
Abstract
Postpartum depression is one of the most common morbidities of childbearing, yet it is underdiagnosed and undertreated with negative consequences for mother and offspring. Despite the widespread use of standard-of-care antidepressants as the mainstay of treatment for postpartum depression, there is limited evidence on their safety and efficacy due to their slow onset of action and suboptimal outcomes. The emergence of gamma-aminobutyric acidergic neuroactive steroids may offer faster response and remission times and improved patient outcomes. This article reviews the evidence base for the efficacy of standard-of-care antidepressants, hormonal therapeutics including progestins and estradiol, and gamma-aminobutyric acidergic neuroactive steroids in the treatment of postpartum depression, as well as the safety of infant exposure to these agents during lactation.
Keywords
Introduction
Postpartum depression (PPD) is one of the most common morbidities of childbearing, bearing a significant mental and public health concern. The Centers for Disease Control and Prevention (CDC) recently estimated the overall prevalence of PPD in the United States to be 13%, with a range of 9.7–23.5% by state. 1 Among women with PPD, 11.5% develop symptoms antenatally, 66.5% develop symptoms within 6 weeks of parturition, and 22% develop symptoms within 12 months of delivery. 2 PPD symptom onset occurs most often within the first few months of childbirth. 3
The American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) categorizes PPD as unipolar major depression along with the specifier ‘with peripartum onset’ when the episode begins during gestation or within 4 weeks following childbirth. 4 Despite this limited time frame, many experts define the postpartum period as the first year after delivery.5,6 Women with PPD may present with excessive worry about their baby and feelings of being inadequate caregivers. A recent study categorized perinatal depression into five distinct subtypes (severe anxious depression, moderate anxious depression, anxious anhedonia, pure anhedonia, and resolved depression) based on differences in symptom quality and time of onset. 7
Despite the high occurrence of PPD, it is underdiagnosed and undertreated. Of women with PPD, only 30.8% are identified in clinical settings, 15.8% receive treatment, 6.3% receive adequate treatment and 3.2% achieve remission. 8 Untreated PPD can have short- and long-term harmful consequences for mother and offspring, including decreased maternal functioning, 9 maternal-infant bonding difficulties, 10 lactation failure 11 and impaired cognitive, 12 behavioral 13 and emotional 14 development of the child. Tragically, untreated PPD is the greatest risk factor for maternal suicide, 15 which is the leading cause of direct maternal mortality in the first postpartum year. 16
Therapeutic interventions for PPD include evidence-based psychotherapeutic, pharmacotherapeutic, neuromodulation, and hormonal treatments. An APA taskforce recommends either psychotherapy or antidepressants as first-line treatment for mild-to-moderate PPD. 17 Evidence-based psychotherapies for PPD including cognitive behavioral therapy and interpersonal psychotherapy18,19 should also be considered as an adjuvant to antidepressants in moderate-to-severe PPD and in cases where women are reluctant to take antidepressants.
Despite the widespread use of standard-of-care antidepressants as the mainstay of treatment for PPD, there is limited evidence on their efficacy and safety, and treatment outcomes remain suboptimal due to their slow onset of action. Treatment with emerging gamma-aminobutyric acid (GABA)ergic neuroactive steroids (NAS), including brexanolone [US Food and Drug Administration (FDA) approved in PPD], zuranolone (investigational) or ganaxolone (investigational), may offer faster response and remission times and improved patient outcomes. This article reviews the evidence base for the efficacy of standard-of-care antidepressants, hormonal therapeutics including progestins and estradiol, and GABAergic NAS in the treatment of women with PPD, as well as the safety of infant exposure to these agents during lactation.
Method for the literature review
An electronic literature search was conducted in April 2021 limited to published English language manuscripts using Scopus, Web of Science, PubMed, Embase and Cochrane. We identified articles using the following key terms in various combinations: postpartum, postnatal, puerperal, depression, antidepressant, selective serotonin reuptake inhibitor (SSRI), serotonin and norepinephrine reuptake inhibitor (SNRI), noradrenergic and specific serotonergic antidepressant (NaSSA), tricyclic or tetracyclic antidepressant (TCA), monoamine oxidase inhibitor (MAOI) and the name of each antidepressant.
Search terms
Postpartum OR post partum or postnatal or post natal or perinatal or peri natal or puerp* or Postpartum Period OR ‘postpartum care’ OR Postnatal Depression OR Post-Partum Depression OR Postpartum Depression OR Post-Natal Depression OR Post Natal Depression OR Puerperal Disorder* or ‘Postnatal Care’[Mesh] OR ‘Depression, Postpartum’[Mesh] OR ‘Postpartum Period’[Mesh] or intrapartum or intra partum or antepartum or ante partum
AND
Antidepressive Agents [tw] OR Antidepressive Agents[pa] or Serotonin Uptake Inhibitors [PA] OR Serotonin Uptake Inhibitors [tw] or ‘Serotonin Uptake Inhibitors’[Mesh] OR SSRIs OR serotonin reuptake inhibitors or SSRIs serotonin-norepinephrine reuptake inhibitors or ‘Serotonin and Noradrenaline Reuptake Inhibitors’ [Pharmacological Action] OR ‘Serotonin and Noradrenaline Reuptake Inhibitors’[Mesh] or SRNIs OR ‘serotonin reuptake inhibitors’ or ‘Antidepressive Agents’[Mesh] OR Brexanolone OR MAOIs OR NASSAs OR TCAs or antidepress* or anti depress* or MAOI* or monoamine oxidase inhibit* or ((serotonin or norepinephrine or noradrenaline or nor epinephrine or nor adrenaline or neurotransmitt* or dopamine*) and (uptake or reuptake or re-uptake)) or noradrenerg* or antiadrenergic or anti adrenergic or SSRI* or SNRI* or TCA* or tricyclic* or tetracyclic* or heterocyclic* or psychotropic* or the name of each antidepressant.
We managed records obtained from the search in Covidence. Inclusion criteria were randomized controlled trials (RCTs) of women with PPD treated with antidepressants, progestin, estradiol or GABAergic NAS during the first year after childbirth, as well as systematic reviews and meta-analyses that included these RCTs or observational studies related to PPD treatment with the aforementioned agents. One of three review authors (YK) inspected abstracts resulting from the search and assessed them for inclusion based on the defined criteria. We excluded studies focused on PPD prevention and PPD treatment with only complementary, alternative, integrative, neuromodulatory, and psychotherapy treatments. Additional RCTs, systematic reviews and meta-analyses were identified by reviewing bibliographies of articles identified within the search.
Search results
The electronic literature search yielded 292 articles after 79 duplicates were removed. This review included the following RCTs from the search: 10 related to PPD treatment with standard-of-care antidepressants20 –29 (Table 1), two related to PPD treatment with estradiol30,31 (Table 2), two related to PPD treatment with brexanolone,32,33 and one related to PPD treatment with zuranolone 34 (Table 3). The following additional trials were identified from the bibliographic reviews: one related to estradiol 35 and two related to progestin PPD treatment36,37 (Table 2). This review also included the following systematic reviews and meta-analyses from the literature search: three related to PPD treatment with antidepressants,38 –40 two related to PPD treatment with brexanolone41,42 and two related to antidepressant use during lactation.43,44 The following additional systematic reviews and meta-analyses that did not result from the search were also identified by reviewing bibliographies of articles identified within the literature search: two related to PPD treatment with estradiol and progestins,45,46 three related to antidepressant use with lactation,47 –49 and two related to the use of progestin during lactation.50,51
Antidepressant randomized clinical trials for the treatment of postpartum depression.

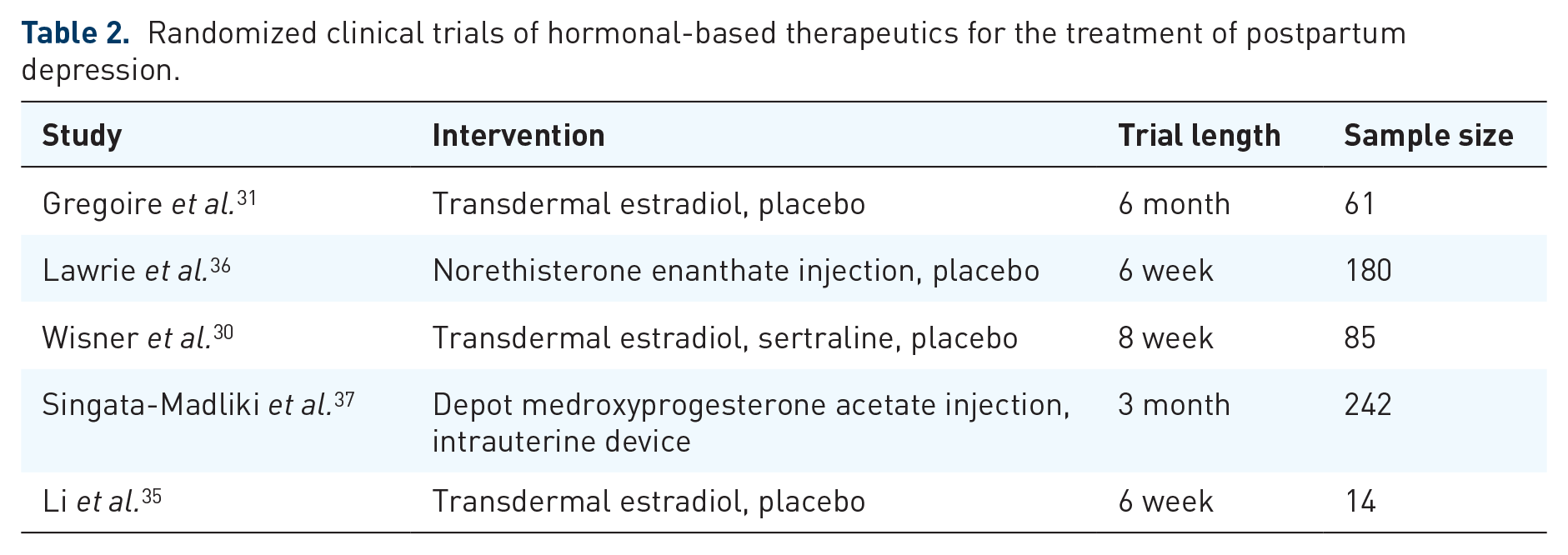
Randomized clinical trials of hormonal-based therapeutics for the treatment of postpartum depression.
Randomized clinical trials of GABAergic antidepressants for the treatment of postpartum depression.

Evidence for standard-of-care antidepressants for PPD
Antidepressants are indicated for moderate-to-severe PPD, with SSRIs typically considered as first-line therapy based on the perceived good tolerability. However, the current evidence on antidepressant efficacy for PPD treatment is limited by small number and sample size of RCTs and the absence of long-term follow-up. In addition, the existing studies are heterogeneous in design with few using a placebo control vs an active comparator such as similar antidepressant or psychotherapy. Ten RCTs evaluated the use of antidepressants (mostly sertraline, fluoxetine, paroxetine and citalopram) for PPD treatment.20 –29 All of these RCTs used a specific antidepressant except one which employed a variety of antidepressants (mostly SSRIs). 24 Two RCTs used the TCAs amitriptyline 29 and nortriptyline. 26 The remaining RCTs used SSRIs: sertraline,20 –23,26 paroxetine25,27 and fluoxetine. 28 No RCTs have evaluated the use of SNRIs, bupropion, mirtazapine, trazodone, nefazodone, MAOIs or TCAs (except nortriptyline and amitriptyline) for PPD treatment.
While several RCTs support antidepressant efficacy in PPD treatment, results have been mixed.
A meta-analysis of three RCTs22,23,25 comparing SSRIs with placebo found that women who received SSRIs were more likely to show symptom response (52.2% versus 36.5%) or remission (46.0% versus 25.7%) at follow-up. 40 A systematic review of six RCTs23 –28 concluded that SSRIs, nortriptyline and psychotherapy are efficacious for short-term PPD treatment, but there is insufficient evidence to demonstrate clear superiority of one over the other. 38 Another systematic review of the same studies concluded that evidence is insufficient to support the efficacy of antidepressants for PPD treatment, 52 but the authors acknowledged that their findings may be explained by methodological limitations including low recruitment rates. Despite limited and inconsistent data, there is a consensus supporting antidepressant use in PPD treatment.
Evidence for estradiol and progestins as treatments for PPD
Current evidence on the use of estradiol is limited by the small number and size of RCTs and mixed results. A small double-blind RCT of transdermal estradiol (TE) in women with severe PPD showed greater and faster symptom improvement compared with those who received placebo, though these results may be confounded by the inclusion of women who were simultaneously treated with antidepressants. 31 Another small double-blind RCT found that women who received TE exhibited non-significantly higher response and remission rates compared with those who received placebo patch, although this study was limited by under-recruitment and loss to follow-up. 35 One large trial comparing TE with placebo did not show significant differences between groups for response or remission rates, though this study was underpowered as it was stopped early due to estradiol serum concentrations not reaching the expected levels. 30 Additional data from large RCTs is needed before estrogen may be recommended to treat PPD.
Fewer data exist on synthetic progesterone treatment. Two RCTs showed that women with PPD treated with the synthetic progestogens including intramuscular injections of norethisterone enanthate 36 and depot medroxyprogesterone acetate 37 experienced increased depressive symptoms compared with those receiving placebo 36 or with an intrauterine device. 37 A Cochrane systematic review concluded that synthetic progestogens should be used cautiously in postpartum women 45 when used for contraception, and are not recommended to treat PPD.
Development of GABAergic neuroactive steroids as novel, fast-acting antidepressants for PPD
Definition and mechanism of action
NAS are naturally occurring steroids and their metabolites that are synthesized from cholesterol. Neurosteroids (NS) refer specifically to those NAS and their metabolites synthesized in the central nervous system (CNS).53,54 The NAS pregnenolone, progesterone, and deoxycorticosterone are pregnane steroid precursors.54,55 Allopregnanolone (3α, 5α-tetrahydroprogesterone), pregnanolone (3α, 5β-tetrahydroprogesterone), and tetrahydrodeoxycorticosterone are pregnane steroid metabolites.
Many NAS are positive allosteric modulators (PAMs) of the inhibitory GABA receptors (R), the ligand-gated and membrane-bound pentameric ion channels that allow or prevent passage of negatively-charged chloride ions into the post-synaptic membrane.56 –58 Synaptic GABA- ARs contribute to low-affinity phasic inhibition, and extrasynaptic GABA- ARs contribute to high affinity tonic inhibition; these differences in function are accounted for by the particular subunits composing the receptor in addition to its location.59,60 GABA- ARs can bind barbiturates, benzodiazepines, general anesthetics, alcohol, and NAS in accordance with their subunit arrangement, composition, and location. 61 Benzodiazepines interact with the abundant γ subunit types, 62 particularly at α/γ interfaces, 63 but the presence of specific receptor subunits can render GABA- ARs unable to bind certain benzodiazepines. 64 NAS appear to bind primarily to the transmembrane α-subunit of GABA- ARs, with the α2 subunit potentially implicated in the anxiolytic effects of NAS, 65 although δ subunits play a large role in the overall sensitization of the receptor to NAS. 66 The homomeric ρ1 GABAARs, currently understood to be largely insensitive to benzodiazepines and barbiturates, bind NAS. 67 As such, the complex pharmacology of GABA- ARs can only be understood in terms of its entire composition: binding properties arise from the interface of multiple subunits in addition to the composition of a specific subunit. 68 For these reasons, NAS studied as PPD pharmacotherapies should not be mistakenly assumed to be equivalent in mechanism or side effect profile to these other GABA- AR-binding psychoactive substances.
GABAA R complexes in the brain are located in specific regions, circuits, and cells. 69 Therefore, in addition to subunit composition and phosphorylation, local steroid metabolism also contributes to the selectivity of the interactions between GABAA Rs and NAS. 70 The binding of NAS to GABAA Rs typically potentiates both synaptic and extrasynaptic receptors and results in increased GABAA R surface expression.71,72 Both tonic and phasic GABAergic neurotransmission are modulated by NAS, leading to changes in the excitatory–inhibitory balance of those specific networks. 73 NAS are critical in the regulation of the hypothalamic–pituitary–adrenal (HPA) axis during acute and chronic stress as well as nonstress conditions.74,75 One pathway that is important to the pathophysiology of PPD involves the hypothalamic paraventricular nucleus (PVN), an area of the brain involved in the neuroendocrine and autonomic response to stress; NAS affect the duration of stress-induced modulation of GABAergic transmission in the PVN. 76 In addition to integral action in the HPA axis, NAS have been shown to have anti-inflammatory and neurotrophic effects within the CNS.77,78 Multiple neuropsychiatric illnesses may involve the action of NAS,79 –82 including PPD.83,84 Well-established research suggests that PPD involves a differential response of the stress steroid system as well as a differential (epi)genetic risk in serotonergic and GABAergic signaling which act as moderators or mediators between changes in the reproductive steroid system and clinical symptomatology. 85 Consequently, synthetic NAS and their analogs became a target of research as possible therapeutics.
Evidence for brexanolone as a treatment for PPD
Brexanolone (ZULRESSO) is the first FDA approved medication indicated for unipolar PPD. A soluble, intravenous preparation of synthetic allopregnanolone, brexanolone is a potent, selective, PAM of extrasynaptic and synaptic GABAARs. 86 It is administered as a 60-hour peripheral intravenous (IV) infusion through a programmable peristaltic infusion pump. The initial dosage is 30 µg/kg/hour from hour 0 to 4, which is then increased to 60 µg/kg/hour from hour 4 to 24, then increased again to 90 µg/kg/hour from hour 24 to 52. At this time, a reduction in dosage to 60 µg/kg/hour may be considered for women who do not tolerate 90 µg/kg/hour. During hour 52–56, the dosage is reduced to or continued at 60 µg/kg/hour, then reduced to 30 µg/kg/hour during hour 56–60 hours, and finally the infusion is terminated at hour 60. The 60-hour infusion generally requires the preparation of five infusion bags with additional bags needed for women ⩾90 kg.
Brexanolone has demonstrated rapid reduction of PPD symptoms in open-label 87 and placebo-controlled RCTs.32,33 The placebo-controlled trials were conducted in healthy women aged 18–45 who were within 6 months postpartum and had an onset of a major depressive episode no earlier than third trimester and no later than 4 weeks following delivery. Participants had moderate to severe depression as rated by the 17-item Hamilton Rating Scale for Depression (HAM-D17) 88 total score ⩾26 or 20–25 at study entry. Women entering the study were either antidepressant-free or were on a stable dose of a traditional antidepressant.
Subjects were randomized to receive placebo or brexanolone IV 90 μg/kg/hour or 60 μg/kg/hour for 60 hours. The primary outcome measure was the least-squares mean change in HAM-D17 total score from baseline to hour 60. Safety, tolerability and depression severity were assessed through day 30. Across a range of disease severities, at hour 60, there were significantly larger mean reductions from baseline in HAM-D total scores with brexanolone IV 90 μg/kg/hour (-17.0; p < 0.001) and brexanolone IV 60 μg/kg/hour (-19.1; p < 0.001) versus placebo (-12.8). Significant differences from placebo were observed at hour 24 (both dose groups p = 0.001) and maintained through day 30 (p ⩽ 0.021). 32 Post hoc analyses showed that depression remission (defined as HAM-D17 total score ⩽7) and response (defined as ⩾50% reduction in HAM-D17 total score from baseline) rates were 50% versus 25% (brexanolone versus placebo) and 75% versus 55% (brexanolone versus placebo) at hour 60, respectively.
The most common adverse events reported in clinical trials with incidence ⩾5% and at least twice the rate of placebo were sedation/somnolence, dry mouth, loss of consciousness, and flushing/hot flush. Adverse events involving sedation and somnolence necessitated dose interruption or reduction in 5% of brexanolone-treated patients compared with 0% of placebo-treated patients. Four percent of the brexanolone-treated patients compared with 0% of the placebo-treated patients were reported to have loss of consciousness or altered state of consciousness during the infusion, with time to full recovery ranging from 15 to 60 minutes. 32 Based on these adverse event reports, brexanolone is currently a Schedule IV medication with a black box warning for excessive sedation and sudden loss of consciousness. Infusion should be halted for any signs or symptoms of excessive sedation; it may be restarted after symptoms resolve with or without a dose reduction as clinically appropriate. In the event of hypoxia or loss of consciousness, infusion should be stopped permanently.
Brexanolone is currently available only through a restricted risk evaluation and mitigation strategy (REMS) program to reduce the risk of serious adverse events. The REMS program ensures that brexanolone is administered in a medically supervised setting capable of providing monitoring, such as continuous pulse oximetry and assessment of sedation during awake periods, throughout the IV infusion, that health care settings and pharmacies involved in providing infusions are properly certified, that patients are informed of the risk for excessive sedation and sudden loss of consciousness and the necessity of monitoring for such symptoms during the infusion, and that patients are enrolled in a registry to monitor adverse events.
The terminal half-life of brexanolone is approximately 9 hours and it is extensively metabolized by non-CYP pathways including keto-reduction, glucuronidation and sulfation. 86 Brexanolone should not be used in patients with a hypersensitivity to allopregnanolone or other NAS and in patients with end stage renal disease with an estimated glomerular filtration rate (eGFR) < 15 mL/minute/1.73 m2. As brexanolone is a GABA PAM, concurrent CNS depressants including benzodiazepines, opioids and alcohol should be used with caution. In placebo-controlled studies, a higher percentage of brexanolone-treated patients who used concomitant antidepressants reported sedation-related events. 32
Other neuroactive steroids in development for the treatment of PPD
Zuranolone is an oral, potent, selective extrasynaptic and synaptic GABAAR PAM currently in clinical trials.89,90 A recent double-blind, placebo-controlled phase 3 trial randomized 153 participants to a 14 day course of zuranolone 30 mg or placebo. 34 Participants were then followed for 4 weeks. Participants receiving zuranolone had a significant reduction in least-squares mean HAM-D17 total score versus those receiving placebo (-17.8 versus -13.6, p = 0.003). In addition to efficacy for the primary endpoint of total score, significant differences in efficacy of zuranolone were observed at Day 3 (p = 0.026) and were sustained through Day 45 (p = 0.003). HAM-D17 response (72% versus 48%, p = 0.005) and remission rates (45% versus 23%, p = 0.012) were significantly greater in the zuranolone group at Day 15, and these significant differences were maintained through Day 45 (response p = 0.022; remission p = 0.010), 4 weeks after zuranolone cessation. The most common adverse events (⩾5%) reported in the zuranolone group were sedation, headache, somnolence, dizziness, upper respiratory tract infection, and diarrhea. One participant receiving zuranolone reported a transient confusional state with sedation on Day 3, which resolved within hours. Neither the active nor placebo group reported syncope or loss of consciousness. There is an ongoing randomized, double-blind placebo-controlled trial of oral zuranolone evaluating its efficacy in severe unipolar PPD (NCT04442503).
Ganaxolone, the 3β-methylated synthetic analog of allopregnanolone, is also in development for the treatment of unipolar PPD. Ganaxolone, like allopregnanolone, is an extrasynaptic and synaptic GABAAR PAM, but it differs significantly in its lack of affinity for estrogen or progesterone receptors. 91 Trials of ganaxolone have included both IV and oral formulations (NCT03460756; NCT03228394); however, published results are not yet available.
Safety of antidepressant pharmacotherapy use during lactation
The evidence on the safety of infant exposure to antidepressants during lactation largely consists of small observational studies. A variety of lactation safety indices have been used in the literature to estimate the amount of a drug transferred into breast milk. A systematic review comparing antidepressant excretion ratios into breast milk, derived from dividing the antidepressant concentration in breast milk by that in the maternal serum, found the highest ratios for venlafaxine, mianserin and escitalopram and the lowest ratios for reboxetine, trazodone and amoxapine. 47 The infant serum level of a drug is a more direct and accurate measure of infant exposure. In a pooled meta-analysis of 57 studies, the use of nortriptyline, paroxetine and sertraline during breastfeeding produced undetectable serum levels in more than 200 newborns, while fluoxetine, citalopram and the metabolite of venlafaxine, O-desmethylvenlafaxine, resulted in measurable but usually low levels in some infants. 48 This analysis indicated that while all antidepressants were detected in breast milk, they were not always spotted in infant serum.
The degree to which the concentration of medication found in breast milk and infant plasma influences its lactation safety profile remains uncertain. Among SSRIs, while there is more data supporting the safety of sertraline 44 and paroxetine during lactation, a systematic review found that risk of infant exposure to this class through breast milk appears to be low. 43 In addition, while less breastfeeding safety data exists for SNRIs, the available data indicates that venlafaxine, desvenlafaxine and duloxetine are compatible with lactation. 43 Furthermore, TCAs may be used while breastfeeding since the infant exposure is low and serious side effects have not been observed, except doxepin. 92 Nortriptyline is generally the preferred TCA for use with lactation due to its favorable safety profile. 92 MAOIs are generally not used in breastfed infants given their potential adverse effects as insufficient data are available about their safety during lactation. Insufficient data are available regarding the safety of mirtazapine, 49 bupropion and serotonin modulators (trazodone, nefazodone and vilazodone) in breastfed infants. Nonspecific adverse effects to monitor for in nursing babies exposed to standard-of care antidepressants include sedation, sleep disturbance, irritability, and poor feeding. 93
Limited data indicate maternal use of transdermal estradiol up to a dose of 200 µg daily during lactation does not increase estradiol or estrone serum concentrations in breastfed infants or negatively impact infant growth; 94 however, it has been associated with an increased risk of impaired lactation. 95 Recent systematic reviews found that maternal use of progestin-only contraceptives does not adversely affect breast milk composition, lactation duration or the growth and development of breastfed infants.50,51
For brexanolone, the maximum relative infant dose during infusion is between 1% and 2% of the maternal weight adjusted dosage. 86 A relative infant dose of <10% is considered acceptable in a healthy postnatal infant; 93 however, this parameter does not translate directly into bioavailability in the infant.
No studies of zuranolone or ganaxolone use during lactation resulted from our structured literature search.
Conclusion
There are a growing number of antidepressant pharmacotherapy studies in PPD. The recent novel therapeutic development of GABAergic NAS for the treatment of PPD is a significant and exciting era in the field of PPD and other fields where NAS are under investigation, including post-traumatic stress disorder, 96 major depressive disorder 97 without peripartum onset, traumatic brain injury 98 and epilepsy. 99 When selecting an antidepressant, the clinician should consider factors including breastfeeding status, psychiatric diagnoses, current and past symptom severity, suicidal risk, past psychiatric history, prior and current psychiatric treatment efficacy and tolerability, medical comorbidities, family psychiatric history, patient treatment preference and ability to comply with the recommended treatment plan. Regarding use in lactation, the clinician must weigh the risks of infant drug exposure through breast milk with the risk of untreated maternal PPD. While limited high-quality data exist on antidepressant use during lactation, there is a consensus that the overwhelming benefits of treating PPD with antidepressants during lactation in most cases outweigh the low risks of antidepressant use while breastfeeding healthy, full-term infants. In addition, despite the varying levels of antidepressants found in breast milk and infant serum, the choice of antidepressant for a lactating woman should be based on her prior treatment history and potential adverse effects on the mother and infant.
Ideally, future novel PPD therapeutics should be fast-acting and offer shorter treatment duration. These properties will not only limit adverse events for the mother and her child, but also increase treatment adherence. Given the heterogeneous phenotypic presentation of PPD, future work should focus on determining which pharmacotherapeutic interventions, as well as other non-pharmacotherapeutic interventions not reviewed here, may preferentially benefit women with differing clinical presentations, thus personalizing care for the mother–infant dyad.
Footnotes
Acknowledgements
We acknowledge Janice Lester, MLS, the Reference and Education Librarian at the Health Science Library of Long Island Jewish Medical Center at Northwell Health for her assistance with the literature review search.
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Deligiannidis serves as a consultant to Sage Therapeutics, Inc, and Brii Biosciences, and reports grants awarded to Zucker Hillside Hospital/Feinstein Institutes for Medical Research during the conduct of the brexanolone injection and zuranolone clinical trials. Dr Deligiannidis received grants from the National Institutes of Health (NIH) and Vorso Corporation and royalties from an NIH employee invention outside of the submitted work. Drs Kaufman and Carlini have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH grant (1R01MH120313) supported Dr Deligiannidis’s time spent on writing and publication of this article.