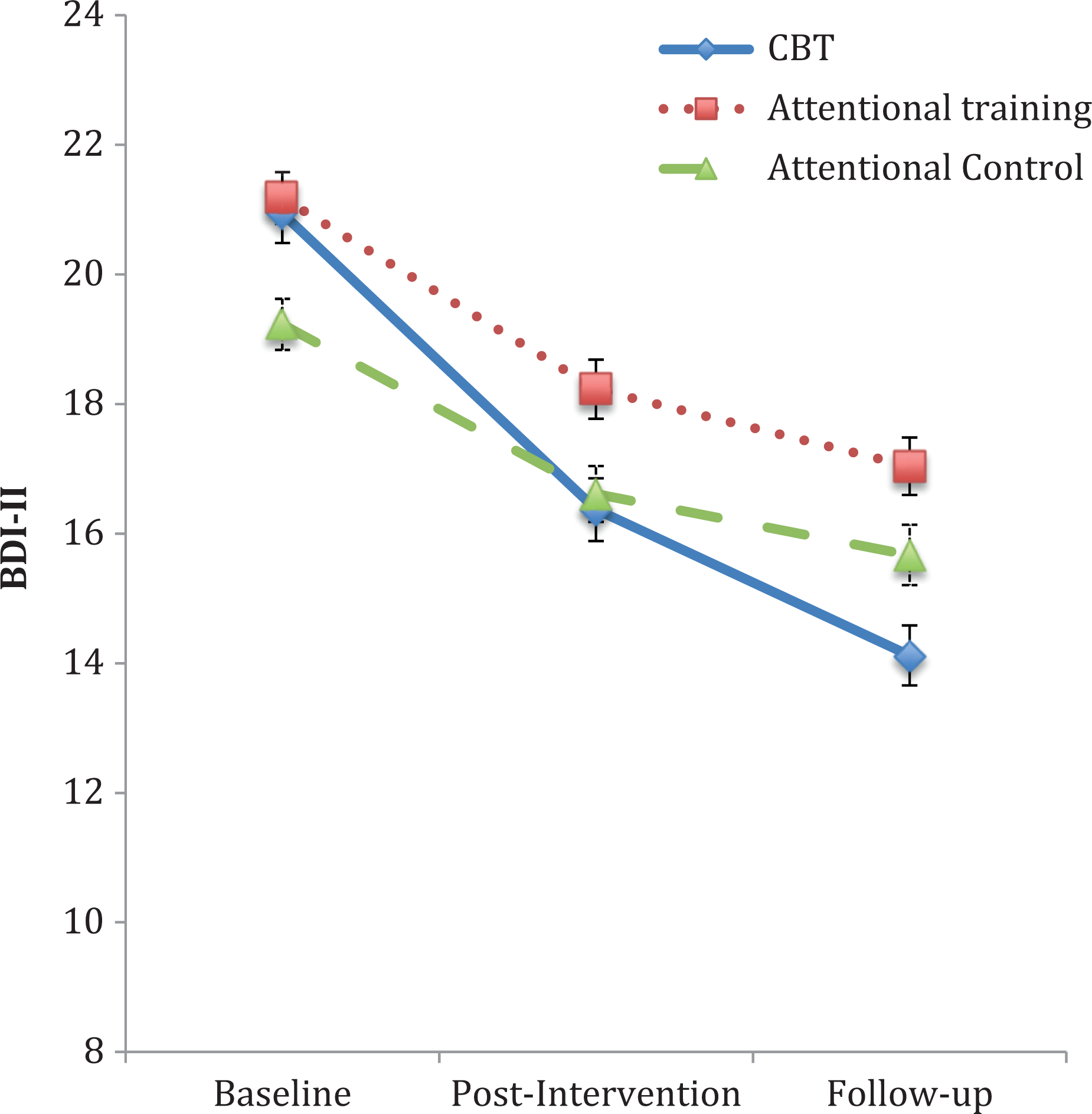
Beck Depression Inventory-II symptom scores across conditions at baseline, post-intervention, and follow-up.
A priori follow-up contrasts compared CBT to the ABM condition and ABM to the attentional control condition. Participants’ improvement was compared from baseline to post-intervention. The two attentional conditions exhibited statistically similar rates of change, F(1, 668) = 0.44, p = .66. By contrast, the CBT condition significantly outperformed the ABM condition, F(1, 668) = 2.09, p < .037. The same pattern of results was replicated with the observed improvement from baseline to follow-up. There was no statistical difference in the rate of change between the attentional groups, F(1, 668) = 0.77, p = .44. In contrast, the CBT group improved to a greater extent than the ABM group over time, F(1, 668) = 11.95, p < .001.
Depression subscale of the DASS-21
Mean scores on the depression scale of the DASS-21 across conditions are also reported in Table 2. A split-plot ANOVA was conducted, analyzing Condition (CBT, ABM, Control) by Time (Baseline, Post-intervention, Follow-up). The main effect of Time was significant, F(1.98, 895.11) = 41.87, p < .001, but there was no main effect of Condition, F(2, 895.11) = 1.67, p = .19. The main effect of Time was qualified by a significant interaction, F(3.96, 895.11) = 2.88, p < .05, which indicated that there was a difference in how the three conditions improved over time (see Figure 3).

Depression scale of the Depression Anxiety Stress Scale-21 symptom scores across conditions at baseline, post-intervention, and follow-up.
Participants’ improvement was compared from baseline to post-intervention. There was no significant difference between the attentional conditions, F(1, 668) = 1.70, p = .09, but the CBT condition showed significantly greater improvement than did the ABM conditions, F(1, 668) = 9.00, p < .001. From baseline to follow-up, the change in the attentional conditions differed statistically, F(1, 668) = 5.72, p < .001, with the ABM condition showing greater improvement. The CBT condition improved more than did the ABM condition, F(1, 668) = 10.66, p < .001.
Diagnostic outcomes
To test for the presence of baseline differences in the frequency of MDD, an analysis was conducted on participants’ recalled previous episodes of depression. At baseline, 15 participants in the CBT, 15 in the attentional control condition, and 22 in the ABM condition reported experiencing depression according to SCID-I criteria. There was no significant difference in the frequency of depression across conditions, χ2(1, 337) = 1.64, p = .44, at baseline.
Diagnostic outcomes were based on the results of the SCID-I. A χ2 analysis was used to determine if there were any significant differences in diagnostic outcomes across conditions. Current MDD was not combined with other mood disorders (e.g., dysthymia or depression NOS) as these disorders were both infrequent and not targets of this intervention. There were 5 cases of depression in the CBT condition, 11 in the control condition, and 18 in the ABM condition. Consistent with the initial hypothesis, there was a significant difference in the prevalence of MDD across the three conditions, χ2(2, 350) = 6.33, p < .05.
Follow-up analyses followed the same model used on the earlier symptom data. There were no significant differences between the two ABM conditions, χ2(1, 248) = 2.11, p = .15. However, significant differences existed between the prevalence of MDD in the CBT and attentional conditions, χ2(1, 227) = 6.087, p < .013, suggesting that the prevalence of MDD was significantly lower in the CBT condition.
Discussion
This study compared the efficacy of three interventions at reducing the symptom severity and frequency of MDD. Participants completed one of three 6-week interventions consisting of an Internet-delivered CBT program (MoodGYM), ABM (modified face-in-the-crowd task), and an attentional control condition (unmodified face-in-the-crowd task). Depression symptoms were assessed at three testing intervals: baseline, post-intervention, and follow-up. Diagnostic outcomes were assessed at follow-up.
It was unknown how the ABM and CBT conditions would compare on MDD prevalence and symptom severity. MoodGYM outperformed the ABM at reducing MDD symptoms and frequency. A second hypothesis was that the ABM condition would outperform the attentional control condition. However, no significant differences were found between the ABM and attentional control conditions. This finding suggests that the MoodGYM condition was the most effective intervention at both the diagnostic and symptom levels.
The results of this trial have important implications for future prevention and early intervention implementation and research. The active control condition provided an effective control for placebo effects and demonstrated that the effects observed in the CBT condition were valid and not simply artifacts of experimental methodology or participant bias. The diagnostic outcomes match the findings at the symptom level. The lower than usual attrition rate allowed for intent-to-treat analysis which replicated the differences seen between the CBT and the attentional conditions in the conventional analysis, confirming that even after accounting for attrition, the CBT condition outperformed the other two conditions at reducing depressive symptoms.
Efficacy of MoodGYM
An important aspect of these findings is that MoodGYM demonstrated superior results both at post-intervention and follow-up. In fact, there was marked improvement from baseline to follow-up, with relatively powerful effects, Cohen’s d = .40 and .51 (based on the BDI-II and DASS-21, respectively). Cohen’s ds of .5 represent a medium effect size (Cohen, 1973). These findings are notable, particularly given that the effects are based on a comparison to an active intervention (i.e., treatment conditions often show less comparative improvement when matched to active than non-active controls; see Horowitz & Garber, 2006; Jane-Llopis, Hosman, Jenkins, & Anderson, 2003; Stice, Shaw, Bohon, Marti, & Rohde, 2009).
Lintvedt and colleagues’ (2013) MoodGYM prevention trial provides a good comparison as it had a similar population (university students) and recruitment criteria (a score above 20 on the K-10). Unlike the current study, Lintvedt and colleagues used a wait-list control condition and did not include a follow-up component. Using change contrasts, as the current study did, the authors found a large effect for the comparative change from baseline to post-intervention (d = .57). The current study had slightly smaller effects at post-intervention (d = .37 and .48) but similar or larger effects at follow-up (d = .57 and .65). In a meta-analysis of Internet-delivered prevention studies, Spek et al. (2007) found small-to-medium depression prevention effect sizes (d = .27–.32).
The strong follow-up results are particularly compelling. As a treatment, it is often argued that CBT prevents relapse better than other interventions (Fava, Rafanelli, Grandi, Conti, & Belluardo, 1998; Jarrett et al., 2001; Paykel, 2007). Potentially, the long-term benefit seen during treatment may also be present in briefer less intensive interventions. Additional research is clearly needed, with longer term follow-ups, to establish the longevity of such benefits or to ascertain if continued improvement is maintained.
Other trials have demonstrated positive follow-up effects and, similar to this study, some have found even stronger effects at follow-up than post-intervention. O’Kearney et al. (2009), for instance, implemented a universal, CBT preventative intervention with adolescents girls. Although the authors did not find significant effects post-intervention, they did at follow-up. Van’t Veer-Tazelaar et al. (2009) conducted a staged prevention trial; after a year, the intervention condition was twice as effective as the care-as-usual control. There is also some limited evidence that Internet-delivered interventions might perform particularly well at follow-up. Spek et al. (2007, 2008) compared Internet- and group-administered CBT prevention. The two groups performed equally well at post-intervention but, at follow-up, the Internet-delivered condition appeared most effective. Although this is an interesting finding, it is important to note that attrition was higher in the Internet-administered group, which, as discussed earlier, could have inflated results.
The beneficial effects at follow-up have important implications for prevention and early intervention. In contrast to treatment, where the aim is to alleviate a current illness, in prevention/early intervention, the objective is to prevent the occurrence of a new illness or prevent the reoccurrence of previous disorders. Thus, the long-term utility of the intervention is important.
In addition to lower symptom levels, the CBT condition also exhibited fewer cases of MDD at follow-up. As diagnosis was only assessed at follow-up, it is theoretically possible that the difference in MDD prevalence also occurred at baseline; however, two results contradict this explanation. First, there were no significant differences in symptoms at baseline and the results trended in the opposite direction, with relatively higher scores in the CBT condition. Post-intervention symptom scores also corresponded with diagnostic findings.
Second, during the follow-up SCID-I interviews, participants were queried about previous depressive episodes and their approximate start and end dates. Comparing these results to participants’ study, start dates provided a measure of MDD frequency at baseline. No significant differences were found at baseline across the conditions. The strength of this evidence is somewhat reduced by the possibility of recall bias since participants were asked to recall events from the past. The ideal methodology would have been to interview participants at both baseline and follow-up. With this limitation acknowledged, the combined findings of no differences in symptoms or recalled occurrence of depression at baseline suggest that the diagnostic differences seen at follow-up are likely driven by the interventions rather than by chance findings.
MoodGYM’s impact on diagnostic outcomes is particularly important and adds to the symptom reduction findings. Although many studies have only examined symptom reduction as an outcome (Lintvedt et al., 2013; Vazquez et al., 2013), the true aim of prevention and early intervention is to prevent the onset of the targeted disorder (i.e., MDD). Diagnostic interviews are time-consuming to conduct and, as diagnosis is a dichotomous variable, unlike symptom measurement, larger sample sizes are needed to detect diagnostic differences. Thus, many researchers opt to use symptoms as the primary outcome measure, particularly in large, Internet-delivered trials. However, using both symptom and diagnostic measures, the current study was able to establish efficacy at both levels.
ABM findings
The second finding from this trial was that there were no significant differences between the ABM and the control conditions. This finding is consistent with recent research in the anxiety domain, where numerous studies have found that Internet-delivered ABM and attentional controls both reduce anxiety symptoms (Boettcher, Hasselrot, Sund, Andersson, & Carlbring, 2014; Carlbring et al., 2012; Neubauer et al., 2013). Enock, Hofmann, and McNally (2014) recently conducted an ABM trial to treat social anxiety comparing ABM, an attentional control, and a wait-list condition. The authors found, as in the current study, that ABM and the control condition performed identically, but outperformed the wait-list condition. What is unclear is whether this symptom reduction is due to experimental bias (e.g., placebo effects, natural symptom decline) or some active ingredient in the two interventions yet unaccounted for. Regardless of the cause of the MDD symptom decline in the attentional conditions, when compared to the MoodGYM, they do not appear to be as efficient at preventing depression.
Limitations
Although this study has numerous strengths, there are limitations that warrant mention. One limitation was that the SCID-I was not administered at baseline. Although participants were interviewed about historical depressive episodes, this method may be subject to participant recall bias. Another design improvement would entail longer follow-up periods. Regular yearly follow-ups would have provided information about the extended efficacy of the trial. Although the fact that improvements held and even increased at 4-month follow-up suggests that benefits may be sustained beyond the intervention period, it would require a multiyear study to know if such gains are maintained over longer periods. Another limitation is that participants were financially compensated to participate in this study, which limits the generalizability of these findings to “real-world” settings as it may have increased participants’ motivation to complete the trial.
Implications and future directions
The current study has important implications, which, in part, define the next steps for prevention research. One important question is how these results translate into implementation. Based on the results from this trial, it appears that MoodGYM is a superior option for selected/indicated prevention when compared to the attentional interventions. Given the efficacy of MoodGYM demonstrated in this trial, future research may wish to explore the effectiveness of this intervention under more naturalistic conditions. For example, future effectiveness research may wish to investigate a university wide implementation where all students are encouraged to participate in the intervention. Replication of these findings with the larger cohort would further support the efficacy of MoodGYM for early intervention and allow the exploration of its impact on other related problems such as stress generation (Hammen, 1991). Although an effectiveness trial has been conducted with MoodGYM Internet users (Christensen et al., 2002), additional effectiveness trials are warranted.
Effectiveness trials go hand in hand with cost-effectiveness research. Given that MoodGYM halved the rate of MDD in the current study, it may prove to be a highly cost-effective intervention. Previous studies have demonstrated the cost-effectiveness of prevention (Lynch et al., 2005; Smit et al., 2006), and other researchers have explored the cost-effectiveness of Internet-delivered treatment (Warmerdam, Smit, van Straten, Riper, & Cuijpers, 2010). However, a paucity of research has explored the cost-effectiveness of Internet-delivered prevention.
Summary
This prevention/early intervention trial established that MoodGYM may be effective at reducing the symptom-severity and onset of MDD. This trial strengthened the findings of other depression prevention studies by establishing the prevention effects of MoodGYM, comparing this program to an active intervention, reducing the bias from attrition, and examining diagnostic outcomes. This is the first study that measured diagnostic prevention outcomes using MoodGYM and one of the few prevention studies that used intent to treat and an active comparison condition. The attentional control and the ABM conditions, on the other hand, performed similarly, as has been observed in recent research.
Footnotes
Acknowledgements
The author would like to thank the University of Western Ontario for providing an Academic Development Fund (Major Grants Competition) and New Research and Scholarly Initiative Award.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Academic Development Fund (Major Grants Competition), New Research and Scholarly Initiative Award, awarded to the second author from the University of Western Ontario.