
Abstract
Background:
Postoperative cognitive dysfunction (POCD) is a common complication after anesthesia surgery, especially in older people, that can persist weeks or months after surgery as a short-term impairment of cognitive abilities, or even for a prolonged duration over years, potentially progressing into permanent cognitive dysfunction. However, the pathogenesis of POCD is not fully understood, and therefore an optimal solution for preventing POCD has yet to be established. Some studies have shown that intraoperative ketamine/esketamine reduces the incidence of POCD, but this remains controversial.
Objectives:
We evaluated the effect of intraoperative subanesthetic doses of ketamine/esketamine versus no intervention in adults undergoing general anesthesia surgery on the incidence of POCD.
Data Sources:
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and searched the PubMed, Embase, Ovid, Cochrane, Scopus, and Web of Science databases for the MeSH terms ‘ketamine’, ‘esketamine’, and ‘Postoperative Cognitive Complications’ from database inception to 25 June 2023.
Results:
We found no statistically significant difference in the incidence of POCD within 7 days for intraoperative subanesthetic dose of ketamine/esketamine compared with the control group [relative risk (RR) = 0.57, 95% confidence interval (CI): 0.32, 1.01], and the results from the subgroup analysis based on age (>60 years) also revealed that the difference was not statistically significant (RR = 0.49, 95% CI: 0.23, 1.04).
Conclusion:
Compared with controls, intraoperative subanesthetic dose of ketamine/esketamine has no advantage in preventing POCD in patients, or in elderly patients. This study provides reference data for POCD research and clinical drug intervention strategies.
Registration:
Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42023401159).
Introduction
Postoperative cognitive dysfunction (POCD) is one of the most common complications after anesthesia, with a prevalence of approximately 12%, 1 and a higher prevalence of up to 41.4% in older surgical patients during the entire hospitalization period.2,3 There is currently no consensus on the definition of POCD, 4 but it is commonly defined as a decline in cognitive abilities compared to the individual’s preoperative baseline level. 5 Most POCD persists weeks or months after surgery, 6 mainly manifested as impairment of cognitive abilities, including memory, mood, confusion, and sleep disturbances, often resulting in increased mortality, delayed recovery, unexpected complications, and prolonged hospital stay, especially in older people.7,8 In addition, some patients may experience POCD for a prolonged duration of up to years, 9 which could potentially progress into permanent cognitive dysfunction.4,10 The risk factors for POCD are multifaceted and exist in various stages of the perioperative period, including advanced age, history of cognitive impairment, type of surgery, intraoperative hypotension, time and depth of anesthesia, pain management, inflammatory biomarkers, and other related risk factors. 11 Postoperative neuroinflammation is regarded as one of the main pathogenic mechanisms contributing to the development of POCD. 12 However, the underlying pathophysiology of POCD is still unclear, and there are currently no effective strategies for prevention and treatment. 4 Consequently, the prevention of POCD has emerged as a major concern.
Ketamine, a non-competitive antagonist of N-methyl-
Ketamine is a versatile drug that has been widely used since the 1970s and is commonly employed for intraoperative anesthesia and adjunctive perioperative analgesia, 16 and it is commonly used for children 17 and burn victims, owing to its favorable cardiovascular characteristics and ability to reduce glandular secretion. 18 However, ketamine demonstrates sympathomimetic effects, including increased sympathetic activity, cardiac contractility, and heart rate, 19 while it may also aggravate psychiatric symptoms.20,21 Consequently, caution should be exercised in patients with preoperative hypertension, severe cardiovascular disease, preoperative severe psychiatric disease, and hyperthyroidism patients. In recent years, ketamine has been considered to have potential preventive effects on POCD, but its efficacy remains controversial. While several clinical studies have reported attenuates in the incidence of POCD with intraoperative ketamine, 22 conflicting findings have also been observed that intraoperative ketamine/esketamine may have no advantage in preventing POCD.23–25
Esketamine is an S (+) enantiomer of ketamine with indications broadly similar to those of ketamine, but offers the advantage of fewer adverse effects and shorter recovery time. 13 Li et al. 26 suggested that esketamine would alleviate surgery-induced POCD in rats via inhibition of the STING/TBK1 signaling pathway. According to research, the combined administration of esketamine and propofol had been shown to effectively reduce postoperative inflammatory and facilitate cognitive function recovery in elderly patients. 27 When considering ketamine and esketamine as one group, there is no significant difference between them in improving many cognitive functions in treatment-resistant depression (TRD) patients. 28 Nevertheless, there is insufficient evidence on the efficacy of esketamine as a novel drug for the treatment of POCD.
To explore the potential impact of ketamine/esketamine on the incidence of POCD, we present a systematic review and meta-analysis to determine whether the intraoperative subanesthetic dose of ketamine/esketamine infusion has preventive effects on POCD.
Methods
Protocol and registration
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines for reporting systematic reviews. 29 Study details including eligibility criteria, outcomes, and statistical methods were predefined (study protocol registered on PROSPERO – CRD42023401159).
Information sources and search
We searched six databases, including PubMed, Embase, Ovid, Cochrane, Scopus, and Web of Science with the MeSH terms ‘Ketamine’, ‘esketamine’, and ‘Postoperative Cognitive Complications’ from database inception to 25 June 2023.
Eligibility criteria
We included original studies in this review, if they assessed the effect of ketamine/esketamine on the incidence of POCD. Inclusion criteria: (1) patients undergoing general anesthesia surgery (any type of surgery), patients aged ⩾18 years old, and American Society of Anesthesiologists (ASA) classification I–III; (2) POCD was diagnosed using standardized neuropsychological tests, with quantitative testing methods including the Mini-Mental State Examination (MMSE), or other combination of neuropsychological tests based on the recommendations of International Study of Postoperative Cognitive Dysfunction (ISPOCD). Semi-qualitative testing methods such as the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU); (3) intervention/comparator groups consisting of ketamine/esketamine and controls; and (4) research reporting the incidence of POCD.
Studies that included the following patients were excluded: (1) patients with cognitive impairment before surgery; (2) patients with past long-term use of medication affecting neuropsychiatric function (hypnotics, anti-anxiety, and antidepressants); (3) patients with a history of neurological, psychiatric, and cardiovascular disease (e.g. Alzheimer’s disease, cerebral infarction, coronary artery disease, etc.); (4) patients with severe visual or auditory impairment and inability to perform neurocognitive function tests; or (5) patients with severe liver or kidney impairment.
Study selection
Two reviewers (NZ and CCC) reviewed the title and abstract independently, scored included studies, and extracted relevant data. In case of disagreement between reviewers, a third reviewer (YHC) will be consulted to resolve any disagreements.
Data collection process
The data extracted independently by two reviewers included demographic information, study methodology, interventions, the incidence of POCD, and route and dose of administration of ketamine/esketamine. If data were missing, we contacted the authors for more information.
Outcome indicators
We recorded the incidence of POCD at the study endpoint using validated diagnostic scales as the outcome. By comparing the difference in the incidence of patients with POCD between the group of intervention and control, evaluate the effectiveness of ketamine/esketamine in preventing POCD.
Quality evaluation
The quality evaluation was assessed using the Cochrane Collaboration Risk of Bias tool, 30 and two reviewers (NZ and CCC) independently assessed the risk of bias in each included study and a third reviewer (YHC) was consulted to resolve any disagreements.
Analytic methods
We used R version 4.2.1 for data analysis. Relative risk (RR) with 95% confidence intervals (CIs) for dichotomous data was used as the effect measure. We assessed the heterogeneity using the I2 statistic values as followed: 0–39% were small, 40–74% as moderate, and 75–100% as large, 31 and we used sensitivity analysis to explore sources of heterogeneity. Subsequently, subgroup analysis by age group (⩾60 years) was performed. Funnel plots were used to assess the presence of publication bias, an asymmetric graph suggested possible publication bias.
Results
Study selection
The search strategy identified a total of 404 records (Figure 1). After removing duplicate records, 226 articles remained, and we excluded 196 irrelevant records after screening by title and abstract, leaving 30 articles for full-text review. Finally, nine randomized controlled trials (RCTs) met the inclusion criteria.22–25,32–36
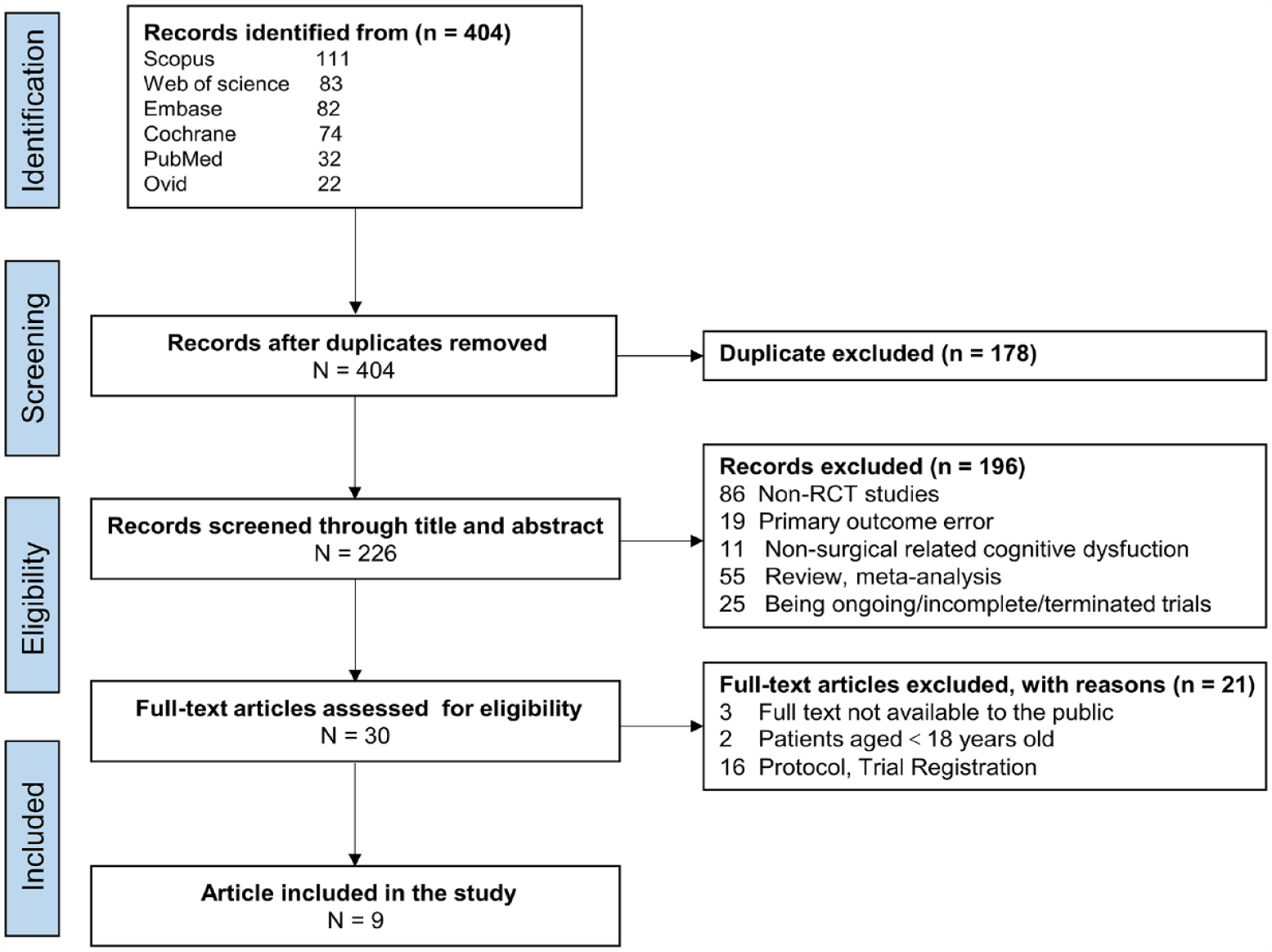
Flow chart of selection of the included studies.
Characteristics of studies, participants, and interventions
Table 1 provides an overview of the study characteristics. Nine RCTs involving a total of 573 patients between 2013 and 2023 were included in this study. Regarding the type of surgery, one study was cardiac surgery,22,32 one was both cardiac and noncardiac surgery, 24 and the others were non-cardiac.23,25,32–36 Ketamine use and dosage varied in different studies. Seven studies used ketamine,22,24,25,33–36 and two studies used esketamine.23,32 Most studies used interventional agents before and during induction,22,24,25,32,35,36 and three studies used continuous intraoperative infusion during surgery.23,33,34 Three studies with single-dose injections of ketamine were 0.5 mg/kg.22,25,35 One administration of esketamine is 0.3 mg/kg after induction, followed by an infusion of 0.2 mg/kg/h during surgery. 23 Another one is an intravenous injection 0.15 mg/kg during induction. 32 Most studies used ketamine alone, with one study using ketamine in combination with other drugs. One study used ketamine in combination with lidocaine 0.5 mg/kg/h during surgery. 36 All studies were completed within 7 days for the diagnosis of POCD, three studies were completed within 24 h of surgery,23,33,35,36 one study was completed within 48 h, 36 two studies were completed within 72 h,22,24 and three studies were completed within 6 and 7 days.25,32,34 Eight studies used quantitative testing methods to assess POCD, including MMSE-only,23,24,35 and a combination of neuropsychological tests based on the recommendations of ISPOCD.22,25,32,34,36 One study used a semi-quantitative approach as CAM-ICU. 33
Summary of study characteristics.

The study by Han (2023), Hudetz (2009), Lee (2015), Oriby (2023), and Zhu (2014) diagnosed POCD by choosing a series of neuropsychological tests based on the recommendations of ISPOCD.
CAM-ICU, Confusion Assessment Method for the Intensive Care Unit; ISPOCD, International Study of Postoperative Cognitive Dysfunction; iv., intravenous injection; ivgtt., intravenously gutte; MMSE, Mini-Mental State Examination.
Study quality and risk of bias
The risk of bias of all studies included was classified as ‘low risk’ to ‘some concerns’, with no study having ‘high risk’ (Figure 2). No significant bias was found in all included studies. Our overall assessment of the quality of all the research was moderate.

Risk of bias.
Effects of ketamine/esketamine on the incidence of POCD
The forest plot (Figure 3) summarizes the effect of ketamine/esketamine on the prevention of POCD in patients. Our included studies had moderate heterogeneity (I 2 = 56%), and a random effects model was used to calculate the effect size. Our results showed that effect of intraoperative ketamine/esketamine on the incidence of POCD within 7 days compared to the control group that was not statistically significant (RR = 0.57, 95% CI: 0.32, 1.01).

Forest plots of the effect of ketamine/esketamine in preventing POCD.
Effects of ketamine/esketamine on the incidence of POCD in elderly patients
We formed subgroups by age (>60 years old) and included six studies, presented with a forest plot (Figure 4). There was moderate heterogeneity in this forest plot (I 2 = 53%), and the results also showed that effect of ketamine/esketamine on the incidence of POCD in the elderly was not statistically significant (RR = 0.49, 95% CI: 0.23, 1.04).
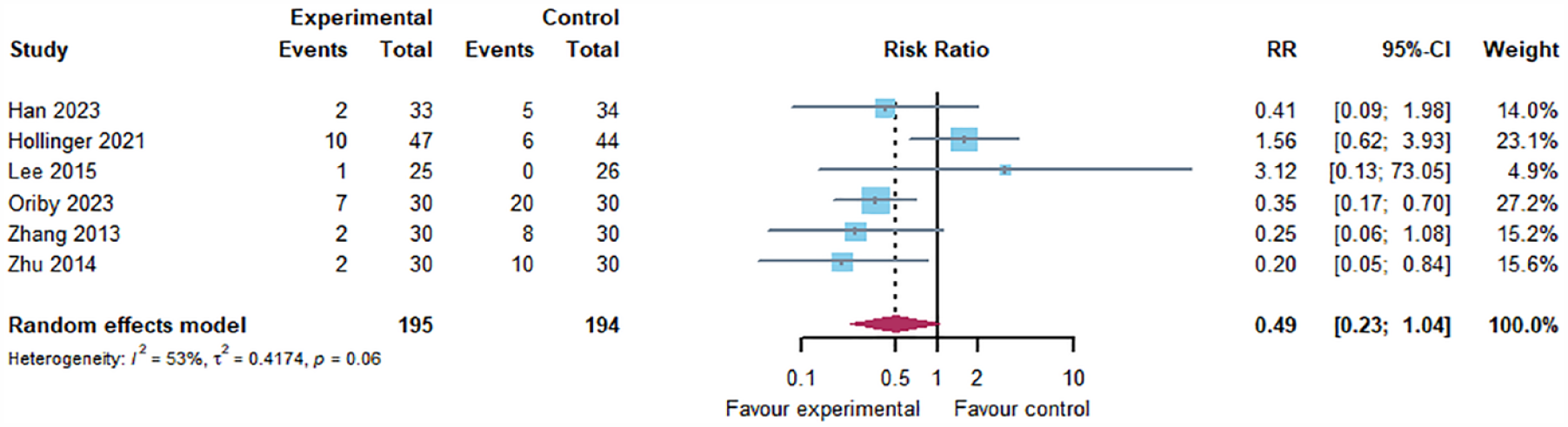
Forest plots of the effect of ketamine preventing POCD in older patients.
Sensitivity analysis
Sensitivity analysis (Figure 5) revealed no significant directional changes in the findings excluding either study and low heterogeneity among the included studies. The results had good stability.

Sensitivity analysis.
Publication bias
Funnel plots indicated that there was no significant publication bias (Figure 6).

Funnel plot of the effect of ketamine/esketamine in preventing POCD.
Discussion
In this systematic review and meta-analysis, we included a total of nine RCTs exploring the efficacy of an intraoperative subanesthetic dose of ketamine/esketamine in preventing POCD, and the results showed no advantage of ketamine/esketamine compared with controls in preventing POCD, and similarly, subgroup analysis showed insufficient evidence to support a protective effect of ketamine/esketamine in elderly patients.
This conclusion differs from previous similar studies. A systematic review included three RCTs with a total of 163 patients to evaluate the effects of intraoperative ketamine administration on POCD and showed that ketamine may offer some protection against POCD, but the quality of the evidence was deemed very low. 37 Li et al. 38 conducted a network meta-analysis of different drugs for the prevention of POCD in general anesthesia and showed that ketamine was somewhat effective in preventing POCD in cardiac or non-cardiac surgeries. It is worth noting that some clinical findings support our results. However, an RCT included 60 patients with ASA I–III for elective laparoscopic cholecystectomy under total intravenous anesthesia, and the results indicated that a subanesthetic dose of ketamine did not result in significant differences in cognitive function compared to the control group. 39 In addition, there were similar results in some fundamental studies. One study reported that intravenous administration of ketamine disrupts iron homeostasis and overloads hippocampal neuronal iron in vitro and in vivo cultures, thereby contributing to the development of neurodegenerative diseases in the elderly. 40 Hong et al. 41 also found that repetitive ketamine use may cause memory impairment or emotional disorders in adolescent mice.
The clinical effects of ketamine/esketamine may be related to the method of administration. In included studies in our meta-analysis, the intervention group either received ketamine/esketamine alone or a combination of ketamine/esketamine with another drug whose efficacy in preventing POCD has not been approved. Consequently, the use of ketamine/esketamine alone may not have a preventive effect against POCD, but some studies have suggested that a combination of ketamine/esketamine with other drugs may be preventive in this regard. In an RCT that included 100 participants, it was observed that older adults who received a single dose of ketamine during heart valve replacement surgery had a 20% incidence of POCD, which was significantly lower compared to the combined etomidate–ketamine group that had a 6% incidence. 42 In another RCT involving 182 patients, it was found that haloperidol and ketamine as individual treatments did not demonstrate a superior effect on the incidence of POCD compared with the control group (15.6% and 21.3% versus 13.6%); however, the combination group, which received both haloperidol and ketamine, exhibited a lower incidence of POCD compared to the control group (6.6% versus 13.6%). 24 Further research is needed to confirm the efficacy and safety of such combinations in preventing POCD.
Studies suggest that the inflammatory response may play a role in the pathogenesis and progression of POCD. 11 Surgical trauma-induced peripheral inflammation and the release of systemic inflammatory mediators have been shown to affect inflammatory processes in the central nervous system. 12 Therefore, inflammatory markers regarding nerve injury in POCD have also become a focus of interest for investigators. A meta-analysis of inflammatory markers in patients after undergoing total hip arthroplasty reported that preoperative C-reactive protein (CRP) and S-100β as well as post-operative CPR and IL-6 at 6 h were significantly higher in patients with POCD compared with non-POCD patients. 43 Animal studies on femoral fracture surgery have shown that elevated serum concentrations of IL-1β, IL-6, and TNF-α may suggest the development of an inflammatory response induced by femoral fracture surgery, which is consistent with the observations of elderly people with POCD after femoral fracture surgery. 44 Other experiments have also shown that serum concentrations of S-100β and neuron-specific enolase are elevated in aged dogs after surgery, which may contribute to nerve damage. 45 Hollinger et al.’s 24 findings were consistent with similar results, indicating a significant increase in S-100β levels among the POCD group compared to the preoperative baseline. These results suggest that an approach to alleviate and prevent POCD by reducing inflammation in the operative period seems to be feasible. However, ketamine has been found to exhibit an anti-inflammatory agent that promotes inflammatory homeostasis by modulating immunity. 46 A single dose of ketamine (0.25 mg/kg) given during induction of anesthesia significantly suppresses the increase of serum IL-6 in patients undergoing coronary artery bypass surgery. 47 A meta-analysis consisting of 14 RCTs investigated the impact of intraoperative use of ketamine on postoperative IL-6 levels, including a total of 684 patients, with eight studies focusing on cardiac surgery and six on noncardiac surgery, revealed that ketamine significantly suppressed the serum IL-6 inflammatory response in the early postoperative period. 48 A study of the postoperative inflammatory response to laparoscopic surgery found that pre-incisional administration of ketamine partially attenuated serum IL-6 and TNF-α concentrations compared to the control group. 49 Nevertheless, there are contradictory clinical reports regarding the efficacy of ketamine in reducing the inflammatory response to surgery. Recent clinical trials have also shown that the CRP and IL-6 levels and TNF-α in patients with intraoperative esketamine were not significantly different from controls in the postoperative period. 50 Cho et al. 51 measured IL-6, TNF-α, and CRP levels at multiple time points before and after colorectal cancer surgery in both the control group and the ketamine group, indicating that the changes between groups were not significantly different, and the authors concluded that the administration of ketamine did not yield any beneficial effects on the postoperative inflammatory response. Therefore, high-quality studies in the future are necessary to verify whether ketamine has an anti-inflammatory effect as well as to prevent the incidence of POCD.
As the population ages, with an increase in the number of elderly patients undergoing surgical procedures, POCD in elderly patients needs more concern. 52 The mechanisms underlying POCD in the elderly are not yet fully understood. However, it is recognized that factors such as neuroinflammation, deposition of amyloid-β, and neuronal apoptosis play significant roles. 53 Recent studies have suggested that the higher incidence of POCD in the elderly may be partially due to a significant decrease in the volume fraction of astrocytes connected through gap junctions and peri-synaptic processes, 54 as well as SIRT1 expression declines in hippocampal microglia and promote tau acetylation, resulting in age-associated neuroinflammation and cognitive impairment.55,56 We conducted a subgroup analysis of the six included studies using age (>60 years old) as a criterion and found no advantage of intraoperative ketamine/esketamine in preventing POCD in older patients. These findings are consistent with previous research.24,25 However, there are also clinical studies that show no advantages in preventing the development of POCD in elderly patients treated with ketamine.32,34 For future studies, it is crucial to provide more high-quality evidence to further investigate the effect of ketamine on POCD.
Limitation
This study has limitations. First, the absence of a uniform definition/cut-offs about the diagnosis of POCD currently, and different diagnostic methods for POCD used in the included studies may lead to heterogeneity in results. Second, although some studies concluded that there were no significant differences between ketamine and esketamine in the treatment of cognitive function in TRD patients, there is still a lack of high-quality evidence reported on whether there is heterogeneity in the effects of ketamine and esketamine on POCD in normal patients. In addition, the included original studies excluded patients with preoperative cognitive dysfunction and patients with severe disease (ASA IV–V) because there is no enough evidence to support the protective effect of ketamine/esketamine on POCD, and there are even studies that suggest that ketamine increases the occurrence of POCD. In contrast, patients with preoperative cognitive dysfunction as well as critically ill patients usually need to undergo more complex treatments, and the safety risk of using ketamine/esketamine in such patients may be even greater. Future studies should address limitations and contribute to a better understanding of the pathogenic mechanisms and prevention strategies for POCD.
Conclusion
Our results do not support an effect of intraoperative subanesthetic dose of ketamine/esketamine having advantage compared with controls in preventing POCD in patients, or in elderly patients. We hope to learn more details about the involvement of ketamine/esketamine in the pathogenesis of POCD to help identify new targets for disease intervention. This study provides reference data for POCD research and clinical drug intervention strategies in patients.