
Abstract
Background:
A prolonged electrocardiogram (ECG) QT interval is associated with cardiac events and increased mortality. Antipsychotics can prolong the QT interval. The QT interval requires correction (QTc) for heart rate using a formula or QT-nomogram. The QT and QTc can be calculated automatically by the ECG machine or manually; however, machine-measured QT(c) intervals may be inaccurate.
Objective:
We aimed to investigate the mean QTc and proportion of prolonged QTc intervals in people taking antipsychotic medicines.
Methods:
We conducted an observational retrospective chart review and data analysis of all consecutive patients taking antipsychotics, with an ECG record, admitted to the psychiatric unit of a large tertiary hospital in Brisbane, Australia, between 1 January 2017 and 30 January 2019. We investigated the mean QTc of people taking antipsychotics to determine differences using (a) machine versus manual QT interval measurement and (b) QTc correction formulae (Bazett, Fridericia, Framingham, Hodges and Rautaharju) and the QT-nomogram. We also determined the number of people with a prolonged QTc using different methods and compared rates of prolonged QTc with antipsychotic monotherapy and polypharmacy.
Results:
Of 920 included people, the mean (±SD) machine-measured, Bazett-corrected QT interval (recorded from the ECG) was 435 ms (±27), significantly longer (p < 0.001) than the mean manually measured corrected QT intervals with Fridericia 394 ms (±24), Framingham 395 ms (±22), Hodges 398 ms (±22) and Rautaharju 400 ms (±24) formulae. There were significantly more people with a prolonged QTc using machine-measured QT and the Bazett formula (12.0%, 110/920) when compared with manually measured QT and the Fridericia formula (2.2%, 20/920) or QT-nomogram (0.7%, 6/920). Rates of QTc prolongation did not differ between people taking antipsychotic polypharmacy compared with monotherapy.
Conclusion:
Machine-measured QTc using the Bazett formula overestimates the QTc interval length and number of people with a prolonged QTc, compared with other formulae and the QT-nomogram. We recommend manually measuring the QT and correcting with the Fridericia formula or QT-nomogram prior to modifying antipsychotic therapies.
Background
People with severe mental illness (SMI) live with a high burden of excess morbidity and mortality. 1 Cardiovascular disease is the largest cause of 20-year reduction in lifespan among people with SMI. 2 This is likely due to sedentary lifestyle, as well as metabolic dysregulation and weight gain associated with SMI and antipsychotic medicines.3–6 Antipsychotic medicines are a mainstay in treating people with schizophrenia and other psychotic disorders as they are highly effective in attenuating positive symptoms, preventing relapse and reducing the risk of death in both acute and long-term settings.7–9 However, antipsychotic medicines are associated with adverse events, including a prolonged QT interval. 9
The QT interval represents the time taken for the ventricles to depolarise and repolarise. On an electrocardiogram (ECG), it is the interval from the beginning of the QRS complex to the end of the T wave. 10 A prolonged QT interval can lead to ventricular tachycardia (VT) and arrhythmias. 11 Polymorphic VT with a twisting of QRS complexes (around the isoelectric line) is known as Torsades de Pointes (TdP). 12 It is often self-limiting but in some cases it progresses to ventricular fibrillation and sudden cardiac death. 13
Other classical features of TdP include a short-long-short R-R cycle which may disturb even repolarisation across the myocardial wall. There also tend to be longer (i.e. cycle length) first beats in VT than the subsequent arrhythmia complexes: a warm-up phenomenon. 13
Antipsychotic medicines have been associated with sudden cardiac death, potentially due to an increased risk of TdP. 14 TdP may develop due to a delay in the net repolarising current via blocking of the Ik channel in cardiac myocytes (by the drug), 11 which can prolong the QT interval 13 and reactivate L-type calcium channels leading to early after depolarisations (EAD). 15 Since there are regional differences (of myocardial tissue) in action potential length, heterogeneous transmural repolarisation can create functional re-entrant pathways leading to the development of ventricular fibrillation and TdP, resulting in faintness, syncope and death.11,13,16
Derangements of serum potassium, calcium and magnesium and other electrolytes are known to contribute to arrhythmias.17,18 Second-generation antipsychotics are associated with electrolyte disturbances such as hyponatraemia and hypokalaemia, although the mechanism remains unclear.19–22 Along with (female) sex and age, other factors such as bradycardia, alcohol intake and illicit substance use are risk factors for a prolonged QT interval.23,24
There are two main limitations for accurately measuring the QT interval and assessing the risk of complications in clinical practice. First, many ECG machines routinely used in hospitals measure the distance from an ancillary line drawn from the peak of the T wave to an overestimated inflection point 25 which may be imprecise.26,27 ECG machines can have trouble defining the end of T waves, especially when they have morphological variations (e.g. inversions, biphasic, flattened) or lie close to the U wave.28–30 Since T and U wave fusion is subtle, it is the interpreter’s responsibility to recognise the abnormality; often times this means selecting leads not showing U waves. 31 It has also been shown that automatic QT measurement by the (ECG) machine has high reproducibility and avoids variability inherent with measurement by different clinicians. 32 Confirming the machine-measured QT interval by manually measuring and calculating the median value of six leads is a more accurate way to measure the QT interval.28,33,34 The American Heart Association recommends using the lead showing the longest QT interval. 31
Second, the QT interval is dependent on the heart rate and must be corrected using a formula (QTc). 35 The Bazett formula was the first one developed (1920) and is the most commonly used correction formula. 36 However, the Bazett formula is known to overcorrect the QT interval at tachycardic heart rates (>100 bpm) and undercorrect at bradycardic heart rates (<60 bpm).37–41 Many ECG machines use the Bazett formula for correction as the default.
Tachycardia is a common adverse effect of many antipsychotic medicines with α1-adrenergic and muscarinic receptor antagonism. 42 The widespread use of the Bazett formula has led to overestimating rates of QTc prolongation in people taking antipsychotic medicines and complicates the ability to assess the risk of cardiac events in people with antipsychotic-induced tachycardia. Global clinical guidelines suggest that the risk of TdP starts to increase with QTc values >470 ms for women and >440 ms for men, and the causative medicines should be ceased for QTc intervals >500 ms. 9 In addition, the Food and Drug Administration (FDA) has determined that 30 ms changes to the baseline QTc are clinically noteworthy, with increases of 60 ms potentially justify treatment discontinuation. 43 Several prospective antipsychotics were abandoned in the predevelopment phase because of prolonged QTc.12,44 In clinical practice, effective antipsychotic medicines may be needlessly withdrawn due to falsely elevated QTc measurements.
Other formulae have been developed including the Fridericia, Framingham, Hodges and Rautaharju formulae (Supplementary Figure 1). 35 Fossa et al. 45 developed a QT-cloud diagram which consists of QT-HR [heart rate (bpm)] plots of a population; any QT-HR pairs outside the 95% ‘normal’ range are associated with an increased risk of arrhythmia and TdP. A nomogram was subsequently developed to assist clinicians in assessing the risk of TdP in clinical settings and has a reported sensitivity of 96.9%. 37
We aimed to determine any differences in the mean QTc interval measurements and the number of people estimated to have a prolonged QTc between (a) machine versus manual measurement methods; (b) the Bazett, Fridericia, Framingham, Hodges and Rautaharju formulae and the QT-nomogram; and (c) antipsychotic monotherapy versus polypharmacy.
Method
Study design
We conducted an observational retrospective audit of each unique person admitted to the mental health unit of a large metropolitan hospital in Brisbane, Australia, over 25 months (1 January 2017 to 31 January 2019). We included 920 people who received an antipsychotic medicine at any point in their admission, had an ECG performed and were not acutely intoxicated on illicit substances.
Protocol
We extracted data from the local electronic medical record (EMR) on regular antipsychotic and non-antipsychotic QT-prolonging medicines 46 (Supplementary Tables 1 and 2) for each person, including any ‘when required’ antipsychotic doses given 48 h prior to the ECG (i.e. as 24-h equivalent doses). People who did not have a dose of antipsychotic prior to the ECG recording (but did receive one later in their admission) were thus categorised into the ‘no therapy’ group. We calculated the olanzapine-equivalent dose for each antipsychotic using the defined daily dose (DDD) method. 47 The QT interval was extracted from ECG leads (see below) as were serum electrolyte concentrations (if they were available within two days from the ECG) of potassium, corrected calcium, and magnesium from the EMR. We excluded any person that was non-adherent to their prescribed antipsychotic medicine, those who were documented to be acutely intoxicated with illicit substances and people who did not have a practitioner-confirmed ECG.
ECG and heart rate measurement
The Philips PageWriter TC50 ECG machine report was used to tabulate the machine-measured QT and QTc (Bazett) interval, along with the heart rate. The QT interval estimation technique within PageWriter TC50 uses an ancillary line from the peak of the T wave to a point beyond the expected inflection point at the end of the T wave. 25 The machine had a resolution of 800 × 600 SVGA, 8000 Hz sampling rate and a standard paper speed of 25 mm/s. 48 We manually measured the QT interval in six ECG leads from a standard 12-lead electrode. The most well-defined leads were chosen from the chest (3) and limbs (3).28,33,34 Leads showing U waves were avoided. To reduce inter-rater variability, one researcher (T.A.) measured all intervals and was trained by a clinical toxicologist (K.I.). A Bland–Altman plot testing for intra-rater variability suggested there was no proportional bias between two occasions of measurement (p = 0.670). We measured the QT interval from the beginning of the QRS complex to the end of the T wave using a magnifying electronic calliper function that was a feature of the EMR ECG recording. The end of the T wave was determined using the maximum slope technique. 49
We calculated the QTc interval using the median QT interval (from six leads) and the Bazett, Fridericia, Framingham, Hodges and Rautaharju formulae. The median QT interval is recommended as it provides a more robust measurement compared to the mean.28,33,34 The QT-HR pairs (using the median six-lead QT interval) were plotted on the QT-nomogram to determine whether the individual was at risk of TdP.
In clinical practice, any cases of QT prolongation should be assessed for QRS prolongation, as QT prolongation which is caused by QRS prolongation may have a different risk of TdP.
Statistical analysis
The mean population QTc intervals (ms) were calculated using the median six-lead QT interval (ms) that was individually corrected with the formulae (Bazett, Fridericia, Framingham, Hodges and Rautaharju). We determined whether there was a difference in the mean QTc interval calculated using the different formulae through sample paired T-tests using a significance level of ⍺ = 0.05. For analyses where multiple testing was undertaken, we used a significance of ⍺ = 0.01 to reduce the risk of a Type I error.
Through chi-square and sensitivity analyses, we determined whether there was a difference in the number of people with a prolonged QTc using the correction formulae. We also compared treatment groups (no therapy versus any therapy and monotherapy versus polypharmacy). We used the Fridericia formula for dichotomous analyses as it is more accurate for patients with tachycardia.40,50,51
Three sensitivity analyses were conducted. In the first sensitivity analysis, we excluded people with below-range electrolyte (potassium, magnesium and corrected calcium) derangements as they can contribute to QTc prolongation (Supplementary Tables 3 and 4).17,18 In the second sensitivity analysis, people who were taking non-antipsychotic QT-prolonging medicines (Supplementary Tables 5 and 6) were excluded. In the third sensitivity analysis, we compared no antipsychotic therapy groups to ‘high-risk’ monotherapy groups (i.e. people taking an antipsychotic medicine with a known risk of QT prolongation and TdP) 46 (Supplementary Table 7). We used SPSS version 27 (IBM) and GraphPad Prism 9 for statistical analyses.
Results
Of the 2025 unique persons identified, we excluded 1105 due to a non-confirmed ECG, non-adherence to medicines or acute illicit substance intoxication; 920 people were included.
The median age was 39 years [interquartile range (IQR): 29–51 years] and 59.2% were male (Table 1). The mean heart rate was 83 bpm [± standard deviation (SD): 16 bpm] [range: 32–149 bpm], with 5.3% of people with a heart rate <60 bpm (bradycardic) and 14.8% with a heart rate >100 bpm (tachycardic). Two in three people (66.2%) had all three serum electrolytes recorded within two days of their ECG. Most electrolyte levels recorded were normal (potassium: 95.6%, albumin corrected calcium: 99.0%, magnesium: 96.0%); the most common deviation were values below normal range.
Baseline characteristics of study population (n = 920).

IQR, interquartile range; SD, standard deviation.
Four in five people (81.5%) were taking at least one antipsychotic at the time of the ECG; the most commonly used were olanzapine (42.3%), quetiapine (16.1%) and risperidone (16.0%) (Supplementary Table 1). The median olanzapine-equivalent dose of antipsychotics was 10 mg (IQR: 2.5–20 mg) per day. There were 26.7% (246/920) of people taking medicines other than antipsychotics that have been reported to prolong the QTc. The most commonly prescribed non-antipsychotic QT-prolonging drugs were mirtazapine (7.3%), lithium (6.5%) and venlafaxine (4.9%) (Supplementary Table 2), all of which have limited evidence for risk of TdP. 46
QTc calculation using formulae
The mean machine-measured QT interval recorded from the ECG and corrected using the Bazett formula was 435 ms (± SD 27, Figure 1). The mean manually measured corrected QT intervals were Bazett 415 ms (± SD 26); Fridericia 394 ms (± SD 24); Framingham 395 ms (± SD 22); Hodges 398 ms (± SD 22); and Rautaharju 400 ms (± SD 24, Figure 1). The mean QTc interval using the Bazett formula (either machine or manually measured) was significantly greater than all other formulae (p < 0.001); however, the manually measured QT interval was not statistically different at ⍺ = 0.01 from the machine-measured QT interval when both were adjusted using the Bazett formula (Table 2).
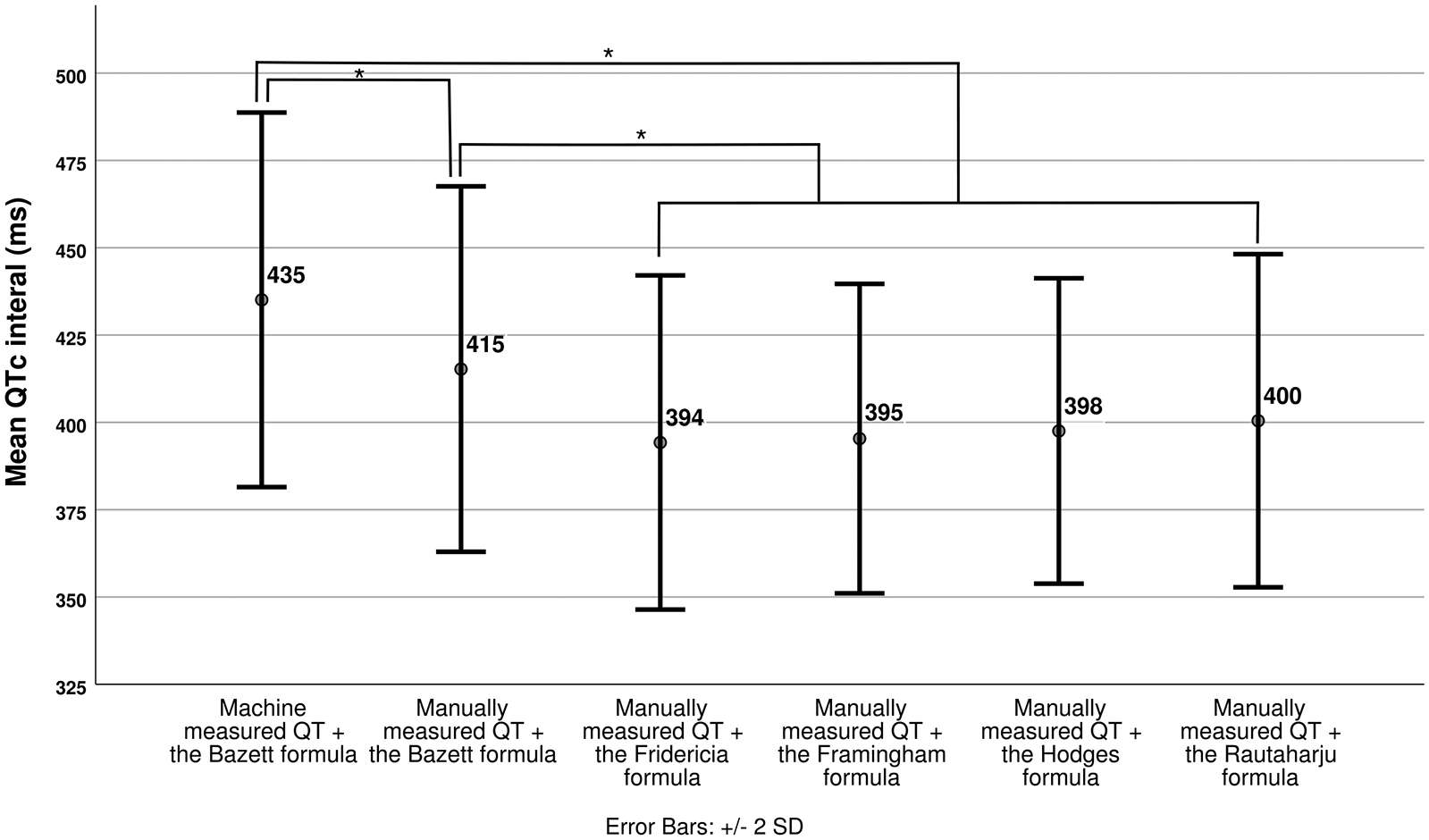
Mean corrected QT intervals (ms) obtained using various formulae. Machine-measured QT is the interval read from the ECG machine. Sample paired t-tests were conducted to calculate the p values.
Proportion of population identified as having a prolonged QTc using various calculation methods.

Alternative calculation methods, using standard cut-offs [>440 ms (M), >470 ms (F)], were compared to Machine-measured QT + the Bazett formula. Machine-measured QT + the Bazett formula was also compared to manually measured QT + the Bazett formula using a severe cut-off [>500 ms]. Chi-square analysis was used to calculate p values.
Fails to meet statistical significance with ⍺ = 0.01.
The number of people with a prolonged QTc was significantly greater using machine-measured QT with the Bazett formula compared with manually measured QT with the Bazett formula (12.0% versus 8.8%, p = 0.027). Only 2.2% were identified with a prolonged QTc using the Fridericia formula; significantly less than with the machine-measured Bazett correction (p < 0.001). Less than one in a hundred (0.7%) were at risk of TdP using the QT-nomogram; the lowest proportion of all the calculation methods.
When we excluded people with below-range electrolyte derangements, there remained significantly fewer people identified as having a prolonged QTc with manually measured QT corrected with the Fridericia formula or the QT-nomogram than with machine-measured QT corrected with the Bazett formula (Supplementary Table 3). The same trend was seen when we excluded people taking non-antipsychotic QT-prolonging medicines (Supplementary Table 5).
We also compared no antipsychotic therapy to ‘high-risk’ antipsychotic monotherapy (i.e. monotherapy with antipsychotic medicines known to prolong the QT interval and increase TdP risk). There was no difference (p = 0.361) in the rate of QTc prolongation between the groups using an alternative calculation method (i.e. manually measured QT and the Fridericia formula) (Supplementary Table 7).
Of all the formulae, only the Bazett formula identified any people with severe QTc prolongation [i.e. QTc >500 ms (severe threshold)]. There were fivefold more people above the severe threshold using the machine-measured QT interval (2.0%, 18/920) than the manually measured QT interval (0.4%, 4/920, p = 0.004). This trend (i.e. p < 0.05) remained even after excluding people with below-range electrolyte levels or people taking non-antipsychotic QT-prolonging medicines (Supplementary Tables 3 and 5).
The Bazett formula also appeared to underestimate rates of QTc prolongation in people with bradycardia. Two people who were below the prolonged QTc thresholds were identified as at risk of TdP using the QT-nomogram (Supplementary Figure 2).
Comparison of treatment regimes
There were no differences in the proportion of people with a prolonged QTc interval receiving either antipsychotic monotherapy or polypharmacy when measured using the various formulae (with machine and manual QT measurement) and the QT-nomogram (Table 3). There was also no difference in the proportion of people with a prolonged QTc receiving no therapy or any therapy when a manually measured QT interval and the Fridericia formula or QT-nomogram were used (Table 3). There was, however, a significantly higher (p < 0.001) proportion of people with a prolonged QTc when comparing no antipsychotic to any antipsychotic therapy when using a machine-measured QT interval and the Bazett formula. There was no difference in trend among treatment regimens when we excluded people with below-range electrolyte levels or people taking non-antipsychotic QT-prolonging medicines (Supplementary Tables 4 and 6).
Proportion of population from a treatment type identified as having a prolonged QTc using various calculation methods.
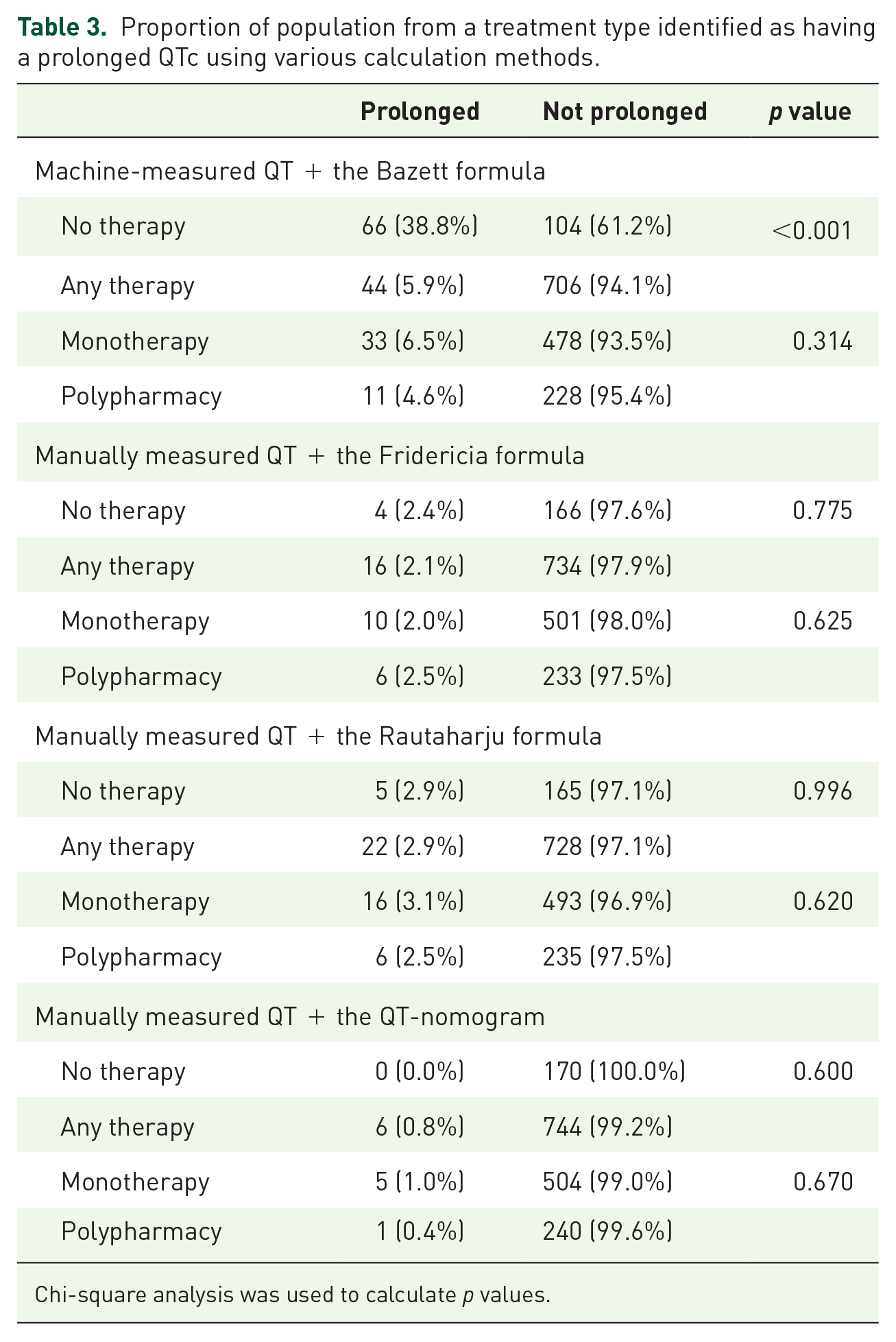
Chi-square analysis was used to calculate p values.
Discussion
Machine-measured QT intervals and correction of the QT using the Bazett formula significantly overestimates the absolute QT interval length. This method may result in misclassification among people taking antipsychotic medicines who are at risk. We only detected severe prolongation (QTc >500 ms) using the Bazett formula. When using alternative calculation methods, there was no difference in the number of people with a prolonged QTc when we compared those taking antipsychotic monotherapy versus polypharmacy, those taking any antipsychotic therapy (monotherapy or polypharmacy) versus no antipsychotic therapy, nor those taking antipsychotic monotherapy with higher risk of prolonged QTc versus no antipsychotic therapy.
Of the 110 people identified as having prolonged QTc with machine-measured QT corrected with the Bazett formula, only 6 were considered at risk of TdP when QT was measured manually and plotted on the QT-nomogram. Furthermore, two people in bradycardic heart rate zones who were considered at risk of TdP using the QT-nomogram were not identified using the machine-measured [QT], Bazett-corrected QTc (Supplementary Figure 2).
The Bazett formula may overestimate QTc in people with tachycardia. This is less likely with the other formulae. Antipsychotic-induced tachycardia is a common occurrence in people with SMI. In this population sample, the higher rates of prolonged QTc with the Bazett formula are likely due to overestimation secondary to antipsychotic-induced tachycardia. Concerningly, the Bazett formula may underestimate QTc in people with bradycardia, thus failing to identify people at higher risk of TdP.
Study strengths and limitations
To our knowledge, this is the first study to systematically explore both assessment of the QT interval and the impact of different formulae on identifying people with a prolonged QTc from a ‘real world’ clinical cohort of patients with SMI taking antipsychotic medicines. Only a few studies have explored QTc values in people taking antipsychotic and concomitant non-antipsychotic agents which may prolong the QT interval. These studies had smaller sample sizes (111–495 people)5,11,52 and did not evaluate assessment methods.
We performed a sensitivity analysis excluding people taking non-antipsychotic QT-prolonging medicines which did not affect the significance of the results. The Bazett formula still identified significantly more people with a prolonged QTc compared to the Fridericia formula or QT-nomogram. Including people taking non-antipsychotic QT-prolonging medicines in our study portrays a more pragmatic, real-world estimate of the risk of QTc prolongation as there is common concomitant use of these agents as an adjunct to antipsychotic treatment. 9
Some limitations are worth noting. Given the low incidence of QTc prolongation, there is the risk that analyses may have been insufficiently powered to disprove the null hypothesis. Second, some of our study population may not have reached steady-state plasma concentrations of antipsychotic at the time of the ECG; this might underestimate the risk of QT prolongation. Furthermore, the sample size prevented us from undertaking meaningful sub-analysis by individual antipsychotic when comparing antipsychotic polypharmacy and monotherapy. We were unable to ascertain whether people had electronic pacemakers which could widen the QT interval,53,54 but we estimate the proportion of patients with pacemakers would be very low in our study population. Finally, this study did not consider the effect of non-psychotropic medicines (e.g. certain antibiotics, antihistamines) that can prolong the QTc interval.46,55
Comparison to other literature
Our findings on the clinical limitations of current QTc interval measurement methods are consistent with other studies.26,28–30,37–40 Patel et al.’s 51 study included a large (6723) multihospital tachycardic population from the University of Pennsylvania Health System without atrial fibrillation or flutter, who had an ECG recorded at an encounter with a practitioner but were not specifically receiving antipsychotic medicines. They detected QTc prolongation in 39.0% of people using the Bazett formula, 6.2% using the Fridericia formula, 3.7% using the Framingham formula and 8.7% using the Hodges formula. 51 More than 2000 additional people with a prolonged QTc were identified using the Bazett formula compared with other formulae. Luo et al.’s 50 large (10,303) observational study also reported that the Bazett formula produced significantly higher QTc values than other formulae in a group with predominantly normal sinus rhythm, but, like for Patel et al., 51 this study did not examine people taking antipsychotic medicines. It should be acknowledged that these studies used predominantly normal ECGs from structurally sound hearts. In reality, the risk of TdP is higher in non-normal populations (e.g. heart failure, bradycardia, left ventricular hypertrophy).56,57
So which formulae should be used instead of the Bazett formula? Many authors recommend correcting QT using the Hodges formula,40,50,51 with Patel et al.’s 51 study suggesting it was the only formula shown to identify tachycardic individuals at higher risk of all-cause mortality. 51 Vandenberk et al.’s 58 work is the most extensive study (n = 49,737) comparing performance of QT correction formulae and the association with mortality. It found that the Fridericia formula had the best regression slope in all heart rate ranges and had a superior prediction of mortality (versus the Bazett formula). 58 Therefore, we would advocate for the use of the Friderica formula. The QT-nomogram is highly sensitive and specific (96.9% and 98.7%, respectively) and has a superior prediction of TdP across all heart rate zones compared to the Bazett formula. 37
We found no difference in the number of people with a prolonged QTc between those taking antipsychotic monotherapy versus polypharmacy; this contrasts with other studies.59,60 Barbui et al.’s findings of an association between antipsychotic polypharmacy and QTc interval prolongation were based on a narrow range of (7) antipsychotics, 57.1% of which had evidence supporting that they prolong the QT interval (compared to 36.8% in our study).46,60 However, it should be noted that this study assessed the risk of QTc prolongation using machine-measured QT and the Bazett formula. Furthermore, the mean antipsychotic dose was significantly higher for the polypharmacy group and the authors mention this as the main driving factor behind the small increase in QTc observed (7 ms). It is therefore likely that the increased incidence of QTc prolongation was simply due to increased rates of tachycardia. Although we found increased rates of prolonged QTc in people taking ‘high-risk’ antipsychotics when using machine-measured QT and the Bazzet formula, we did not see this when using manual QT measurement and an alternative formula.
Other authors have suggested there is no meaningful additional QTc prolongation when more than one QTc-prolonging medicine is used which is in keeping with our results.61,62 Our study may have not been sufficiently large enough to detect a difference and is limited by the varied antipsychotics and doses used in the monotherapy and polypharmacy cohort.
Implications and recommendations
Our study suggests that machine-measured QT, corrected using the Bazett formula, significantly overestimates the QT interval length and may result in misclassification among people taking antipsychotic medicines. Consequently, people may have effective medicines inappropriately altered or ceased, increasing the chances of relapse and an unfavourable disease trajectory for those with SMI. For people with heart rates >60 bpm, a formula which more accurately accounts for drug-induced tachycardia such as the Fridericia formula is recommended. For people with heart rates <60 bpm, the QT-nomogram may be used. Future studies investigating the rates of QT prolongation should avoid the use of the Bazett formula.
In clinical scenarios, we suggest using a stepwise approach (Table 4) before any changes are made to antipsychotic treatment or management. We also urge medical supply companies who distribute ECG machines to provide options for correction formulae to minimise the clinical load of manual measurement.
Approach to further examining machine calculated QTc.

ECG, electrocardiogram.
Current dispensing and prescribing software often alerts and recommends against using combinations of antipsychotics. Conversely, our results support previous literature that suggests combinations of antipsychotics may not lead to clinically or statistically significant increases in the number of people with a prolonged QTc. We would still caution against prescribing antipsychotic polypharmacy for reasons such as tablet burden or, most notably, side effect burden, including additional metabolic or extrapyramidal adverse effects. 63
Conclusion
Machine measurement of the QT interval and correction with the Bazett formula overestimates the QTc when compared with other formulae and the QT-nomogram. There was no increased incidence of prolonged QTc in persons taking antipsychotic polypharmacy compared to monotherapy.
As clinical guidelines typically suggest the cessation of causative drugs, 9 accurate measurement of the QT interval prevents unnecessary withdrawal of effective therapy and risk of relapse and deterioration in mental state. Clinicians should manually measure the QT interval and use a method which accurately accounts for drug-induced heart rate changes such as the Fridericia formula or QT-nomogram prior to making any decisions to cease an antipsychotic.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253221104947 – Supplemental material for Estimation of cardiac QTc intervals in people prescribed antipsychotics: a comparison of correction factors
Supplemental material, sj-docx-1-tpp-10.1177_20451253221104947 for Estimation of cardiac QTc intervals in people prescribed antipsychotics: a comparison of correction factors by Teodora Andric, Karl Winckel, Timothy David Tanzer, Samantha Hollingworth, Lesley Smith, Katherine Isoardi, Olivier Tan and Dan Siskind in Therapeutic Advances in Psychopharmacology
Footnotes
Ethics approval and consent to participate
This study analysed deidentified, routinely collected administrative data which did not require patient consent according to local legislation. Ethical approval was obtained from the Metro South Human Research Ethics Committee (HREC/2020/QMS/69685)
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DS is supported in part by an NHMRC EL2 Fellowship GNT1194635.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.