
Abstract
The evidence for the risks associated with anticholinergic agents has grown considerably in the last two decades. Not only are they associated with causing peripheral side effects such as dry mouth, blurred vision and constipation, but they can also cause central effects such as cognitive impairment; and more recently, they have consistently been linked with an increased risk of dementia and death in older people. This paper reviews the evidence for the associations of anticholinergic agents and the risk of dementia and increased mortality in dementia.
Keywords
Introduction
Acetylcholine was first synthesized in 1867, and several decades later it was shown to be an extremely potent physiological depressor, quoted to be ‘a hundred times more active in causing a fall of blood pressure than is adrenaline in causing a rise’.1,2 Sir Henry Dale, an English pharmacologist and physiologist, first discovered the neurotransmitter acetylcholine and its chemical transmission in nerve impulses in 1913. As with many ground-breaking medical discoveries, naturally occurring acetylcholine was first isolated as a rare contaminant in a batch of ergot, which was claimed to be a ‘lucky accident’ by Dale in later life. For this, Dale shared the 1936 Nobel Prize in Physiology or Medicine with Otto Loewi. 1
By the beginning of the 1930s, outstanding evidence suggested that acetylcholine was associated with the normal functioning of the autonomic nervous system. Dale and Otto Loewi had analysed and classified the effects of acetylcholine postulating its ability to mimic parasympathetic nervous stimulation and had provided strong, and replicable, evidence that a chemical substance, remarkably similar to acetylcholine, was released when the parasympathetic nerves were stimulated. These findings were further validated when it was shown that acetylcholine was a normal constituent of the mammalian body. Further experiments continued over the next few years suggesting that acetylcholine might act as a transmitter at both pre- and post-ganglionic sites in the parasympathetic nervous system, as well as at the voluntary neuromuscular junction. 3
Few medicines enhance the action of acetylcholine; these include medicines for dementia and myasthenia gravis. Most drugs affecting the cholinergic system act by blocking cholinergic receptors and thus the action of acetylcholine, and these are known as anticholinergic drugs.
Anticholinergic agents were originally derived from atropine-containing plants like deadly nightshade (Belladonna plant) and thorn apple. For many centuries, atropine-containing plants were burned and the smoke was inhaled and used to treat diseases that obstruct the airways. 4 In the 19th century, anticholinergic agents were introduced into medication for Parkinson’s disease and were the first form of treatment for this condition. 5
The dangers and mind-altering effects of atropine have been known for centuries. In fact, the name atropine, derived from ‘Atropos’, the Greek Goddess with the power to cut the thread of life, infers its deadly potential. It is not surprising that for decades, medical and pharmacy students have been taught that anticholinergic drug use should be minimized or avoided in older people. 6 Nevertheless, anticholinergic drugs are still widely prescribed for the management of various conditions, including mental, neurological, respiratory, and urological disorders and are prevalent in the older adult population, ranging from 11% to 80% of their medicines. 7
Over the last 25 years, the evidence for the risks associated with anticholinergic agents has grown considerably. Not only are they associated with causing peripheral side effects 8 such as dry mouth, blurred vision, and constipation, but they can also cause central effects such as cognitive impairment 9 ; and more recently, they have consistently been linked with an increased risk of dementia 10 and death 11 in older people. As a result, a nationwide drive was launched to reduce their use in older people, or at the very least, manage their use safely.
Anticholinergic side effects
Anticholinergic side effects can include both physical and mental impairment and can therefore be divided into two types: peripheral and central effects. It is vital that clinicians are attuned to the potential for these effects so that they can effectively and safely treat patients. Furthermore, there are potential medical complications of anticholinergic side effects, and in susceptible patients, particularly older people or those with pre-existing conditions, these side effects can be serious. 8
Typical peripheral side effects include dry mouth, decreased sweating, constipation, urinary retention, dilated pupils, blurred vision, and increased heart rate (see Table 1). While these effects may not raise immediate concern, clinicians should be wary as they can lead to a plethora of medical complications including bowel obstruction, hyperthermia and myocardial infarction. 8
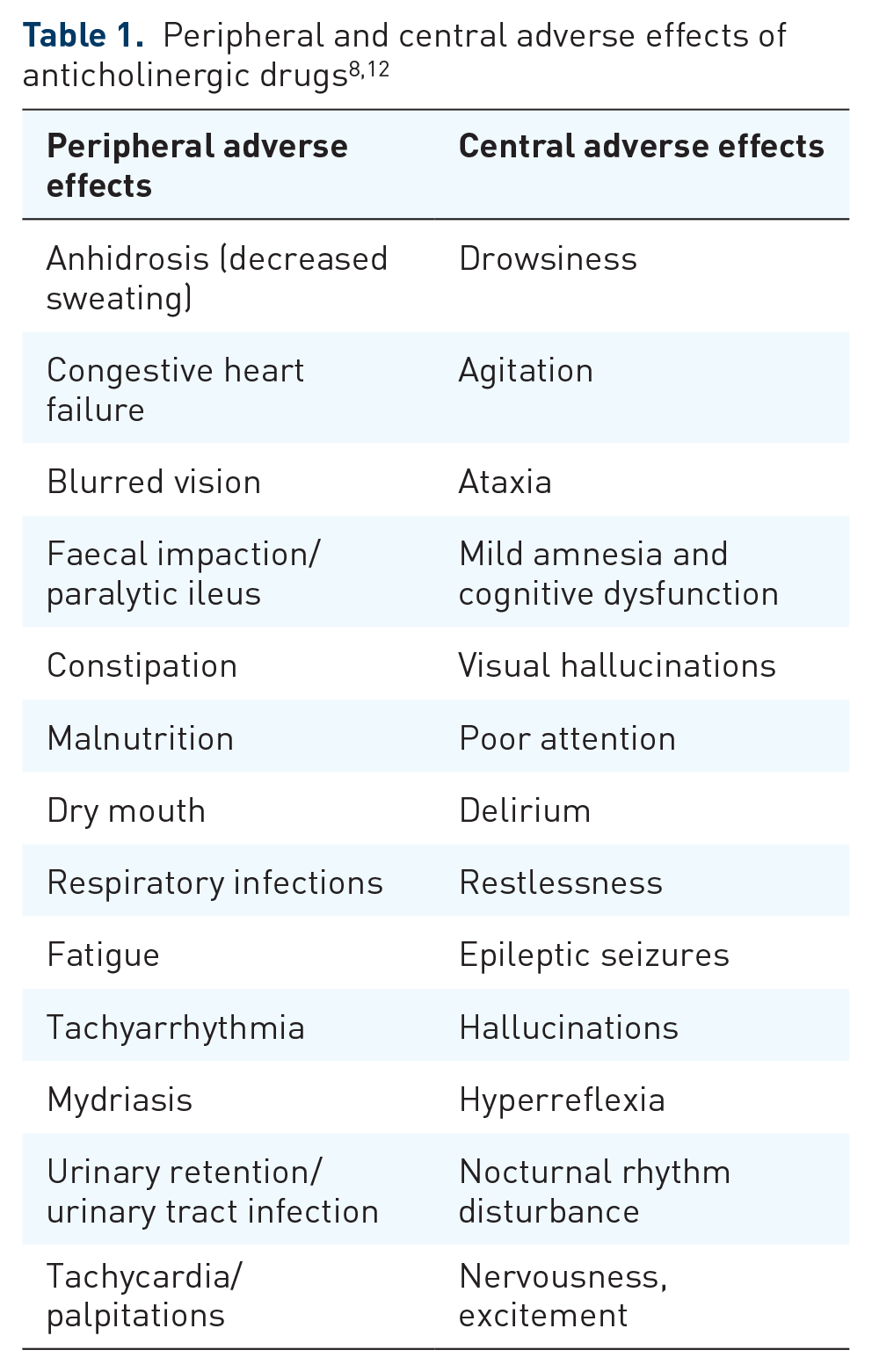
Central side effects associated with anticholinergic drugs include impaired concentration, confusion, attention deficit, memory impairment and delirium, 8 amongst others (see Table 1). It is not difficult to see why, when taken as a whole, anticholinergic side effects can seriously affect a patient’s function and have been shown to increase the risk of falls in older people. 13
Whether a drug penetrates the brain and acts centrally is determined by its physiochemical properties. A drug’s ability to cross the blood–brain barrier (BBB) is dictated by its polarity, molecular size, and lipophilicity. 14 In addition, only certain muscarinic receptor subtypes are located in the central nervous system (CNS). To our knowledge, five different muscarinic receptor subtypes exist (M1–M5). The muscarinic M1 receptors are most abundant in the CNS and expressed in all major forebrain areas including the cerebral cortex, hippocampus and striatum. Activation of muscarinic M1 receptors is implicated in learning and memory processes. 15 Muscarinic M2 receptors are widely expressed in both central and peripheral nervous systems. Selective M2 antagonism increases cholinergic overflow by reducing autoreceptor function in both the brain and periphery. Studies in mice deficient in both M2 and M4 receptors suggest a role for these subtypes in modulating hippocampal cholinergic function. Genetic variants in the human M2 receptor gene correspond with differences in cognitive performance. 15 Muscarinic M4 receptors are abundant in the neostriatum and are believed to affect the regulation of acetylcholine levels.16,17 Hence, cognitive impairment, especially memory dysfunction, can result from antagonism at M1, but also to some extent at M2 and M4 receptors in the CNS. 17 It is also believed that muscarinic M1 and M4 play a role in motor control.18,19 The M3 receptor is mainly responsible for bladder contraction, 14 but is also involved in smooth muscle contractility, exocrine gland secretion, pupil dilation as well as food intake and therefore weight gain. 18 Finally, muscarinic M5 receptors have been identified in various peripheral and cerebral blood vessels and are involved in the modulation of central dopamine function and the tone of cerebral blood vessels. 18 Hence, different drugs, even from within the same class, will vary in terms of their anticholinergic effects, as this will depend on their own individual physiochemical properties.
Anticholinergic burden of drugs and how to measure it
The anticholinergic burden is the cumulative effect on an individual when taking one or more medications with anticholinergic activity. It is not always obvious to clinicians which drugs will contribute to the anticholinergic burden. We know that some drugs are used specifically for their therapeutic effects on the anticholinergic system (e.g. procyclidine, used to manage extrapyramidal side effects caused by antipsychotic drugs and oxybutynin, used to treat symptoms of overactive bladder); however, others have anticholinergic effects that are secondary to their primary mode of action (e.g. tricyclic antidepressants). This example of secondary effect (or side effect) is generally well known amongst clinicians; however, other drugs may have anticholinergic side effects that are less widely known, for example, benzodiazepines or steroids and identifying the risk may therefore pose a challenge. To assist clinicians in identifying high-risk drugs and minimizing their use in older people, various anticholinergic risk scales have been produced usually consisting of a list of drugs, each with a classification of their anticholinergic potency. 20 The Anticholinergic Effect on Cognition Scale is different from the other scales as it can help clinicians to identify drugs specifically with high central anticholinergic burden and considers the individual drug’s physiological characteristics including its selectivity to specific muscarinic receptors, its CNS penetration and any reports of cognitive impairment. It can be accessed at: www.medichec.com. As such, drugs from the same class can be rated differently, thus providing a safer option to patients in terms of preserving cognitive function.
The evidence
While the side effects caused by anticholinergic agents have been known for over a century, new data emerged in the last 25 years on the long-term effects associated with anticholinergic drug use.
A 2-year longitudinal study of over 13,000 participants by Fox et al. 11 in 2011 found that the use of medication with definite anticholinergic effects was associated with a 0.33-point greater decline in Mini-Mental State Examination score and a 26% increased mortality rate. This study raised serious concerns and led to considerable research focused on this area.
Several large, well-conducted studies have consistently found an association between anticholinergic agents and an increased risk of dementia. This relationship was true for specific classes of drugs including antidepressants, antipsychotics, antiepileptics, antiparkinsonian and urological drugs.10,21,22 Similarly, a recent large prospective study, using the UK Biobank, 22 found that anticholinergic burden according to most anticholinergic scales was predictive of dementia. In addition, as with the previous studies, the association between anticholinergic burden and dementia also held true for certain classes of drugs, especially antidepressants, antiepileptics and antidiuretics.
Systematic reviews of the literature are consistent with these findings. One systematic review and meta-analysis deduced that anticholinergic use for ⩾3 months increased the risk of dementia on average by an estimated 46% versus non-users. 23 Another also identified a dose-dependent relationship between anticholinergic drugs and the risk of dementia. 7 Both these reviews highlighted specific drug classes as being problematic (antidepressants, antiparkinsonian and urological drugs). In contrast, Zheng et al. 7 noted that cardiovascular and gastrointestinal drugs appeared to play potentially protective roles. They concluded that these findings highlight the importance of anticholinergic drugs as a potential modifiable risk factor for dementia prevention. 7
There is a reasonable argument that these specific classes of drugs are used in conditions that are risk factors for dementia anyway (e.g. depression, Parkinson’s disease), and that therefore this is an example of potential bias by indication – that the drugs are not the cause of dementia but are simply being used for conditions that themselves predispose to dementia. However, both Welk, McArthur 24 and Matta et al. 25 addressed this bias using an equivalent, condition-specific, non-anticholinergic comparator group mirabegron, a selective beta-3-adrenoceptor agonist. Both studies found a higher risk of dementia in patients receiving anticholinergic drugs compared with those taking mirabegron. Matta et al.’s 25 study found that individuals with incident dementia were 29% more likely to have received any antimuscarinic for overactive bladder than mirabegron.
Furthermore, it appears that the use of oxybutynin, a non-selective centrally acting bladder anticholinergic satisfies the Bradford Hill criteria for establishing a causal link with the development of dementia, 26 and this may also be the case for other anticholinergics that easily cross the BBB.
Whilst beyond the scope of this paper, the mechanisms underpinning the cause of urinary incontinence are complex. Urinary incontinence can be caused by neurological conditions, mechanical damage, or the comorbidities of certain illnesses such as dementia, but it can also be drug induced. For instance, it is a well-known complication of antipsychotic drugs although the mechanisms by which they do this are not fully understood. It is thought that their anticholinergic action may be implicated, since causing urinary retention can lead to overflow incontinence. In addition, incontinence could be an secondary effect of extrapyramidal symptoms (EPSE) 27 or of sedation. 28 It has also been suggested that since α1-adrenergic receptors are widely distributed over the lower urinary tract, especially over the smooth muscle of the trigone and detrusor muscle of the bladder, and promote urinary continence, dopamino-serotoninergic effects along with peripheral α1-adrenergic blockade may act synergistically to cause urinary incontinence and/or urinary retention. 27 Hence, the cause of urinary incontinence may be multifactorial and involve several different pathways, not just the cholinergic pathway. Nevertheless, alternative options to anticholinergic agents are limited, and further research is needed to investigate these other mechanisms and develop new drugs targeting them.
Evidence also exists for the association between anticholinergic burden and poor outcomes in people with pre-existing dementia. Several large longitudinal retrospective studies have shown that a high anticholinergic burden is associated with increased mortality29–33 and hospitalization.30,31,34 To address protopathic bias, three separate studies focused on anticholinergic bladder drugs.32,35,36 This class of drugs includes receptor selective and non-selective drugs within the same group of agents used for the same condition which can occur in people with or without dementia. Hence, peripheral and central effects could be compared whilst reducing potential protopathic bias. All three studies found an increased mortality risk with bladder drugs with high anticholinergic burden. Two of the studies compared selective and non-selective agents and found that non-selective agents with the high central anticholinergic burden (oxybutynin, tolterodine) were associated with a 50% 35 and 55% 36 increased mortality risk than the more selective agents that do not penetrate the brain.
Antidepressants and antipsychotics were also examined separately to investigate their effects on outcomes in dementia. Studies found that the influence of anticholinergic burden did not increase mortality with antidepressants32,37 or antipsychotics 37 in people with dementia and if anything, a reverse association was found with antidepressants. 37 So contrary to expectation, tricyclic antidepressants were safer than antidepressants with low anticholinergic burden. Potential reasons for this are complex and numerous. Firstly, it is not surprising that antidepressants reduce mortality in depression; the evidence for this is established.38,39 Secondly, it is widely known that even antidepressants with a low anticholinergic burden such as selective serotonin reuptake inhibitors can increase mortality through other mechanisms, for example, gastrointestinal bleeds. 40 Finally, mirtazapine (which has a low anticholinergic burden) is often reserved for patients who are seriously ill or have contraindications to other antidepressants. It is very possible therefore that other properties of different antidepressants may influence the choice of prescribing and that the types of illnesses being treated with anticholinergics may also influence patient outcomes in dementia. Also, perhaps changes in prescribing habits had already occurred and high-risk drugs were avoided in vulnerable patients. 37 Of note, some antidepressants with low anticholinergic burden, for example, mirtazapine can cause some seemingly anticholinergic side effects such as constipation, but through other mechanisms. Mirtazapine acts as an antagonist at central presynaptic α2 adrenergic receptors, an action that results in an increase in central noradrenergic and serotonergic activity. Furthermore, mirtazapine is a potent histamine H1, serotonin 5-HT2 and 5-HT3 antagonist. Constipation could therefore result from its adrenergic rather than cholinergic action, or like most drugs, it may be a combination of different mechanisms at play.
The anticholinergic burden of antipsychotic drugs was also not found to be associated with increased mortality in dementia. 37 Reasons for this could be explained by the fact that complex processes are also involved when selecting an antipsychotic agent and that their action is also multimodal. For example, risperidone and haloperidol are antipsychotics with low central anticholinergic burden. Thus, the higher risks of antipsychotic drugs with low central anticholinergic burden could be attributed to these agents being used for behavioural and psychological symptoms of dementia (or delirium for haloperidol) and therefore reserved for patients with a more severe illness or stage of dementia. This could explain why antipsychotics with low central anticholinergic burden were found to be associated with higher mortality. 37
Of note, whilst the association between anticholinergic burden and constipation is not well defined, findings from a systematic review 41 suggest that a correlation between anticholinergic burden and constipation exists. The prevalence of constipation varies widely depending on gender, age, comorbidities, medication, lack of physical activity and poor diet and some estimates approach 50% among older adults over 80 years. 42 Constipation can reduce the quality of life, increase hospitalization and is a risk factor for faecal impaction. Consequences can be serious and substantial and are often underestimated. Case reports have identified bowel ulceration, perforation and death.41,42 Furthermore, laxative use can result in falls. 43
Anticholinergic drugs have been implicated in tardive dyskinesia (TD) for many years, and not without due cause. A recent expert panel of psychiatry and neurology clinicians agrees with current treatment guidelines that anticholinergics should not be used to treat TD as they do not improve and may worsen TD symptoms. The study findings were presented at Psych Congress 2022. Authors concluded that whilst anticholinergics may be considered for use among patients at high risk for acute dystonia, prolonged use should be avoided due to the potential long-term cognitive and peripheral adverse effects. The misuse of the classification ‘extrapyramidal symptoms’ contributes to patients continuing to receive incorrect therapies. ‘Extrapyramidal symptoms’ is an all-encompassing term for acute and tardive neuroleptic-induced movement disorders, which does not differentiate by presentation, pathophysiology or treatment. 44 The experts added that when discontinuing, anticholinergics should be tapered slowly since abrupt discontinuation may result in cholinergic rebound.
Finally, polypharmacy is very common in older people and its prevalence is increasing. It is associated with numerous adverse effects, hospitalization, falls and mortality.45,46 Polypharmacy predisposes to higher anticholinergic burden which may explain a proportion of the poor outcomes associated with it. 45
Conclusion
Research over the last two decades has provided us with compelling evidence that in most cases, anticholinergic agents are harmful in older people. A key challenge is to flag up at-risk patients to clinicians, and for clinicians to have the knowledge and available information at hand on which is the most effective and safe treatment for their patients. Often, it is a case of ‘if an anticholinergic agent is deemed necessary, consider the safest anticholinergic agent for that individual patient, and use it for the shortest time possible’. Many factors should be considered in terms of the specific action of each drug, its penetration into the CNS, potential adverse effects, interactions, etc. Recent evidence has substantiated concerns that some anticholinergic agents for example, non-selective, centrally acting ones may therefore be more harmful than others. Initiatives to change prescribing habits could become a key tool in reducing the risk of dementia and improving outcomes in people with dementia.