
Abstract
Background:
Partial adherence to antipsychotics is the most common cause of relapses and rehospitalization in patients with schizophrenia (SZ), leading to higher health care costs and psychosocial disability. The use of long-acting injectable (LAI) antipsychotics may improve therapeutic continuity and adherence to treatment.
Objective:
To assess the effectiveness of switching from oral antipsychotics (OAs) to long-acting antipsychotics.
Methods:
This 1-year mirror-image study evaluated the effect of switching from OAs to LAIs on the reduction of psychiatric hospitalizations and the improvement of global functioning in patients with schizophrenia. Differences in outcomes between second-generation (SGA) LAIs and first-generation (FGA) LAIs were also analyzed.
Results:
In all, 166 patients were included: 32.5% treated by FGA-LAIs and 67.5% by SGA-LAIs. There was an overall reduction of 71% in the average number of hospital admissions and an overall improvement of 29.3% in the Global Assessment of Functioning (GAF) score between the previous 12 months and the 12 months following the switching to LAIs. Patients who switched to SGA-LAIs had no significant differences in hospitalization occurrences but a significant improvement in GAF scores when compared with patients who switched to FGA-LAIs.
Conclusion:
Our results suggest that using LAIs could be the most adequate treatment choice for SZ patients with a high risk of relapse and low adherence rate. Patients with poorer social functioning may be ideal candidates for SGA-LAIs treatment. Our findings may be of particular interest from a clinical and health care management perspective.
Keywords
Introduction
Schizophrenia (SZ) is a severe, often recurring, mental disorder, adversely impairing daily activities, work productivity, and social functioning 1 and increasing financial burdens. 2
In Italy, the total economic impact of SZ is equal to €2,770,495,280 [95% confidence interval (CI) = €1771.93–€3988.65], of which 50.5% is due to indirect costs, while the remaining 49.5% is due to direct costs linked to the disease. 3 Drugs corresponded to 10% of direct costs and hospitalizations accounted for 81%. 3
Moreover, frequent rehospitalization in SZ is associated with poor long-term prognosis, psychosocial disability, and increased health care resource utilization and costs.4,5
Partial adherence to antipsychotics, which concerns at least 40–60% of SZ patients,6,7 is the most common cause of rehospitalization (about 40% of new hospital admissions) and the risk of relapses,8 –10 leading to higher health care costs.11 –13
One strategy to reduce non-adherence to oral medications in SZ has been the use of long-acting injectable (LAI) antipsychotics. Moreover, LAIs may improve therapeutic continuity facilitating regular contact between the physician and patient, reducing the, albeit rare, risk of overdose while maintaining a more stable level of medication in the blood and avoiding the bioavailability issues that occur with oral antipsychotics (OAs).14 –17 Finally, they can also help clinicians differentiate true treatment resistance to pseudo-resistance.
The latest meta-analysis of 21 randomized clinical trials (RCTs) with 5176 participants, 18 however, showed no superiority of LAIs in preventing relapse (risk ratio = 0.93) and hospitalizations (risk ratio = 0.89). Several limitations may contribute to explain this negative result: (a) RCTs might enroll a larger number of patients with better treatment adherence and cognitive capabilities and lower illness severity19,20 and selectively exclude non-seeking treatment patients, those who had treatment-resistant SZ, and other psychiatric and medical comorbidities; 21 (b) patients who were not willing to receive LAIs may have refused to participate to an RCT or are more likely to withdraw; 22 (c) participation in an RCT can alter the ecology of treatment delivery and experience, 19 that is, patients receive reminders, reimbursement, free medication, provision of transportation, and assessment of efficacy, safety, and even adherence. Patients are monitored much more frequently and closely in RCTs than in normal care settings. Thus, patients in RCTs are likely to receive much more and different types of attention than patients in routine clinical practice, and all of these differences may work to the disadvantage of LAIs when compared with OAs.20,23
Therefore, the standard RCT may not be the best strategy to examine the effectiveness of LAIs. 24 Indeed, pragmatic management of SZ is much more complex, and there is a need for naturalistic data to establish the real-world impact.16,23
Mirror-image studies, which involve collecting data with regard to a particular outcome over a specified time period before and after an event (e.g. after switching treatments) and where each patient serves as his or her own control, might better reflect the relative impact of LAIs versus OAs in the targeted population and in naturalistic settings and circumstances. 25 As LAIs are prescribed in priority to patients who are non-adherent to treatment and to those with greater severity of illness, 18 the populations in mirror-image studies better reflect the populations receiving LAIs in clinical practice as compared to those recruited in RCTs. In addition, mirror-image studies are conducted in a naturalistic context and, therefore, do not alter the ecology of the treatment delivery and experience.26,27
A large meta-analysis based on 25 mirror-image studies that followed 5940 SZ patients for ⩾12 months showed a strong superiority for LAIs over OAs in preventing hospitalization. 26 This result was confirmed in the review update, performed by the same authors in 2021 that analyze 32 mirror-image studies (8577 patients). 27
It is, however, possible that this difference may not be the same for all LAIs. If true, knowing which LAIs do present this difference is important, as this knowledge can be utilized to refine the treatment guidelines for SZ.
In this 1-year mirror-image study, our primary goal is to evaluate the effectiveness (i.e. efficacy under ordinary circumstances) in a sample of patients with SZ [Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)], who needed to switch from OAs to LAIs in real-life conditions, by considering naturalistic outcome measures, that is, means of psychiatric hospitalizations, and Global Assessment of Functioning (GAF).
Our next goals are to delineate the differences in outcomes between second-generation (SGA) LAIs and first-generation (FGA) LAIs. To obtain real-life measures, patients had to be treated in three community mental health centers and in one University mental health center (located in a hospital).
Methods
Study design
We conducted a naturalistic, retrospective, 1-year mirror-image study in three community mental health centers and one University mental health center located in a hospital in Turin. Mental health care in Italy is delivered by the National Health Service through the Departments of Mental Health (DMH). In each catchment area, one or more central mental health centers (CMHCs) provide outpatient care, day care, and rehabilitation to nearly 100,000 inhabitants.
Being a retrospective study, in accordance with our Ethics Committee (Comitato Etico Interaziendale AOU Città della Salute e della Scienza di Torino – AO Ordine Mauriziano – ASL Città di Torino), patients were not required to provide informed consent. All the patients whose data were collected had previously signed the informed consent, present in the medical record, to the processing of personal data and the use of the data for research purposes. Given the naturalistic design of the study, the results remained purely observational, and the researchers did not influence the results in any way. The study was conducted in accordance with the Declaration of Helsinki.
We chose this study design as it is inexpensive, can be conducted within a reasonably short period of time, and allows for a ‘real-world’ analysis of the variables under scrutiny, as it does not follow the more strict rigors of an RCT. The intervention under scrutiny in this study was the commencement of LAI in the management of SZ. The outcomes under scrutiny were the number of admissions to a psychiatric ward and GAF scores before and after commencing LAI.
Study sample
SZ patients were selected into the study from the electronic records of the mental health centers and the University mental health center (located in a hospital) if they were initiated to LAI from 2015 to 2020, were 18 years of age or older at the time of initiation, have continued to take LAI for at least 1 year, and had 1 year of data both before and after the initial LAI. Drug abuse and comorbidities were allowed. We defined the initiation of LAI based on a floating date approach (i.e. patients received the first prescription of LAI at any time during the period of interest, provided that they were not on LAI during the 12 months prior to initiation). The initiation dates (index date), which tended to vary across patients, were used as a cutoff point in defining pre- and post-initiation periods. More specifically, the pre-LAI period included the 12 months prior to the initiation date; whereas, the post-LAI period included the 12 months following the initiation date. The index date or mirror point was defined as the date of the first LAI prescription. ‘Pre-index date’ was defined as the period before the initiation of LAI prescription, while ‘post-index date’ stood for the period after the initiation of LAI prescription.
They were excluded if complete data were not available for any reason, such as illegible medical records, hospital transfer, or loss to follow-up.
Data collection
Clinical and sociodemographic variables, including age on the index date, sex, marital status, living and educational status, age of illness onset, duration of illness, family history of mental illness, type of LAI antipsychotic treatment (in particular FGA-LAI or SGA-LAI), GAF score, and number of psychiatric hospitalizations in the 12-month ‘pre’ and ‘post’ index date, were obtained retrospectively from the medical notes of the local information system for University mental health center (located in a hospital) records and the local databases of mental health centers. All GAF assessments were performed by the patients’ clinicians, as a part of their clinical routine. In an attempt to reduce inter-rater variability, all clinicians were usually trained to administer GAF and other psychometric tools according to the common standards when they started working in the mental health centers or in the University mental health center of our department. Also, once a year, psychopathological rater training is usually performed regularly to establish a high inter-rater reliability when clinicians administer GAF or other psychometric tools.
The primary outcome indexes of the study for 1 year before initiation to 1 year after initiation of LAIs were (a) GAF and (b) the number of psychiatric hospital admissions. To perform a cost-consequence analysis, all psychiatric hospital admissions were included, that is, scheduled hospital admissions and involuntary hospital admission from any discontinuation of treatment.
GAF is used because it provides a broader picture of functioning, including the impact of symptomatology and social and professional functioning, and because it is easy to administer by clinicians. Its 1–100 scoring allows for a finer discrimination than other global scores with a limited range.
Psychopharmacological treatment
Being a naturalistic study, there were no specific guidelines for treatments, so patients received the antipsychotic treatment, co-medications, and treatment changes based on the clinician’s choice. Dosing, co-medications, or treatment changes were based on clinical necessity. Being a retrospective data collection, patients included did not lead a different patient care that deviated from the regular treatment and were not required to provide informed consent.
In the University mental health center, patients were generally treated according to the American Psychiatry Association guidelines, 28 whereas patients in mental health centers were generally treated according to the National Institute for Health and Care Excellence (NICE) guidelines. 29
Statistical analysis
This mirror-image study compares outcomes before and after the index date. The mirror-image study design, which uses participants as their own controls, can control for all time-invariant measured and unmeasured confounders.
Descriptive statistics included the mean, standard deviation (SD) in continuous data, and the frequencies and percentages in discrete data. The normal distribution of the data was evaluated with the Kolmogorov–Smirnov test.
Like in the traditional mirror-image models, GAF scores and number of psychiatric admissions in the 12 months before and after the mirror points were compared for the entire cohort, as well as SGA-LAIs and FGA-LAIs groups using paired t tests, because the distribution of data regarding pre and the LAI periods was normal. We then calculated differences in the change in GAF scores and psychiatric admissions between the two groups (SGA-LAIs and FGA-LAIs) using one-way repeated-measures analysis of covariance (ANCOVA), which allows controlling for sampling bias (GAF scores and admissions before mirror points).
Risk of hospitalization for the entire cohort was computed as the number of patients hospitalized divided by the number of patients at risk. The risk ratio was then given by the ratio of risks for LAIs versus OAs.
Rate of hospitalizations was computed as the number of hospitalizations divided by the person-years at risk. The rate ratio was then given by the ratio of rates for LAIs versus OAs.
The rates of readmissions between the two groups were compared using a chi-square test.
Finally, we conducted multiple linear regressions with the change in GAF scores or hospitalizations between before and after the mirror points as the dependent variable.
A p value of ⩽0.05 was considered statistically significant.
Adjusted R 2 of the two final models was calculated.
Statistical analyses were conducted using Statistical Package for the Social Sciences, SPSS, version 25 for Windows (SPSS, Chicago, IL, USA).
Results
Two researchers analyzed the electronic records of databases of three community mental health centers and one University mental health center (located in a hospital) looking for SZ patients who were switched to a LAI in the period’s study (2015–2020) and who had 1 year of data both before and after the initial LAI. They identified 274 SZ patients who were switched to a LAI between 2015 and 2020 and who continued LAI treatment for almost 1 year; however, 108 of them were not included in our analysis because complete data on the outcomes were not available for any reason. This happened because their clinicians did not complete the database correctly or because patients moved to another community mental health center that used another database and did not rate GAF.
For the comparison between study subjects (N = 166) and excluding subjects (N = 108), sex, age, and duration of illness were not statistically different.
The final sample included 166 patients: 54 treated by FGA-LAIs (32.53%) and 112 by SGA-LAIs (67.47%). Of these, 54 were treated with Haloperidol-LAI, 16 with Risperidone-LAI, 12 with Paliperidone three-monthly, 70 with Paliperidone one-monthly, and 14 with Aripiprazole-LAI one-monthly.
The demographic and clinical characteristics of the sample are listed in Table 1.
Patient demographics.

CI, confidence intervals at 95%; FGA, first-generation; LAI, long-acting injectable; LOI, length of illness; SD, standard deviation; SGA, second-generation.
Mean GAF score increased significantly in the 12 months after commencing LAIs compared with the prior equivalent period in the entire cohort (Table 2). For the number of admissions in the 12 months before and after the mirror points, there was a statistically significant reduction for the entire cohort and both the SGA-LAIs and the FGA-LAIs groups (Table 2).
GAF and admissions in the 12 months before and after the mirror points.

FGA, first-generation; GAF, Global Assessment of Functioning; LAI, long-acting injectable; SGA, second-generation.
As compared with the pre-LAIs period, the total annual number of acute admissions was reduced by 71% (0.76 versus 0.21). These findings translated into a mean reduction of 0.55 admissions [standard error (SE) = 0.86], meaning that for every 100 patients who initiated LAI, there were 55 fewer hospitalizations. Moreover, it was recorded as a mean increase of 15.69 (SE = 1.11) in GAF scores from the 12 months before to the 12 months after the mirror points. Thus, the total GAF score increased by 29.3% (53.30 versus 68.99) in the 1-year post-LAI period with statistical significance (Table 3).
Change in GAF and hospitalizations among people with FGA-LAI and SGA-LAI.

One-way ANCOVA. ANCOVA, analysis of covariance; FGA, first-generation; GAF, Global Assessment of Functioning; LAI, long-acting injectable; SE, standard error; SGA, second-generation.
F = 170.68, 1 degree of freedom, p < 0.001, η 2 = 0.51.
F = 0.187, 1 degree of freedom, p = 0.666, η 2 = 0.001.
Controlling for GAF score as a covariate in the 12 months before commencing LAI, people who switched to SGA-LAIs gained 19.61 points on GAF scores (SE = 0.66) after the mirror point compared with before (Table 3), a significantly greater difference when compared with people who switched to FGA-LAIs (7.55 increase of GAF score, F = 170.681, SE = 1.07, p < 0.001; η 2 = 0.512) (Table 3).
As regards the number of admissions, those who were administered FGA-LAIs had 0.79 fewer occurrences of hospitalizations (SE = 1.08), a no significantly greater difference when compared with people who switched to SGA-LAIs (0.43 fewer hospitalizations, SE = 0.30), even while controlling for admissions as a covariate in the 12 months before commencing LAI. The combined F statistic was 0.187, 1 degree of freedom, p = 0.666, η 2 = 0.001.
In the entire cohort, LAIs showed strong superiority over OAs in preventing hospitalization (risk ratio = 0.26) and in decreasing the number of hospitalizations (rate ratio = 0.24).
The rate of readmission was higher for the FGA-LAIs group (16.7%), with no statistical difference with the SGA-LAIs group (13.4%) (p = 0.574, χ2 = 0.32).
For the change in GAF score before and after the mirror points, occupation (β = –0.19, t = –2.40, p = 0.018), medical comorbidity (β = –0.18, t = –2.32, p = 0.022), and SGAs’ treatment (β = 0.47, t = 6.32, p < 0.001) were significantly associated in the multiple linear regressions. All other variables had no effect (adjusted R 2 = 0.41).
Only treatment (SGA-LAIs/FGA-LAIs) (β = –0.26, t = –2.87, p = 0.047) and marital status (beta = –0.20, t = –2.12, p = 0.036) were significantly associated with a reduction in the number of admissions before and after the mirror points (adjusted R 2 = 0.08).
Discussion
This large naturalistic mirror study investigated the impact of LAI commencement on subsequent psychiatric hospitalizations and global functioning. Psychiatric hospitalizations were selected as outcomes of interest as they are typically considered as proxies for episodes of SZ relapse, which in turn are associated with impaired functioning, reduced quality of life, and potential harm to oneself or others.30 –34
First, our major finding is that LAIs led to an improvement in global functioning and a substantial reduction in frequency of psychiatric admissions that were maintained over a 12-month period following the initiation of LAIs (Figure 1).
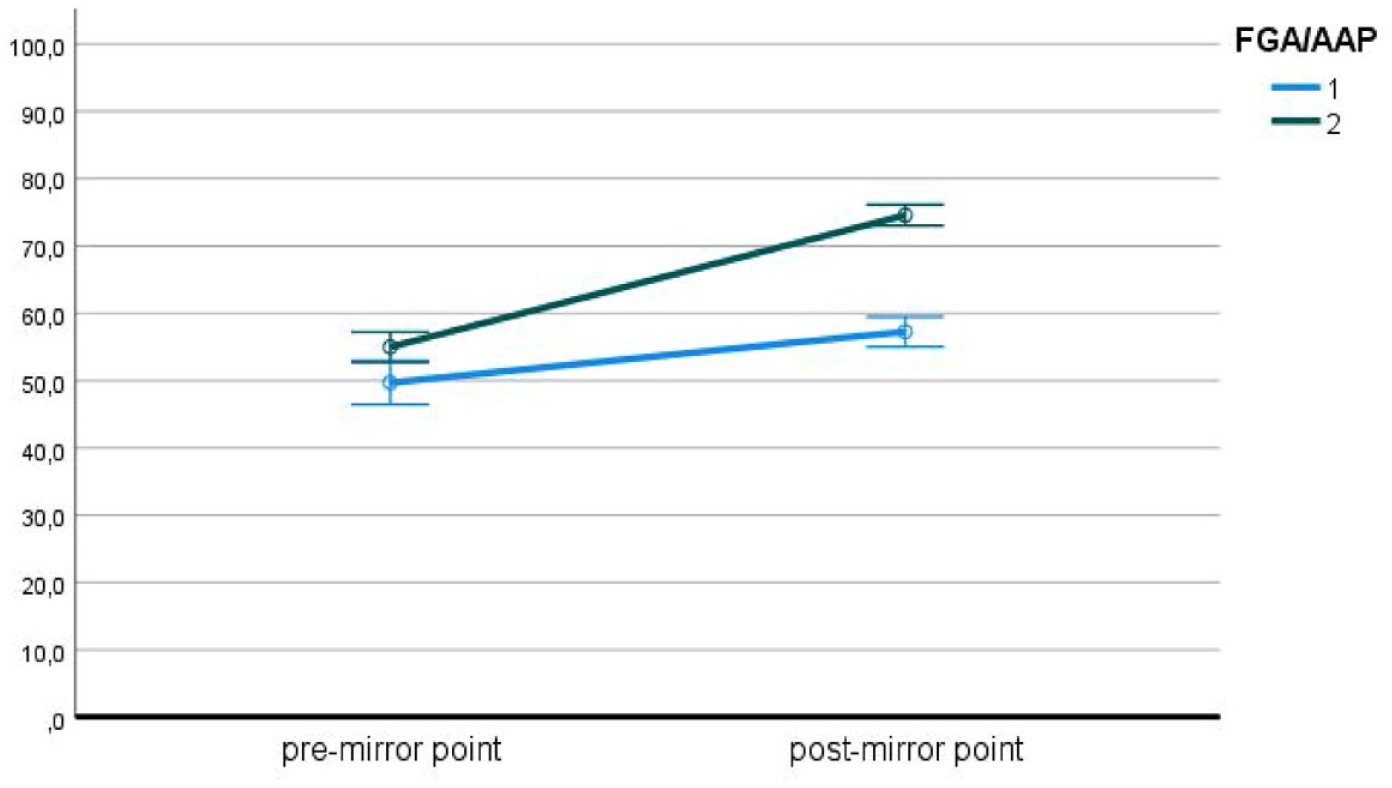
Mean GAF scores before and after LAIs (bars represent standard error).
Patients who continued for 12 months demonstrated an overall reduction of 71% in the mean number of hospital admissions compared with the 12-month period before initiation and demonstrated an overall improvement of 29.3% in the GAF score (Figure 2).

Mean psychiatric hospitalizations before and after LAI (bars represent standard error).
Sex, age, schooling, and duration of psychotic illness before LAIs initiation, however, were not associated with either outcome. This suggests that commencing LAIs can still have a benefit both on the risk for acute psychiatric hospitalization and on global functioning, irrespective of how late in the course of the illness they were started.
Previous studies demonstrated up to 20–30% reduced risk of hospital readmission during LAIs treatment compared with the equivalent oral formulations35 –37 and a 5% lower risk of rehospitalization at 60 days in the LAI group compared with OAs. 38
The reduced risk/rate of hospitalization in this article is consistent with the results of previous literature reviews and meta-analyses based on real-world data in which a mirror-image analysis was performed, 24 which showed a significant decrease in hospitalization after patients switched to LAIs. Particularly strong evidence was reported in a Spanish 10-year mirror-image study conducted in more than 300 patients that linked LAI administration with significant reductions in number of hospitalized patients and number of hospitalizations due to relapse. 39
Second, SGA-LAIs treatment was associated with greater improvement of global functioning as compared with FGA-LAIs treatment.
The question of which LAI should be the first choice remains uncertain. 40 The comparative effectiveness of expensive SGA-LAIs versus cheaper FGA-LAIs is an important and largely unexamined question.
Systematic reviews between SGA-LAIs and FGA-LAIs have focused on mortality risk 41 or discontinuation rates. 42
A more recent systematic review and meta-analysis focused on efficacy and safety found only three trials (n = 459) with direct comparisons of SGA-LAIs versus FGA-LAIs, two of them on psychiatric hospitalizations, concluding for no significant differences between them. 40
In a 12-month open-label rater-blinded RCT, number of hospitalizations were not significantly different between patients (n = 54) receiving LAI-risperidone (31 mg mean monthly dose) and those receiving haloperidol-LAI (114 mg mean monthly dose) or fluphenazine decanoate (37 mg mean monthly dosage) in 54 patients. 43 A largest double-blind RCT (n = 290) found no significant differences at 24 months in psychiatric hospitalization for paliperidone palmitate (149 mg mean monthly dosage) compared to haloperidol decanoate (75 mg mean monthly dosage). 44
A recent study performed by D’Agostino and colleagues 45 aimed to identify predictors of FGA-LAI or SGA-LAI choice in everyday clinical practice and found that FGA-LAIs were generally privileged in case of hostility, whereas SGA-LAIs are generally preferred in patients with more severe thought disturbances, but it confirmed that the rest of the literature on this topic is poor and sometimes conflicting.
The finding of no evidence for a difference in readmission rates between patients treated with FGA-LAIs and SGA-LAIs would suggest that there is no advantage in terms of maintaining response in choosing either an FGA-LAI versus an SGA-LAI, and prescriber choice should, therefore, be guided by other factors such as side-effect profile, patient acceptability, and costs. 46
In addition to the type of treatment, being married was also associated with fewer hospitalizations. From the available data, it is not possible to assess the impact of other types of social networks (family caregivers or social assistants support); we had only data on marital status. The SGA-LAI group did not show a statistically significant difference compared with the FGA-LAI group as regards marital status. Therefore, it can be assumed that the protective power of having a partner on the risk of hospitalization is more likely attributable to social support factors and to the help in following the therapeutic project. Evidence in literature is mixed regarding the ‘protective’ role of marital status. Some studies have found that being married is usually associated with a better quality of life and protects against suicidal ideation in middle-aged and older individuals with SZ or schizoaffective disorder and depressive symptoms, probably because having a partner is associated with less interpersonal problems, 47 stronger social integration, 48 and increased social support. 49 On the other hand, other authors have found strong support that in cohabiting couples, partner’s psychiatric morbidity associates with incidence of psychiatric disorders in healthy partners at baseline 50 because of assortative mating (i.e. mate selection based on finding a mate that is phenotypically similar to oneself), secondary assortment (i.e. mate selection based on traits which correlate with psychiatric morbidity, such as age, education, and employment status), and social homogamy (i.e. correlated geographic or social environments).51 –53
We have also found that patients treated with SGA-LAIs, however, obtained greater improvement in global functioning, a finding that has not been explored in head-to-head studies and that we considered as a substitute for clinical improvement in mental state.
The study had some strengths. First, the within-subjects design helped to minimize the impact of individual-level confounders on the number of inpatient admissions by effectively comparing the patient against themselves. There is no ‘perfect’ method for evaluating the effect of LAIs: RCTs inevitably recruit broadly compliant subjects who are not representative of LAIs patients in practice and observational studies are open to numerous biases.37,54 We have attempted to increase the generalizability of our results by analyzing patients from two different parts of our department (University hospital mental health center and mental health centers). We did not evaluate all health care costs (out-patient visits, home visits, etc.), but these are usually miniscule in comparison with the cost of hospitalization. 55 Second, we utilized naturalistic data acquired from clinical practice. Third, the informed consent was not required as the data were retrieved from pseudonymized databases. This eliminated the selection bias in favor of higher functioning patients that often taints research on treatment-resistant psychosis.
That said, the results of this study must be analyzed bearing in mind a number of limitations.
The major limitations of this study are inherently linked to its method: the retrospective and naturalistic design of this study. 56 The lack of a comparator group is a potential disadvantage, and we cannot say that LAIs are better, or worse, than any other OAs with certainty, that is, our results may reflect background variations occurring irrespective of the treatment received. All patients consecutively starting treatment with LAIs, however, were recruited to the study in an effort to minimize selection bias. Also, in a mirror-image study, each patient serves as his or her own control, and observed changes from pre- to post-LAIs introduction may reflect regression to the mean. 57 Moreover, there are further biases in mirror-image studies, such as expectation biases, natural illness course, and time-effect. 25
Second, possible confounders that may affect results or some other factors that can be related to readmission risks like cognitive deficits, adverse effects, and reasons for discontinuation and follow-up with outpatient were not included in our analysis. 58 Other factors that may affect the utilization of LAI like physician’s choice, costs, and type of clinical settings were not included which may confound our study results. We, however, included comorbidities, which makes our results representative of real-world clinical settings. Third, the study data were dependent on the quality, detail, and timing of data entry into the clinical records. While the dates and times of hard endpoints such as admission and death are likely to be accurate, discontinuation of medication is more prone to error because of differences in clinical record keeping and so may have been underestimated. The use of inpatient admissions and global functioning as markers or proxies of the overall mental health and the clinical improvement in mental state may be imprecise. This may, however, partly be accounted for with a mirror-image design. In addition, selection of LAI was down to individual clinician choice, and so may have been a source of bias, as paliperidone LAI has been found to be the most prescribed SGA-LAI. 46
Fourth, data on medication dosage or treatment adherence (for OAs) were not evaluated. Moreover, possible drug-drug interactions were not analyzed.
Fifth, owing to the nature of this study, we could not focus on the patients’ perspective or whether there was a specific component or components that yielded the positive outcome. 57
Finally, it may be argued that the change in services during the time frame covered by our study could have influenced our results. 57
Implications
In conclusion, we have shown that LAIs commencement is associated with a greater reduction in the number of psychiatric hospitalizations and greater improvement in global functioning, in a real-world sample treated in a mental health department in the northwestern Italy. 59 In this perspective, real-world findings may furnish data closer to routinely clinical practice,60,61 despite the bias related to their naturalistic no randomized nature. Both the improvement in global functioning and the reduction in psychiatric hospitalizations appear to be independent of the duration or severity of illness.
These results suggest how taking advantage of LAIs could be the most adequate treatment choice in SZ patients with high risk of relapse and low adherence rate. Moreover, we also found that SGA-LAIs with respect to OAs significantly increase global functioning in SZ. Thus, physicians should prefer SGA-LAIs to achieve specific treatment goals, such as improving functioning levels and occupational skills.62,63
Despite their potential advantages, LAIs continue to be underutilized, most notably in early disease stages, during which use could reduce the risk of poor outcomes associated with medication non-adherence.34,64 –68
Hospitalizations may be of particular interest from a clinical and economic perspective.31,32,69 –73 Recent studies agree on reporting significantly lower hospitalization-related expenses and mental health–related costs after initiation of LAI when compared with OAs in individuals with SZ.74,75 Even if LAIs are more expensive than OAs, their use may result in a decrease in the health care–related financial burden because of fewer hospitalizations.76 –84