
Abstract
Background and objective:
Amitriptyline, a frequently used tricyclic antidepressant agent, has powerful cardiotoxic effects especially in high doses. Serum and urine levels of amitriptyline dosages are not correlated with severity of toxicity; therefore, it increases the importance of electrocardiography (ECG) abnormalities. The prolongation of QTc can be a predictive marker for cardiotoxicity. Hence, in this study, it is aimed to evaluate possible effects of metoprolol and diltiazem in amitriptyline toxicity.
Materials and methods:
The rats were separated into four groups. First one was control group, the second was the amitriptyline + saline group, third one was the amitriptyline + metoprolol group, and forth one was the amitriptyline + diltiazem group. ECG were recorded on rats under anesthesia.
Results:
In amitriptyline group, QTc duration was prolonged compared with all other groups. The prolongation of QTc was shorter in amitriptyline + metoprolol group and amitriptyline + diltiazem group than amitriptyline group (p < 0.01 and p < 0.01, respectively).
Conclusion:
According to the results, it is possible to report ameliorating effects of both metoprolol and diltiazem on QTc prolongation related with amitriptyline intoxication. With further studies, these agents may be used for amitriptyline toxicity and besides, they may be used for patients in cardiovascular risk groups who take amitriptyline treatment regularly.
Introduction
Tricyclic antidepressants (TCAs) are commonly used antidepressant agents. Thus, it is very broad on self-poisoning. In total 12,234 cases of TCA toxicity were reported in 2004 by American Association of Poison Control Centers and 61% of them was toxicity of amitriptyline. 1 TCA toxicity, with high mortality and morbidity rate, is due to direct peripheral α-adrenergic blockage, inhibition of norepinephrine reuptake at nerve terminals, a membrane stabilizing or quinidine-like effect on the myocardium and anticholinergic action. 2 Myocardial sodium channel blockage, ventricular dysrhythmias, myocardial depression, and hypotension can be seen in cardiotoxicity of TCA. 3 Electrocardiography (ECG) can be used as a predictive marker on cardiac effects of TCA in emergency department (ER). 4 The widened QRS, QTc, and PR durations can be seen due to prolongations of cardiac action potential and refractory period and besides, delay of atrioventricular node (AVN) conduction. 5 The underlying cause is sodium channel blockage leading to TCA toxicity. The effects of TCA toxicity are not related with ingested dosage. 6 It increases the importance of ECG on diagnosis and early management in ER.
It is known that prolonged QTc is related with poor prognosis in TCA toxicity. 6,7 The prolongation of QT can be seen not only in toxic dosage but also in therapeutic dosages. QT interval is measured from the onset of Q wave and the end of T and it has to be corrected with heart rate. 8 Generally, Bazett’s equation is used for correction of prolongation of QT. 9 The risk factors for prolongation of QTc are female sex, advanced age, congenital QT syndrome, electrolyte imbalance such as hypokalemia, endocrine metabolic problems, and so on. 10 It is reported that prolonged QTc increases mortality in TCA toxicity with some diseases as coronary artery disease, syncope, and diabetes mellitus. 11
Diltiazem, a calcium channel blocker, is class IV antiarrhythmic agent in the Vaughan–Williams classification. When the AVN conduction rates are high, diltiazem decelerates AVN conduction and prolongs refractoriness. 12,13 Metoprolol, a β-blocker, is a class II antiarrhythmic agent. It affects through AVN such as diltiazem. 13 Both of these agents are used to control atrial and ventricular rates. 14 The cardiotoxic effect of TCAs as amitriptyline is powerful and it is a reason for high mortality rate. 4,15 Considering this high mortality rate of amitriptyline toxicities, early diagnosis and treatment are very important. The prevention of prolongation of QTc duration can decrease morbidity and mortality in early stages. In this study, it is aimed to show ECG changes and besides, to investigate possible effects of diltiazem and metoprolol in the experimental model of amitriptyline toxicity. To the best of our knowledge, it is the first study about this issue.
Materials and methods
Animals
Twenty-four adult male Wistar rats (220–240 g) were included in the study. All animals were kept under standard 12-h light/12-h dark cycle in a temperature-controlled (22 ± 2°C) environment with ad libitum access to rodent chow. The experimental protocol performed in the study was approved by the Institutional Animal Care and Ethics Committee of the Gaziosmanpasa University.
Experimental protocol
Rats were divided into four groups (n = 6). Group 1 (control group) rats were given intraperitoneally (i.p.) 1 ml/kg of saline and 1 ml/kg of tap water via orogastric tubes. Group 2 rats were given 100 mg/kg of oral amitriptyline (Laroxyl 25 mg, Roche, Switzerland) and 1 ml/kg of 0.9% sodium chloride saline i.p. Group 3 rats were given 100 mg/kg of the pharmaceutical form of oral amitriptyline (Laroxyl 25 mg, Roche) and 1 mg/kg metoprolol i.p. (Beloc 5 mg, Astra Zeneca, UK). Group 4 rats were given 100 mg/kg of the pharmaceutical form of oral amitriptyline (Laroxyl 25 mg, Roche) and 1 mg/kg diltiazem i.p. (Diltiazem ampul 25 mg, Mustafa Nevzat, Turkey). Tablets containing 25 mg amitriptyline (Laroxyl, Roche) were suspended in tap water to yield a concentration of 10 mg/ml. According to the weight of each rat, suspended drug solution was completed to 4 ml with tap water. The amitriptyline was given via orogastric tubes.
Assessment of ECG
ECGs were recorded on male Wistar rats under anesthesia in the prone position. Electrodes consisted of 26-gauge needles placed subcutaneously for 1 cm. Standard limb leads were constructed from electrodes placed at the paws. Rats were anesthetized by combination of ketamine hydrochloride at a dose of 40 mg/kg (Alfamine®, Ege Vet, Alfasan International B.V., Holland) and 4 mg/kg of xylazine hydrochloric (Alfazyne®, Ege Vet, Alfasan International B.V.) that were administered i.p. Under anesthesia, ketamine (40 mg/kg) and xylazine (4 mg/kg) were administered i.p., ECG was taken in derivation II (BIOPAC MP 150, Goleta, California, USA). Data were evaluated using Biopac Student Lab PRO Version 3.6.7 software (BIOPAC Systems, Inc.), QT interval, T wave duration, and beats per minute (BPM) as the parameters. For the calculation of QTc, Bazett’s formula was used. During the ECG recordings, rectal temperatures of the rats were monitored by a rectal probe (HP Viridia 24-C; Hewlett-Packard Company, Palo Alto, California, USA) and the temperature of each rat was kept at approximately 36–37°C by heating pad.
Statistical analysis
Data analyses were performed using Statistical Package for the Social Sciences Version 15.0 for Windows. The groups of parametric variables were compared by Student’s t test and analysis of variance. The groups of nonparametric variables were compared by Mann-Whitney U test. Shapiro-Wilk test was used for parametric–nonparametric differentiation. Results were given as mean ± standard error of mean. A value of p < 0.05 was accepted as statistically significant.
Results
ECGs of all the four groups are shown in Figure 1. Additionally in Table 1, QTc, BPM, QT duration, and T duration time are presented for all groups. Firstly, the effect of amitriptyline on rat hearts was investigated by ECG. QTc duration was prolonged compared with control group and it was statistically significant (p < 0.000). In amitriptyline group, BPM, QT, and T durations were found to be statistically longer than control group (p < 0.01, p < 0.01, and p < 0.000, respectively). QTc duration in amitriptyline + saline group was found to be longer than amitriptyline + metoprolol group (p < 0.000). Besides, QT and T durations were longer in amitriptyline + saline group than amitriptyline + metoprolol group (p < 0.01 and p < 0.000, respectively). There were statistically significant differences between amitriptyline + saline group and amitriptyline + diltiazem group for QTc and T durations. In amitriptyline + diltiazem group, QTc was found to be shorter than amitriptyline + saline group (p < 0.001). T duration was longer in amitriptyline + saline group than amitriptyline + diltiazem group (p < 0.00).
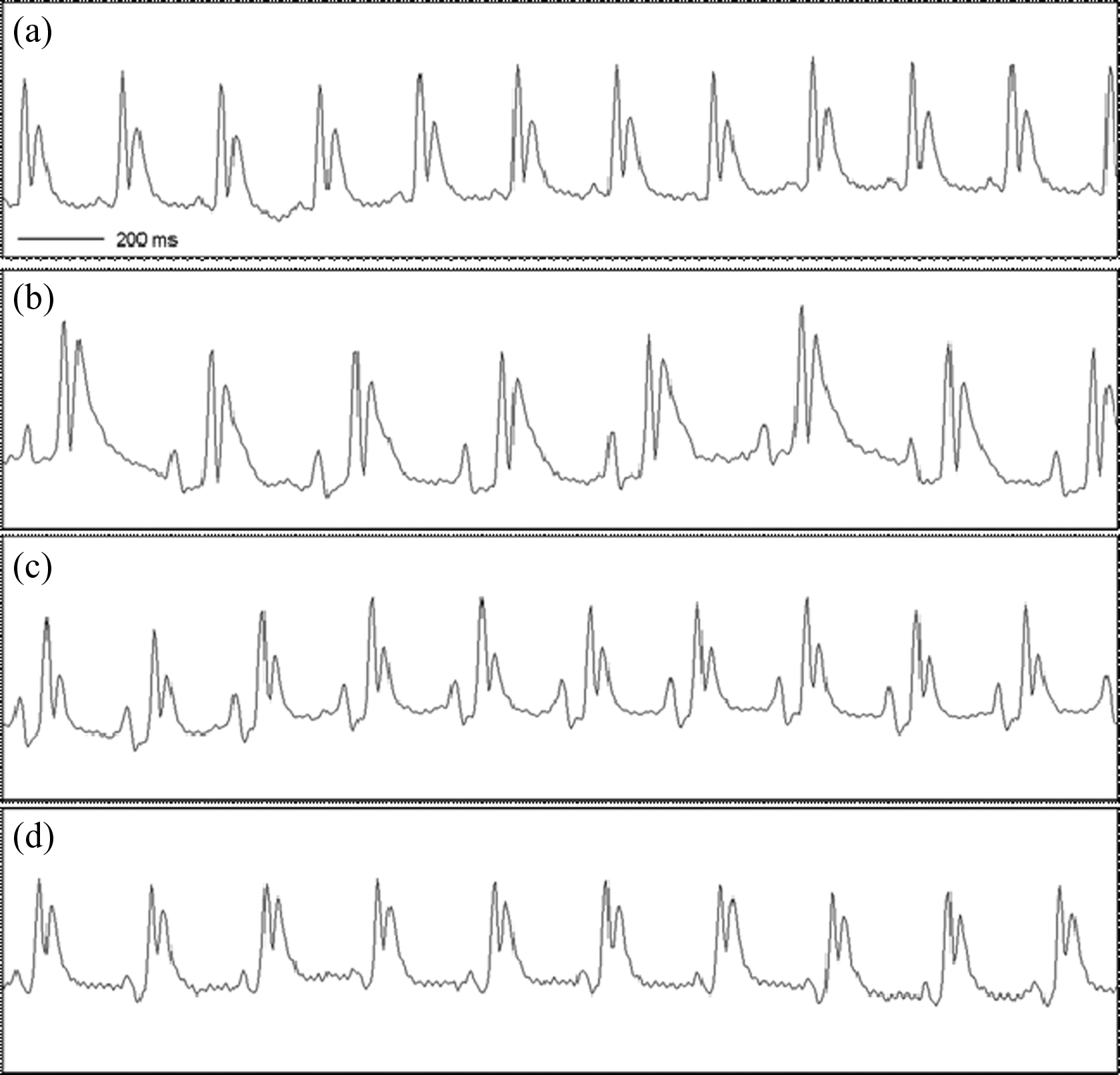
The electrocardiographies of all the four groups. (a) Electrocardiography of normal group (group 1); (b) electrocardiography of amitriptyline and izotonik saline (group 2); (c) electrocardiography of amitriptyline and metoprolol (group 3); and (d) electrocardiography of amitriptyline and diltiazem (group 4).
The QTc, QT, and T durations and BPM for all four groups.

BPM: beats per minute.
a p < 0.000 (compared with normal and isotonic saline).
b p < 0.01 (compared with normal and isotonic saline).
c p < 0.001 (compared with amitriptyline and izotonik saline).
d p < 0.05 (compared with amitriptyline and diltiazem).
e p < 0.01 (compared with amitriptyline and izotonik saline).
f p < 0.000 (compared with amitriptyline and izotonik saline).
When the effect of metoprolol and diltiazem was compared, it was found that QTc duration was shorter in amitriptyline + metoprolol group than amitriptyline + diltiazem group (p < 0.05). Additionally, in amitriptyline + metoprolol group, QT and T durations were shorter than amitriptyline + diltiazem group (p < 0.05).
Discussion
In the study, the ECG changes were presented in the experimental model of amitriptyline toxicity. It is known that cardiovascular toxicity due to TCA toxicities is the most common cause of death. 7 Additionally, it is manifested by ECG abnormalities and hypotension. 16 ECG abnormalities gain importance because arrhythmias and hypotension are late signs of cardiac toxicity. The severity of clinical findings doesn’t correlate with serum and also urine concentrations and it also increases the importance of ECG changes clinically. 17 In amitriptyline toxicity, the most common ECG abnormalities are prolongation of PR, QRS, and QT intervals due to sodium channel blockage, ST segment and T wave changes, right axis deviation, and Brugada pattern. 16 In this study, prolongation of QTc, QT, and T durations was determined in amitriptyline + saline group. Additionally, BPM was decreased compared with normal group. Similar to this study, Kalkan et al. reported that amitriptyline toxicity reduces heart rate, prolongs QRS and QT durations. 18 Inversely, in a study of Kaplan et al., it is suggested that amitriptyline has no effect on heart rate. 19
The prolongation of QTc is particularly important inside of ECG abnormalities. It is suggested that the most responsible mechanism for QTc prolongation is the slowing of depolarization of the cardiac action potential by inhibition of the sodium and also potassium channels. 20 It is known that elderly age, TCA, and higher antipsychotic doses were predictors of significant QTc prolongation. 21 In patients who have high risk for cardiac problems, cardiotoxicity may be seen not only in toxic dosage but also in therapeutic dosage of amitriptyline. 12,22 In a study of Balasubramaniyam et al., it is found that prolongation of QTc may be a sign of mortality in patients with diagnosis of syncope as coronary artery disease or diabetes mellitus that was previously reported. 11 Nose et al. reported prolongation of QTc in antidepressant usage and they suggest that for patients who are prescribed amitriptyline routine cardiac monitoring may be done. They indicated that especially in patients with other risk factors such as cardiovascular comorbidities are controlled routinely by cardiac monitoring and the drug combinations may be done carefully by considering the risk of QTc prolongation. 21
QTc prolongation has been associated with several drugs such as diphenhydramine, ondansetron, pimozide, ziprasidone, gemfibrozil, amiodarone, citalopram, clarithromycin, dofetilide, erythromycin, ketoconazole, methadone, ondansetron, haloperidol, pimozide, quetiapine, and TCAs. 11 The prolongation of QTc may cause lethal arrhythmias in amitriptyline toxicity. 23 Therefore, early recognition and treatment are very important. Despite the mechanism not being clear completely; in literature, there are some studies that tried some agents such as adenosine A1 receptor antagonist, theophylline, glucagon, lidocaine, or phenytoin and found good effects on cardiotoxicity of amitriptyline. 7,18,19,24
In this study, besides presentation of ECG abnormalities as particularly QTc prolongation, the effects of both metoprolol and diltiazem were investigated. According to the results, it is found that both of them shortened QTc and T duration prolongation. To the best of our knowledge, there is no study that investigates possible effects of metoprolol and diltiazem in amitriptyline toxicity. The treatment with β-blockers is considered in prolongation of QTc. It is known that different β-blockers have similar effects in prevention of cardiac functions. 25 Blockade of outward potassium currents may be a cause of prolongation of action potential. Thus, QT interval and T duration prolong. The drugs as amitriptyline that prolong QTc may be responsible from pro-arrhythmic effects by blockade of outward potassium currents. 26
It is known that metoprolol causes shortening in action potential due to decrease in inward calcium current and increase in outward potassium currents in myocardial cells. 27,28 Particularly, the increase in potassium outward from myocardial cells triggers shortening in action potential, QTc, and T durations. 26 Diltiazem causes shortening in action potential and QTc prolongation due to decrease in inward calcium current in myocardial cells. 29
In a study of Erbas, the effects of metoprolol and diltiazem on ziprasidone-induced rats were demonstrated. Ziprasidone is an antipsychotic agent and it can delay cardiac repolarization and potentially cause prolongation of the QT interval and T duration in ECG. Similar to this study, it is found that both metoprolol and diltiazem have good efficacy in the prevention of ziprasidone-induced prolongation in the QTc interval and T duration. Also, they suggest that both metoprolol and diltiazem may be used in the prophylactic therapy of high-risk patients who use antipsychotic drugs. 12 In this study, metoprolol was more effective than diltiazem on shortness of QTc prolongation in amitriptyline toxic rats. In a case of Baysal et al., a patient with amitriptyline toxicity treated with β-blocker agent is reported and they suggest that selective β-blockers may be used in severe amitriptyline toxicity with patients with no hypotension. In spite of the QTc duration, the amendatory effects of β-blocker on ECG changes are presented by ECG figures of the patient in that report. 30
Conclusion
In conclusion, amitriptyline has strong cardiotoxic effects and it presents ECG abnormalities such as prolongation of QTc duration. Prolongation of QTc duration due to increasing mortality caused by amitriptyline toxicity is very important. In this study, the beneficial effects of metoprolol and diltiazem were demonstrated for shortness of QTc prolongation-related amitriptyline intoxication. With further investigations including clinical studies, metoprolol and diltiazem may be used to ameliorate amitriptyline-induced cardiotoxicity. They can be used in patients in cardiac risk group who take amitriptyline treatment regularly.
Limitations
The blood samples that aim to evaluate cardiac biomarkers could not be worked in this study. It was aimed to evaluate cardiac efficacy on ECG findings.
Footnotes
Conflict of interests
I certify that:
1. All forms of financial support, including pharmaceutical company support, are acknowledged in the Contribution.
2. Any commercial or financial involvements that might present an appearance of a conflict of interest related to the Contribution are disclosed in the covering letter accompanying the Contribution and all such potential conflicts of interest will be discussed with the Editor as to whether disclosure of this information with the published Contribution is to be made in the Journal.
3. I have not signed an agreement with any sponsor of the research reported in the Contribution that prevents me from publishing both positive and negative results or that forbids me from publishing this research without the prior approval of the sponsor.
4. I have checked in the manuscript submission guidelines whether this Journal requires a Declaration of Conflicting Interests and complied with the requirements specified where such a policy exists.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.