
Abstract
Background:
A quality improvement programme addressing prescribing practice for depression was initiated by the Prescribing Observatory for Mental Health.
Methods:
A baseline clinical audit against evidence-based practice standards was conducted in UK adult mental health services.
Results:
A total of 55 mental health services submitted data for 2082 patients, under the care of a community psychiatric team (CMHT) for at least a year, with a diagnosis of moderate or severe unipolar depression, 54% of whom had a comorbid psychiatric diagnosis. Selective serotonin reuptake inhibitors were prescribed for 35% of the patients, other newer generation antidepressants for 60%, tricyclic antidepressants for 6% and monoamine oxidase inhibitors for <1%. The most commonly prescribed individual antidepressants were mirtazapine (33%, usually in combination with another antidepressant), venlafaxine (25%) and sertraline (21%). Patients with severe depression were more likely (p < 0.001) to be co-prescribed an antipsychotic medication, lithium, or to have received electroconvulsive therapy. There was a documented clinical review in the last year in 85%, with a symptom rating scale used in 11%. A documented comprehensive treatment history was accessible for 50% of those prescribed antidepressant medication.
Conclusion:
Patients with moderate or severe depression remaining under the care of a CMHT for longer than a year are clinically complex. The failure to achieve a level of wellness allowing discharge from mental health services may be partly related to the finding that not all patients had the benefit of a systematic approach to clinical assessment and sequential testing of available evidence-based pharmacological interventions.
Introduction
In the United Kingdom (UK), most people with depression are treated in primary care, with a relatively small proportion referred to psychiatric services. The gatekeeper role of general practitioners in the UK means that people with depression who are referred to psychiatric services will nearly always have received initial treatment in primary care with one or more antidepressant medications and/or counselling or another psychological therapy. The National Institute for Health and Care Excellence (NICE) guidelines for the management of depression propose a ‘stepped-care’ approach to the treatment of depression based on clinical criteria and treatment needs. 1 Most depressed patients seen in secondary care mental health services meet the criteria for Step 3 (depression with inadequate response to initial interventions) and Step 4 (severe and complex depression including risk to life) and require more intensive treatment delivered in specialist settings, ranging from outpatient support to inpatient care. Given that depression in the majority of patients referred to secondary care will have failed to improve with initial management in primary care, appropriate optimisation and sequencing of treatments is an important component of management. In spite of the lack of a standard treatment regimen, there is evidence that depression is treated more effectively if a systematic approach based on algorithms is used. 2
A better understanding of how current practice is aligned with recommended best practice is an important first step in being able to improve the management of depression in secondary care mental health services, and potentially the outcomes for patients. So, in 2019, the Prescribing Observatory for Mental Health (POMH-UK) conducted a baseline clinical audit as part of a quality improvement (QI) programme focussing on prescribing for depression in UK mental health services. Prescribing performance was measured against evidence-based practice standards derived from the NICE and British Association for Psychopharmacology (BAP) treatment guidelines for depression.1,3 As part of this baseline audit, data were submitted for patients who had been under the care of a community psychiatric team (CMHT) for more than 1 year and had a current diagnosis of moderate or severe depression. We report here on current UK prescribing practice for these patients.
Methods
POMH-UK invited all 64 member healthcare organisations in the UK to participate in a QI programme that focused on the pharmacological treatment of depression. Data were collected during May and June 2019 by clinicians and clinical audit staff using a bespoke data collection tool. These data allowed for the assessment of clinical performance against recommended best practice in the NICE and BAP guidelines for the treatment of depression,1,3 in relation to the quality of clinical assessment of people with depression and the use of evidence-based pharmacological strategies for severe and refractory depressive illness. The data collected included age, gender, ethnicity, sub-type of depression (clinical diagnosis), co-morbid psychiatric diagnoses and details of the psychotropic medication currently prescribed. Information was also collected in relation to the quality of clinical review in the previous year; whether the symptoms and severity of depression had been assessed using a formal rating scale; whether response to treatment, medication adherence and side effects had been assessed; whether the use of substances and the presence of co-morbid physical and mental illness had been considered when reviewing the treatment plan; and whether a comprehensive history of the pharmacological strategies for depression previously tested was accessible in the clinical records.
Data submission and analysis
Anonymised data were submitted online during June and July 2018 using Formic software (Formic Ltd., Middlesex, UK) and analysed using SPSS (SPSS Inc., Chicago, IL, US).4,5 Participating mental health services were sent a copy of their submitted dataset along with any data cleaning queries, allowing data entry errors to be identified and rectified.
Descriptive statistics, along with χ2 tests and t tests were used to describe the demographic and clinical characteristics of the moderate and severe depression sub-groups and explore differences between these sub-groups. Given the large sample size, it was anticipated that such differences might be more robustly interpreted if the threshold for statistical significance was set at p < 0.001.
Results
A total of 55 healthcare organisations submitted data for 2082 patients, 1142 of whom had a clinical diagnosis of moderate depression and 940 had a diagnosis of severe depression, who had been under the care of a CMHT for more than 1 year.
The demographic and clinical characteristics of the population as a whole and the two severity sub-groups are shown in Table 1. Compared with the moderate depression sub-group, the severe depression sub-group was slightly older (mean 52.0 versus 54.4 years; p = 0.001) and less likely to have a co-morbid diagnosis of an anxiety spectrum disorder (26% versus 19%; p < 0.001) or a personality disorder (14% versus 7%; p < 0.001).
Demographic and clinical characteristics of patients with a clinical diagnosis of moderate and severe depression under the medium to long-term care of a CMHT.
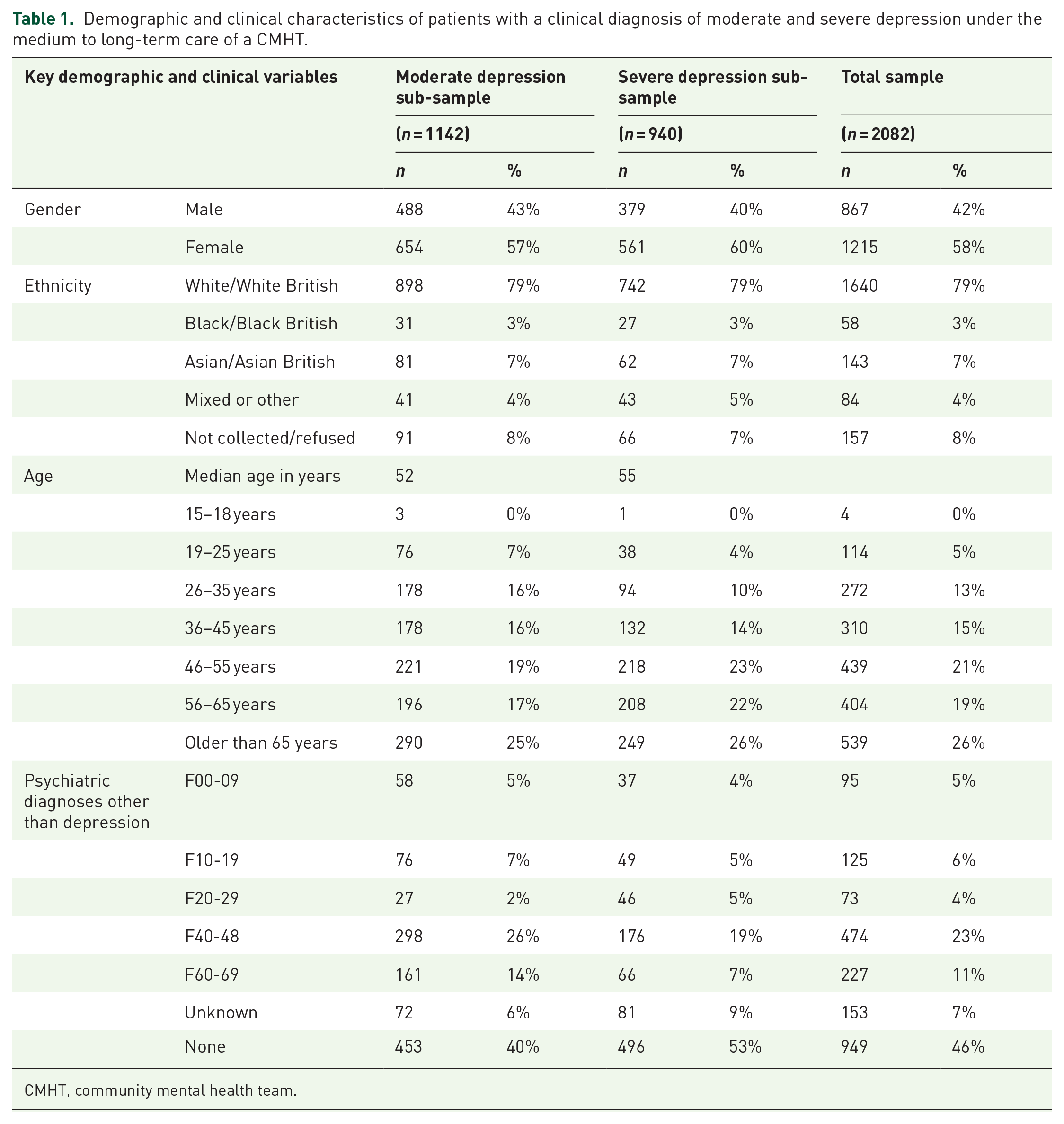
CMHT, community mental health team.
Antidepressant medication prescribed
Antidepressant medication was currently prescribed for 1042 (91%) of the moderate depression sub-group and 863 (92%) of the severe depression sub-group. Details of the antidepressant medication prescribed by sub-group is shown in Table 2.
Antidepressant medication currently prescribed for patients with moderate depression or severe depression under the medium to long-term care of a CMHT.
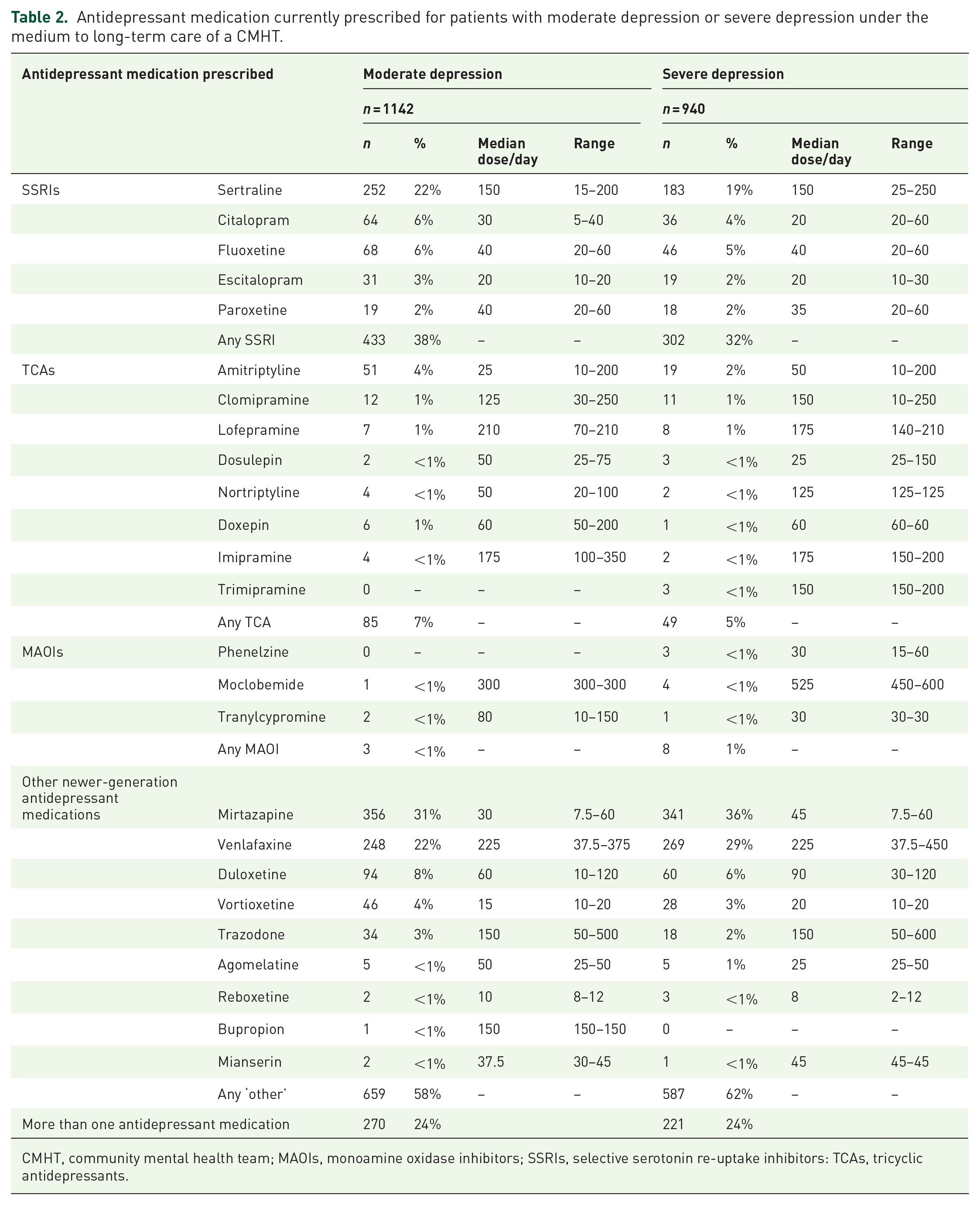
CMHT, community mental health team; MAOIs, monoamine oxidase inhibitors; SSRIs, selective serotonin re-uptake inhibitors: TCAs, tricyclic antidepressants.
Although selective serotonin reuptake inhibitors (SSRIs) were prescribed numerically more often in the moderate depression sub-group and antidepressants from the ‘other’ category in the severe sub-group, neither of these differences was significant at the level of p < 0.001.
Where combined antidepressants were prescribed, more than four-fifths of these combinations included mirtazapine: 80% in the moderate depression sub-group and 86% in the severe depression sub-group. With respect to moderate depression, the antidepressants most commonly co-prescribed with mirtazapine were venlafaxine (n = 93; 34% of combinations), sertraline (46; 17%), duloxetine (16; 6%), fluoxetine (14; 5%) and amitriptyline (14; 5%), whereas for severe depression these were venlafaxine (112; 51%), sertraline (38; 17%) and duloxetine (14; 6%). No other combination of antidepressant medications accounted for more than 5% of all the combinations prescribed in either the moderate or severe depression sub-groups.
Clinical review of depression
Of those patients with moderate depression, 956 (84%) had a documented clinical review in the last year addressing the symptoms and severity of their depression, and in 102 (11%) of these cases a formal rating scale had been used. The respective figures for the severe depression sub-sample were 807 (86%) and 85 (11%). For the moderate depression sub-sample, there was documented evidence that, at clinical review, the use of substances (644: 56%) and the contribution of any co-morbid physical illness (839: 73%) or co-morbid mental illness (890: 78%) to the clinical presentation had been considered. The respective figures for the severe depression sub-sample were 521 (55%), 667 (71%) and 704 (75%). None of the small numerical differences in proportions between the moderate and severe depression sub-samples were statistically significant.
Antidepressant augmentation strategies
To explore the pharmacological strategies that are used in combination with antidepressant medication for the treatment of depression, we selected, for further data analyses, those patients prescribed antidepressant medication but without a co-morbid diagnosis of a schizophrenia spectrum disorder (ICD10 F20-29). This yielded 1018 cases in the moderate depression sub-sample and 825 cases in the severe depression sub-sample. The patients in the latter sub-sample were almost twice as likely (534; 65%) to be currently prescribed antipsychotic medication as those in the former (362; 36%: p < 0.001) and this difference was driven by greater use of olanzapine (21% versus 7%: p < 0.001), aripiprazole (14% versus 5%: p < 0.001) and risperidone (8% versus 3%; p < 0.001). Although quetiapine was the most commonly prescribed antipsychotic overall, there was no difference in the prevalence of prescribing of this medication between the moderate (18%) and severe (20%) depression sub-samples (p = 0.314).
Of those patients with severe depression, 406 (49%) had psychotic symptoms. These patients were significantly more likely (p < 0.001) to be prescribed olanzapine (27% versus 15%), risperidone (13% versus 3%), or aripiprazole (20% versus 8%), compared with those patients with severe depression but without psychotic symptoms. The respective proportions receiving quetiapine were not significantly different (18% versus 22%: p = 0.079).
Just under half of both sub-samples were co-prescribed other psychotropic medicines with their antidepressant medication, most commonly benzodiazepines (17% and 18% respectively in the moderate and severe depression sub-samples), z-hypnotics (10%, 10%) and gabapentinoids (12%, 10%), However, lithium was more often prescribed for those with severe depression (12% versus 5%; p < 0.001).
Clinical review of antidepressant medication
In the sub-sample of 1018 patients with moderate depression who were prescribed an antidepressant medication and had no comorbid psychotic illness (ICD10 F20-29), medication side effects had been reviewed in 675 (66%) and medication adherence in 731 (72%). The respective figures for the severe depression sub-sample (n = 825) were 580 (70%) and 615 (75%). These small numerical differences were not statistically significant.
Comprehensive treatment histories were accessible in the clinical records for 504 patients (50%) in the moderate depression sub-sample and 411 (50%) of the severe depression sub-sample. For those patients with a treatment history, the pharmacological strategies that had ever been tested, whether or not currently prescribed, are shown in Figure 1. Comparing those with moderate depression with those with the severe depression, the latter had more often ever received an antipsychotic medication in combination with an antidepressant (78% versus 47%; p < 0.001) and lithium in combination with an antidepressant (20% versus 11%; p < 0.001). There was also a trend towards greater use of venlafaxine in those with severe depression (50% versus 41%; p = 0.006). No other statistically significant differences were seen. It was documented that two or more of the pharmacological strategies shown in Figure 1 had been tested in 264 (52%) of those patients with moderate depression and 268 (65%) of those with severe depression, whereas in 104 (21%) and 36 (9%) respectively, none of these strategies had ever been tested.

Pharmacological treatments co-prescribed with an antidepressant in the sub-samples of patients with moderate depression (n = 504) and severe depression (n = 411) for whom a treatment history was available in the clinical records.
The treatment histories revealed that psychological treatments had been used in the past in 298 (59%) patients with moderate depression and 225 (55%) with severe depression (p = 0.183) and this was cognitive behavioural therapy in two-thirds of cases (n = 203 and n = 152 respectively). We did not collect data relating to any psychological treatments that were currently being provided.
Electroconvulsive therapy was used either in the past or currently in 30 (6%) patients with moderate depression and 71 (17%) with severe depression (p < 0.001).
Discussion
Our data suggest that patients with moderate or severe depression who remain under the care of a CMHT for longer than a year are clinically complex in that more than half have a co-morbid psychiatric diagnosis and the vast majority are prescribed antidepressant medication, often in combination with other psychotropic medications.
Which antidepressant medications are currently prescribed?
Mirtazapine, venlafaxine and sertraline were the most commonly prescribed antidepressants overall, but the pattern of prescribing differed between the moderate and severe depression sub-groups, with SSRIs being more often prescribed in the former group and mirtazapine and venlafaxine in the latter, although these differences were not statistically significant. Such prescribing is generally consistent with the recommendations made by NICE 1 : essentially, SSRIs should be considered as a first-line treatment, with mirtazapine (a better tolerated, newer generation antidepressant) fitting the NICE criteria for second-line treatment and venlafaxine kept as a third-line option due to its poorer tolerability profile.
With the exception of mirtazapine, the median doses of most of the commonly prescribed antidepressants did not differ between the moderate and severe depression sub-groups, and were generally consistent with the optimal doses identified in clinical studies. 6 Nevertheless, in a small number of patients with severe depression, the licensed maximum doses of sertraline, citalopram, escitalopram, paroxetine, mirtazapine and venlafaxine were exceeded. The small numbers of such patients and the finding that such prescribing was targeted towards those with severe depression suggests that clinicians are aware of the optimal doses of most antidepressant medications and use higher doses selectively and judiciously. We found that the median daily dose of mirtazapine prescribed for severe depression was 45 mg. This is in contrast with the dose-response meta-analysis of selected antidepressant medications conducted by Furukawa et al. that reported doses of mirtazapine higher than 30 mg a day to be associated with reduced response rates and poorer overall tolerability. 6 Our finding, in conjunction with the common use of mirtazapine in combination with another antidepressant medication, suggests that mirtazapine may be used to target severe and treatment-refractory depressive illness and its relatively favourable side-effect profile may allow higher doses within and, rarely, above the licensed range to be tolerated.
For both moderate and severe depression, sertraline was used more often than all other SSRIs combined. Sertraline may be perceived by clinicians to be a good choice in that the efficacy and tolerability data are favourable compared with many other antidepressants.7,8 There are also data supporting cardiac safety, 9 and sertraline has a relatively low potential for pharmacokinetic interactions with other medications as well as a relatively lower liability for discontinuation symptoms compared with antidepressants with shorter half-lives, 10 particularly paroxetine. 11 But, in addition to the influence of such published data, it is also possible that clinicians have found sertraline to be generally well-tolerated by their patients and not associated with discomfiting or intolerable side effects.
Where there is an inadequate response to an SSRI antidepressant, treatment guidelines for depression recommend subsequent sequencing of antidepressant medications,1,3,12 with tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) generally being third-line options. There are data supporting the efficacy of both TCAs and MAOIs.1,13 However, TCAs are known to be generally less well tolerated than newer antidepressant medications and to be relatively more toxic in overdose,1,14 whereas the older MAOIs interact with a number of medicines as well as tyramine-rich foodstuffs leading to potentially serious side effects such as hypertensive crises and serotonin syndrome. 13
We found that TCAs were infrequently prescribed, with amitriptyline the most used medication in this class: both the lower end of the dosage range and the median doses of amitriptyline prescribed suggest that the clinical indication may have been neuropathic pain rather than depression in the majority of cases. In contrast, clomipramine, lofepramine and imipramine were more often prescribed at the dosage recommended for the treatment of depression.
MAOIs are recommended as a treatment option in refractory depression.1,3 We found very few prescriptions for MAOIs. Menkes et al. suggest that the most likely reasons for the low use of these medicines are a lack of familiarity and concerns about side effects. 13 The older MAOIs are also currently very expensive in the UK and there have been on-going supply chain issues. With respect to moclobemide, there is a lack of consensus over its efficacy in treatment-refractory depression. 15
There is evidence to suggest that an algorithm-guided decision-making process involving sequencing of antidepressant medication with systematic measurement of response increases the chance of remission for patients with depression. 2 However, for patients with moderate to severe depression who have been under the care of mental health services for more than a year, our data suggest that some of the available evidence-based pharmacological treatment options may be under-utilised, and this may limit the potential to achieve response and remission for some patients.
Which antidepressant medications are currently combined?
The prevalence of the use of combined antidepressants did not differ between those patients with moderate and severe depression, with just under a quarter of each being prescribed such a strategy. More than four-fifths of combinations included mirtazapine with an SSRI or serotonin-norepinephrine reuptake inhibitors (SNRI), a strategy supported by NICE, 1 and in those patients with severe depression half of all combinations were mirtazapine with venlafaxine, a combination tested with limited success as a fourth-line option in the STAR*D study. 16 As might be expected, sertraline, which was the most commonly prescribed SSRI overall, was also the SSRI that was used most often in combination with mirtazapine.
There is some evidence from relatively small randomised controlled trials (RCTs) that, compared with an SSRI or SNRI alone, augmentation with mirtazapine leads to a greater reduction in depressive symptoms.17,18 Mirtazapine is an antagonist at noradrenaline alpha-2 as well as 5-hydroxytryptamine receptors 5HT2 and 5HT3, and it has been suggested that this pharmacological profile may potentially enhance the therapeutic effect of SSRIs and SNRIs. 17 The sedative effects of mirtazapine may also be beneficial for patients with depression, particularly in the first few weeks of treatment. However, larger and more recent RCTs, albeit perhaps in less treatment-refractory populations than the current sample, have failed to find a clinically meaningful advantage for mirtazapine augmentation over an SSRI or SNRI alone, and also revealed a greater side-effect burden in the augmentation arms.19,20 So whether, and for whom, combined antidepressants offer an increased chance of response and remission is an area of clinical uncertainty.
Antipsychotic medication used in combination with an antidepressant
Where the illness has not responded sufficiently to antidepressant medication, a further pharmacological strategy that is recommended in treatment guidelines for depression is the addition of an antipsychotic medication.1,3,12 There is most evidence to support the use of quetiapine, 21 olanzapine, 22 aripiprazole, 23 or risperidone. 24 We found that augmentation with one of these four antipsychotic medications was the most common pharmacological strategy employed in routine clinical practice in mental health services, being used in a third of those with moderate depression and two-thirds of those with severe depression.
Quetiapine was the most commonly prescribed antipsychotic medication, being used in almost one patient in five overall, irrespective of the severity of depression. This suggests that many prescribers consider quetiapine to be the first-choice antipsychotic for augmentation of antidepressant medication. Such a view is potentially based on evidence suggesting efficacy in the treatment of depression when used as monotherapy, 25 but may also reflect its established sedative and anxiolytic effects, its relatively favourable tolerability profile and that it is the only antipsychotic medication currently licensed in the UK for the treatment of depression. However, compared with patients with moderate depression, the prevalence of prescribing of olanzapine, aripiprazole and risperidone was almost three-fold higher in those with severe depression. One interpretation of these data is that these specific antipsychotic medications are chosen more often by prescribers when psychotic symptoms are part of the clinical picture. However, we did not collect data relating to sequential trials of antipsychotic augmentation so do not know if patients prescribed these antipsychotic medications had previously received a treatment trial of quetiapine.
Lithium
The effectiveness of lithium combined with antidepressant medication in treating acute episodes of unipolar depression and in preventing relapse is supported by meta-analyses of randomised placebo-controlled trials, 26 pragmatic randomised studies, 27 and population-based cohort studies, 28 and lithium has also been shown to be protective against suicide. 29 Lithium augmentation of antidepressant medication is one of the pharmacological options for treatment-refractory depression recommended by NICE. 1 However, lithium is not an easy medication to prescribe; it has a narrow therapeutic plasma level range and established adverse effects on the kidneys, thyroid and parathyroid. 30
Although lithium was used more often in severe depression, only one patient in five in this sub-sample had ever received a trial of this medication. Potential explanations for this low level of use may include the concerns of prescribers and patients regarding the adverse effects of lithium and the burdensome nature of the required biochemical monitoring. Further, the other two augmentation strategies specifically supported by NICE (antipsychotic augmentation of antidepressant medication and combined antidepressants) may be preferred by prescribers because they perceive these strategies to be easier to use, and associated with fewer and/or less severe side effects and less need for additional monitoring. 1
We found that lamotrigine was prescribed for fewer than 1 in 10 patients with moderate or severe unipolar depression suggesting that the use of lamotrigine for this indication is not routine in UK mental health services. While there is evidence to support the use of lamotrigine in both the treatment of acute episodes of bipolar depression, 31 and the prevention of depressive relapse in bipolar illness, 32 efficacy in unipolar depression remains unproven.3,33
Although there is no convincing evidence that vortioxetine is more effective than any other antidepressant, it does have a different pharmacological profile and so is recommended by NICE as an option for treating depression that has not responded adequately to sequential trials of two antidepressant medications within the current episode. 34 Given that our sample of patients with moderate and severe depression had been under the care of CMHTs for at least 1 year, the vast majority are likely to have received at least two different antidepressant medications during this time, yet fewer than 1 patient in 20 was currently prescribed vortioxetine. This suggests that psychiatrists have not to date altered their prescribing practice in light of this guidance, and may preferentially use more established and familiar pharmacological strategies for which the evidence base in severe and refractory depression is stronger.
Treatment history
When past and current treatments were considered together, those patients with severe depression were significantly more likely overall to have received treatment with antipsychotic medication, lithium and ECT, and numerically more likely to have ever been prescribed venlafaxine. They were also more likely to have received at least two other pharmacological strategies, as listed in Figure 1. However, a comprehensive treatment history was available in the clinical records for only half of our population of patients with moderate or severe depression, all of whom had been under the care of a CMHT for at least 1 year, limiting the ability of clinicians to effectively care plan for this complex and persistently unwell group of patients. Where such a history was available, the differences in prescribing between moderate and severe depression for ‘ever prescribed’ medication were similar to ‘currently prescribed’, as discussed previously.
In those with severe depression, almost all prescriptions for antipsychotic medications were current, with few such prescriptions having been started in the past and subsequently discontinued, suggesting that the benefits of antipsychotic augmentation of antidepressant medication are perceived to outweigh the risks by both clinicians and patients in the vast majority of cases. However, individual trials of combined antidepressants, venlafaxine, tricyclic antidepressants and lithium were more likely to have been discontinued, suggesting either a lack of efficacy or relatively poor tolerability of these treatment options.
While there is no established standard regimen for sequencing treatments for depression, a suggested algorithm is given in Cowen and Anderson. 35 This consists of adequate to high dosing of a sequence of antidepressants of differing pharmacology, with the addition of augmenting agents including second-generation antipsychotic medication and lithium, concurrent psychological treatments including cognitive behaviour therapy and behavioural activation, and consideration of ECT at a relatively early stage. Our data suggest that, in routine clinical practice, patients with severe depression are likely to receive an individual treatment trial of antipsychotic augmentation of their antidepressant treatment, venlafaxine, combined antidepressants, or psychological therapy, but are much less likely to ever be prescribed a TCA, MAOI or lithium, with less than 20% having received ECT. This may partly reflect the absence of a comprehensive treatment history that could usefully inform the use of these strategies.
Clinical review
More than four-fifths of patients in our audit sample had their care reviewed in the last year but symptoms were assessed and quantified using a formal rating scale for only one patient in ten, despite such scales being readily available, and recommended in both the NICE and BAP depression guidelines.1,3 Standardised scales are potentially valuable for mapping an individual’s symptoms as well as communicating the symptom profile and severity to other mental health professionals. The use of standardised scales for quantifying symptoms and assessing the response of target symptoms to different treatment strategies is particularly important for those patients who have a treatment-refractory illness.
The quality of medication review did not differ between those with moderate and severe depression, a possible indication that more structured care is not targeted towards those with more severe illness. Further, medication adherence had been reviewed in the previous year in around three-quarters of patients and medication side effects in two-thirds, suggesting that questioning relating to the acceptability of prescribed antidepressant medication falls short of best practice in UK community mental health services. Poor adherence to prescribed medication is associated with worse outcomes in patients with depression. 36 The World Health Organisation has stated that improving adherence to prescribed medication in general would have a greater impact on public health than any improvements in specific medical treatments, leading to the proposal that non-adherence should be a diagnosable condition for which interventions are offered. 37 Where the illness has not responded sufficiently to prescribed medication, systematic and sensitive questioning about adherence and side effects is essential to inform the treatment plan. Otherwise non-adherence may be misdiagnosed as treatment resistance.
Reviews of the current literature conclude that one-third to one-half of people who recover from a depressive episode subsequently relapse in the following year, 3 with the rate being much higher if there are adverse factors such as greater severity of depression, longer episode duration, psychosis, a degree of treatment resistance, a greater number of previous episodes, residual depressive symptoms, social stress/poor social adjustment, and comorbid mental or physical illness. 1 We found that the presence of comorbid physical and mental illness had been reviewed in the previous year in around three-quarters of patients, medication side effects in two-thirds and the contribution of substances to the clinical presentation had been considered for almost three-fifths.
Conclusion
There is evidence to suggest that, in patients with depression, a systematic algorithmic approach with timed evaluation of response followed by treatment adjustment and sequencing according to a predetermined plan at critical decision points offers the best chance of response and remission. 2 Following such an approach requires clear documentation of the efficacy and side effects of each treatment strategy tested, as well as the target symptoms, dosages, adherence and reasons for stopping.
Our data suggest that it is not routine practice for clinicians in secondary care to follow a systematic treatment plan, or indeed to routinely determine and document the severity of depressive symptoms using established rating scales, even though these are readily available, and recommended in both the NICE and BAP depression guidelines.1,3 For patients with moderate-to-severe depression who have been under the care of mental health services for more than a year, some of the available evidence-based pharmacological treatment options may be under-utilised, and this could limit the potential to achieve a level of wellness that allows discharge from mental health services for some patients. If mental health services were to adopt a more systematic approach to the assessment and treatment of depression, the evidence suggests that better clinical outcomes could be achieved.
Strengths and limitations of the study
Participation in POMH QI programmes is voluntary, raising the possibility that Trusts that participate may not be representative of those that do not. However, given the large sample size, with submission of data by the vast majority of mental health Trusts, our findings are likely to be representative of current prescribing practice for patients with moderate to severe depression under the care of UK mental health services.
Our findings relate specifically to care provided in UK mental health Trusts and may not be generalisable to healthcare systems in other countries.
We assessed prescribing practice against recommendations in evidence-based clinical guidelines. Deviation from some guideline recommendations may be appropriate in some cases. We did not directly assess the quality of care for individual patients.
The clinical diagnosis of depression as moderate or severe was cross-sectional and therefore it is unclear to what extent the moderate and severe depression sub-groups reflected enduring states of symptom severity. However, there were some statistically significant differences between these sub-groups on a number of clinical variables, suggesting that this separation has some face validity.
We did not enquire specifically about treatment-refractory illness nor set any criteria that allowed us to derive this diagnosis. However, we consider it reasonable to assume the presence of varying degrees of treatment-refractoriness in our sample of patients with depression under the long-term care of community mental health teams.
Key points
Patients with moderate or severe depression who remain under the care of a CMHT for longer than a year are clinically complex in that more than half have a comorbid psychiatric diagnosis and the vast majority were prescribed antidepressant medication, often in combination with other psychotropic medications.
Although the routine use of standardised scales for depression is recommended in treatment guidelines as being potentially valuable for mapping an individual’s symptoms, assessing response to treatment, and communicating the symptom profile and severity to other mental health professionals, such scales are infrequently used in clinical practice.
In patients with moderate-to-severe depression who have been under the care of UK mental health services for more than a year, some of the available evidence-based pharmacological treatment options may be under-utilised, limiting the potential to achieve response and remission for some patients.
If secondary care mental health services were to adopt a more systematic approach to the assessment and treatment of more severe and treatment-refractory depression better outcomes may be achieved for at least a proportion of patients.
Footnotes
Acknowledgements
Thanks are due to the clinicians and clinical audit staff from the UK mental health services who collected and submitted data as part of this quality improvement initiative, and to Gavin Herrington, the POMH-UK programme manager.
Conflict of interest statement
CP reported participation in a scientific advisory board for Allergan. IMA, PC and OD have no conflict of interest to declare. TREB reported participation in scientific advisory boards for Lundbeck, Newron Pharmaceuticals and Gedeon Richter/Recordati and receipt of an honorarium for a lecture from Janssen.
Ethical statement
Clinical audit by definition does not involve anything being done to patients beyond their normal clinical management and therefore does not require formal ethical approval.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work of POMH is funded wholly by subscriptions from mental health services in the UK.