
Abstract
Cariprazine is one of the newest dopamine-serotonin partial agonists, also known as ‘atypical’ second generation antipsychotics. Originally approved for acute and maintenance treatment of schizophrenia as well as for acute mania and mixed mania/depression, cariprazine has now been approved for bipolar I depression. Additionally, post hoc analyses of bipolar I depressed subjects show that both those with and those without concurrent manic features were improved following treatment with cariprazine. Maintenance studies are in progress in bipolar disorder, as are studies to augment antidepressants in unipolar major depressive episodes insufficiently responsive to treatment. Here, we review specifically the efficacy and safety data of cariprazine in bipolar I disorder and discuss the hypothesized mechanism of action of cariprazine and how it could theoretically be linked to caprazine’s broad therapeutic actions across the mood disorder spectrum.
Introduction
Mood disorders and their treatments are undergoing major paradigm shifts both in diagnostic conceptualization and nomenclature.1–4 Mood disorder treatments are moving away from classical notions of ‘antidepressants’ and ‘antipsychotics,’ which have become confusing terms since classical ‘antidepressants’ are not first line treatments for some forms of depression [e.g. major depressive episodes (MDEs) in bipolar disorder], whereas some classical ‘antipsychotics’ are first line treatments for some forms of depression, even though patients are not psychotic. 3 Thus, a new nomenclature (termed Neuroscience-based Nomenclature or NbN), has been proposed, based on pharmacologic mechanism rather than therapeutic indication, with classical ‘antidepressants’ categorized for example as monoamine reuptake blockers, and classical ‘antipsychotics’ as dopamine antagonists or serotonin dopamine antagonists/partial agonists. 4 Just as the treatments of mood disorders are undergoing a paradigm shift in their nomenclature, so are diagnostic categories for mood disorders. That is, rather than mood disorders being seen in discrete diagnostic categories, (e.g. mania distinct from depression), mood disorders are now conceptualized as lying along a spectrum from depression at one end to mania at the other, with mixtures of subsyndromal mania with depression and subsyndromal depression with mania in between.1–3 These shifts in conceptualization of both the diagnosis and the treatment of mood disorders are having profound effects on clinical practice and it is into this context that the novel agent cariprazine enters for the treatment of mood disorders across the bipolar I spectrum from mania to depression.
Here, we present an overview of the safety and efficacy data on cariprazine in the treatment of bipolar I disorder (BPI) across the spectrum from pure bipolar I depression to bipolar I depression with subsyndromal manic symptoms, to bipolar I mania with subsyndromal depressive symptoms, to pure mania. This review adds to the body of literature discussing cariprazine’s efficacy and side effect profile previously published.5–8 There are no head-to-head studies of cariprazine with the other agents approved for BPI, rendering it difficult to make any comparative statements on safety and efficacy with other approved agents. However, there are notable differences in pharmacologic mechanism of action of cariprazine that we will discuss, specifically as a dopamine-serotonin partial agonist, and, especially, how its unique dopamine D3 partial agonist actions may contribute to its broad therapeutic actions. 9
Cariprazine mechanism of action
Cariprazine is a dopamine-serotonin partial agonist in the same pharmacologic class with brexpiprazole and aripiprazole.4,9 More specifically, cariprazine binds to D3 dopamine, D2 dopamine, and 5HT2B serotonin receptors with high potency, and to 5HT1A serotonin and 5HT2A serotonin receptors with moderate potency, a profile that differs from both brexpiprazole and aripiprazole (Figure 1).9–11 In animal models, cariprazine has antipsychotic effects, 12 not surprising for an agent with D2 partial agonist actions, and indeed cariprazine is approved for the acute and maintenance treatment of schizophrenia. 13 Perhaps the most unique aspect of cariprazine’s pharmacology is that it is D3 preferring, with binding affinity not only higher for the D3 receptor than for the D2 receptor, but with such high affinity binding to the D3 receptor that it is higher than dopamine’s affinity for the D3 receptor, meaning that at physiological doses, there is unique blockade of D3 receptors by cariprazine, unlike most other dopamine agonists/antagonists whose D3 binding is reversible by dopamine (Figure 2). 14 Dopamine D3 receptors are particularly located in limbic areas, the hypothalamus, and the ventral tegmental area/substantia nigra. 15

Representative icon and relative binding affinity for cariprazine.
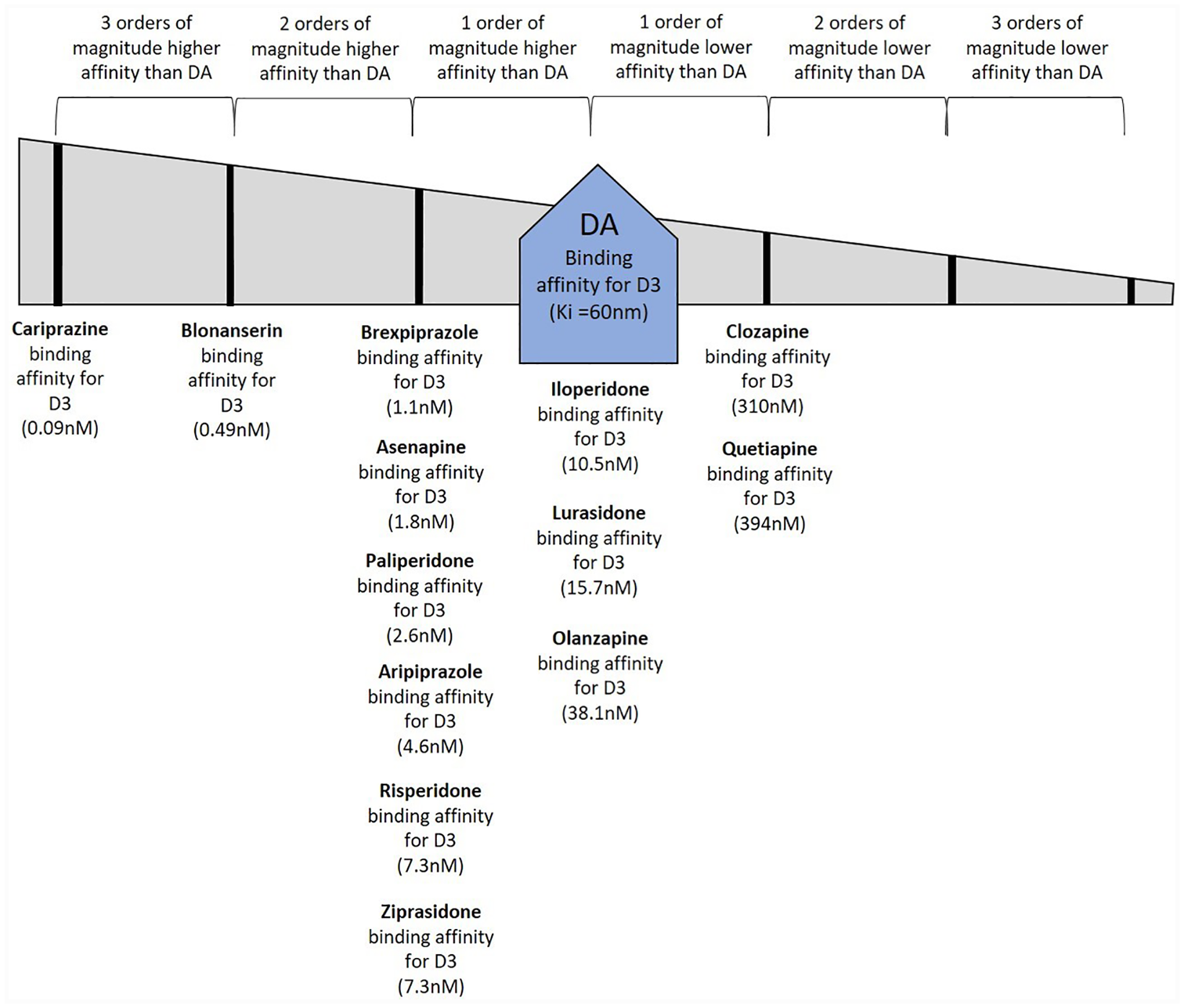
Relative binding affinities of dopamine and antipsychotic drugs for dopamine D3 receptors.
There is intense interest in what this relatively unique high potency D3 partial agonism means for cariprazine’s clinical actions. Of note are observations that cariprazine has procognitive and antidepressant effects, including anti-anhedonia effects in animal models.16–18 These and other data suggest a role for the D3 receptor in reward processing, and this action might be linked to the observed improvement in negative symptoms of schizophrenia, 19 as well as the antidepressant effects in bipolar disorder seen after treatment with cariprazine (discussed below). In fact, a recent meta-analysis indicates greater efficacy of cariprazine compared with other antipsychotics in the treatment of negative symptoms of schizophrenia. 20 One hypothesis for the mechanism of cariprazine’s improvement of anhedonia and mood in bipolar disorder is that partial agonist actions at presynaptic D3 autoreceptors in the ventral tegmental area/substantia nigra, disinhibits dopamine release in prefrontal cortex, promoting positive dopamine tone (Figure 3). 14 Cariprazine’s relatively high binding affinity for serotonin 5HT1A receptors as a partial agonist may also impart antidepressant properties.9,21 Additionally, the binding of cariprazine as a partial agonist/antagonist at dopamine D2 receptors may hypothetically underlie some of its antimanic and antipsychotic effects (Figure 4).

Relative binding affinities of dopamine and antipsychotic drugs for dopamine D2 receptors.
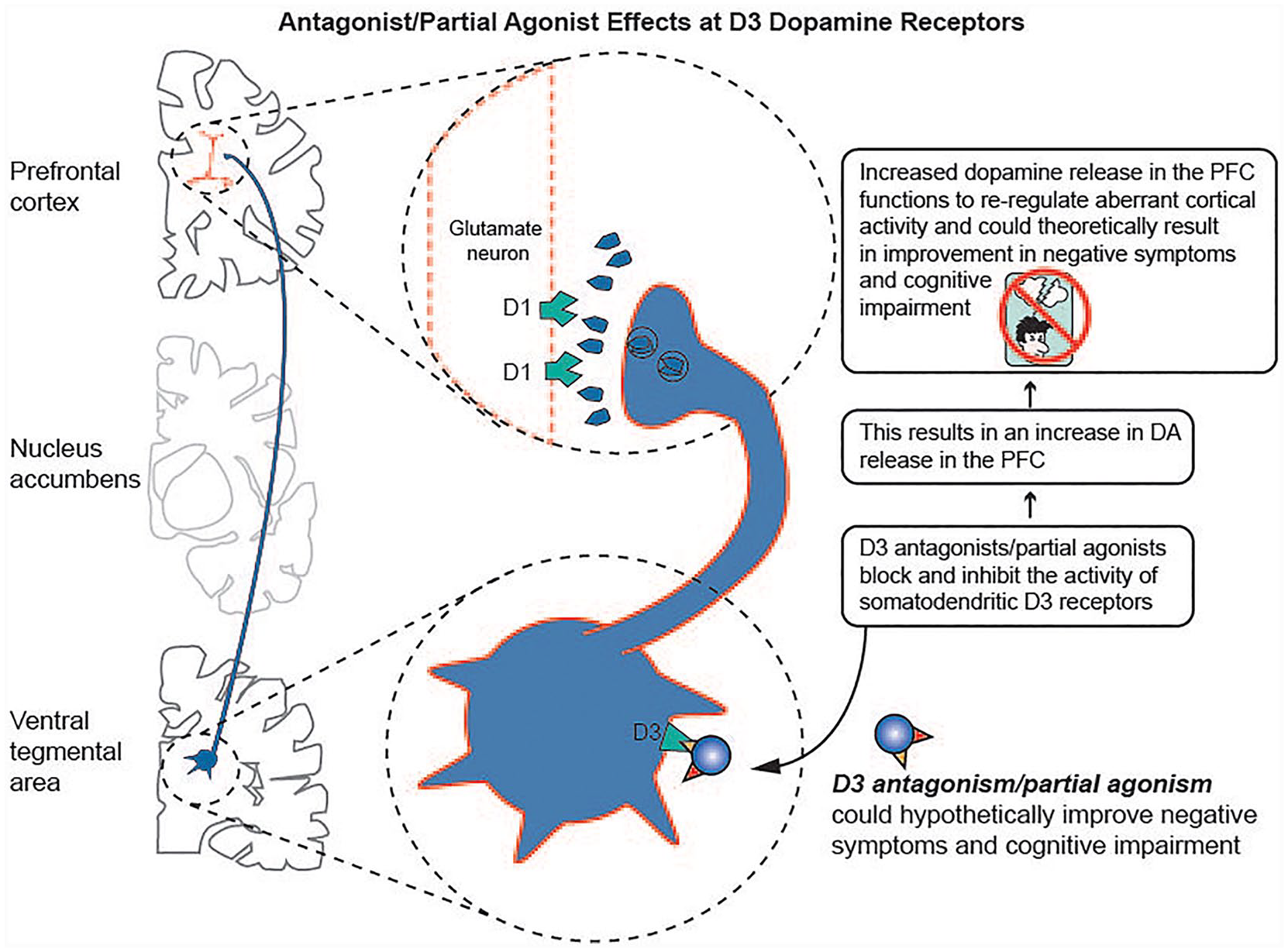
Antagonist/partial agonist effects at D3 receptors.
Another feature unique to cariprazine among atypical antipsychotics is its potential as a long-acting oral treatment. Cariprazine is extensively metabolized by the cytochrome P450 3A4 enzyme (CYP3A4). Although cariprazine itself has a half-life of only 2–4 days, its major metabolite, didesmethyl cariprazine (DDCAR) has a half-life of 1–3 weeks, the longest of any atypical antipsychotic. 10 What this means is that the actions of DDCAR, which has the same, if not more potent, actions on neurotransmitter receptor binding, is responsible for efficacy and tolerability. 22 Thus, on the one hand, effective cariprazine dose may rise over several weeks even though daily dosing stays the same; on the other hand, missing a dose may not be a devastating event. In fact, cariprazine is the only antipsychotic with recommended every-other-day dosing (when cariprazine is taken in the presence of a strong CYP3A4 inhibitor).
Cariprazine clinical efficacy
Cariprazine was approved by the United States Food and Drug Administration (FDA) for the acute treatment of schizophrenia (1.5–6 mg/day) and acute mania/mixed mania in BPI disorder (3–6 mg/day) in September 2015, and for maintenance treatment of schizophrenia in November 2017. Cariprazine is now FDA-approved as a monotherapy for BPI depression (1.5–3.0 mg) as of May 2019, and is currently also in development as an adjunctive treatment for unipolar major depressive disorder. Studies across the spectrum of mood disorders will be discussed here from acute bipolar mania with or without depressive symptoms, to acute bipolar I depression with or without manic symptoms.
Efficacy in mania: acute BP mania, DSM-IV mixed episodes (full criterion mania plus full criterion depression), and DSM5 manic episodes with mixed features of depression
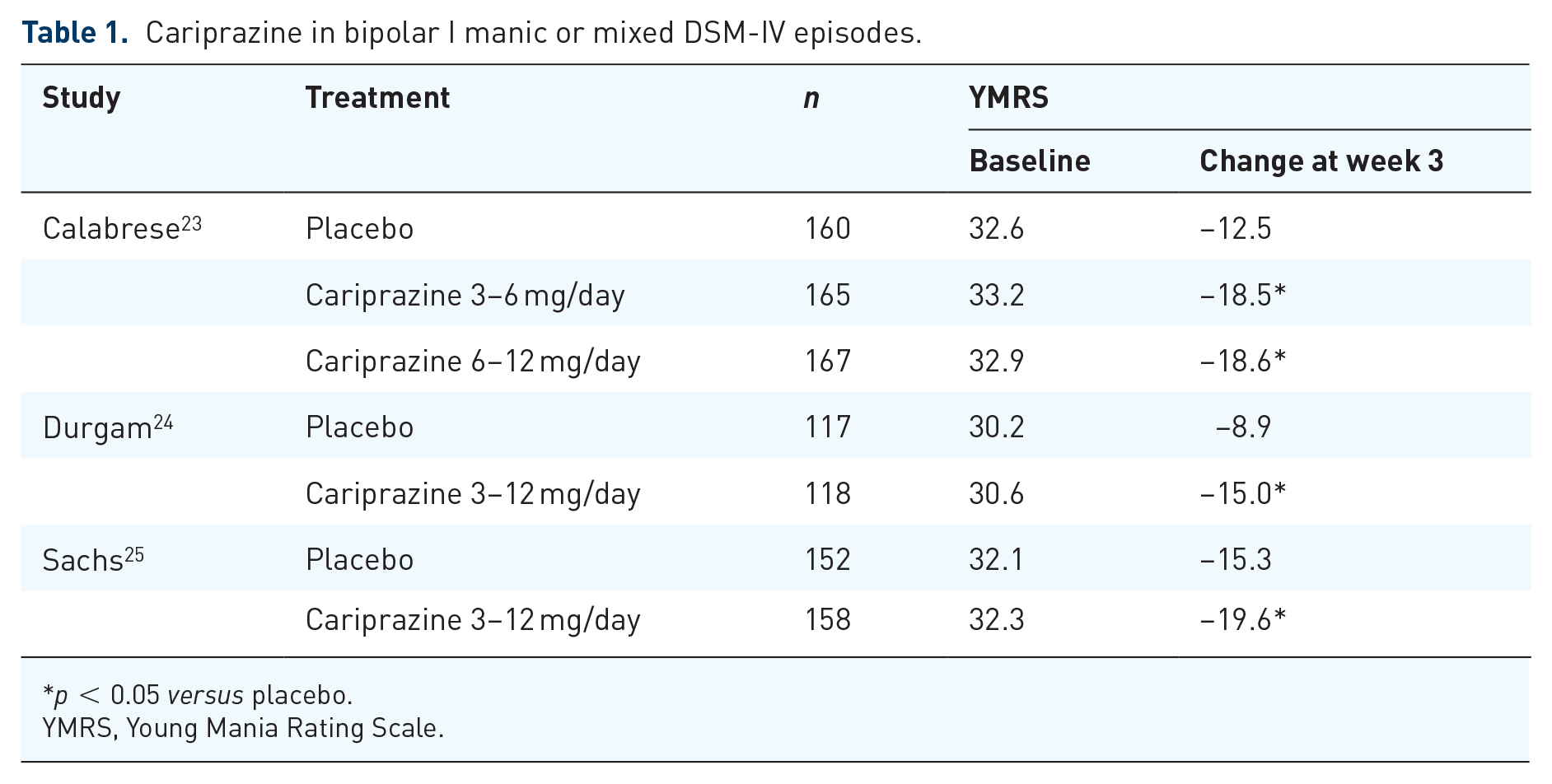
Several short-term (3 week) double-blind, placebo-controlled, randomized phase II/III clinical trials have investigated cariprazine at doses of 3–12 mg/day for the treatment of acute mania or DSM-IV mixed episodes in the context of BPI (i.e. meeting full diagnostic criteria for both a manic and a depressed episode) (Table 1).23–25 All of these trials showed that change from baseline to week 3 on the Young Mania Rating Scale (YMRS) was significantly greater in cariprazine-treated patients compared with placebo-treated patients. Additionally, a greater percentage of cariprazine-treated individuals met response (⩾50% improvement on YMRS score from baseline) and remission (YMRS score ⩽12) criteria at the end of 3 weeks compared with placebo-treated individuals. Furthermore, a 16-week, open label trial of cariprazine for BPI mania or DSM IV mixed episodes showed that cariprazine efficacy was extended over the longer-term. 26 Since there was no greater efficacy in the high dose groups (6–12 mg/day), but greater side effects, cariprazine was approved for the treatment of bipolar mania at doses from 3 to 6 mg/day.
Cariprazine in bipolar I manic or mixed DSM-IV episodes.
p < 0.05 versus placebo.
YMRS, Young Mania Rating Scale.
In a post hoc analysis of all three of these studies pooled together to investigate cariprazine’s efficacy in mania with varying degrees and definitions of concomitant depression, 14% of the cohort had mixed features according to DSM-5 (i.e. three or more symptoms of depression), 15% had two or more depressive symptoms, and 44% had a Montgomery Asberg Depression Rating Scale (MADRS) Score of 10 or more at baseline (Table 2). 27 In each of these groups, cariprazine significantly reduced manic symptoms (Young Mania Rating Scale, YMRS), compared with placebo and numerically reduced depressive symptoms in all groups and significantly so in the MADRS 10 or more subgroup (Table 2).
Cariprazine in bipolar I mania with mixed features.

p < 0.05 versus placebo.
DSM-5 definition.
MADRS, Montgomery Asberg Depression Rating Scale; YMRS, Young Mania Rating Scale.
Efficacy in BP depression with or without concomitant symptoms of mania
Several short-term (6 or 8 weeks with endpoints at week 6) double-blind, placebo-controlled, randomized phase II/III clinical trials have investigated cariprazine at doses of 1.5–3.0 mg/day for the treatment of depressive episodes in BPI (Table 3).28–30 All of these trials showed that change from baseline to week 6 on the Montgomery Asberg Depression Rating Scale (MADRS) was significantly greater in cariprazine-treated patients and 1.5 mg/day compared with placebo-treated patients; all of these trials showed trends to greater efficacy at 3.0 mg/day, and one trial 30 showed significant differences at 3.0 mg/day, as did pooled analysis of all three trials (Table 3). Both 1.5 mg/day and 3.0 m/day are approved doses for bipolar depression. Maintenance trials are in progress.
Cariprazine in bipolar I depression.

p < 0.05 versus placebo.
MADRS, Montgomery Asberg Depression Rating Scale.
In a post hoc analysis of all three of these studies pooled together to investigate cariprazine’s efficacy in depression with symptoms of mania, it was determined that 58.4% of the 1483 patients randomized to treatment had concurrent manic symptoms (YMRS score ⩾4 but <10 (1 study) or 12 (2 studies) (Table 4). 31 Both patients with and without manic symptoms showed significant improvement in MADRS score from baseline compared with placebo, but for patients with manic symptoms, both 1.5 mg/day and 3.0 mg/day were significant but only 1.5 mg/day was significant for patients without manic symptoms (Table 4). 31
Cariprazine in bipolar I depression with or without subsyndromal manic symptoms.

p < 0.05 versus placebo.
YMRS, Young Mania Rating Scale.
Efficacy in MDD
Cariprazine is under investigation as an augmenting agent in unipolar major depressive disorder. One trial investigated the effect of very low dose (0.1–0.3 mg/day or 1–2 mg/day) cariprazine on MADRS scores compared with placebo. 32 Although there was a mean reduction in MADRS scores in the cariprazine-treated groups compared with placebo-treated patients, the differences were not significant. A subsequent study by Durgam and colleagues instituting higher doses of cariprazine (1–2 mg/day and 2–4.5 mg/day) demonstrated statistically significant reductions from baseline to week 8 for the higher dose (2–4.5 mg/day) group compared with placebo. 33 Additional trials in unipolar major depressive disorder are underway. In fact, there are currently six clinical trials currently underway or completed investigating cariprazine for major depressive disorder (www.clinicaltrials.gov).
Tolerability
The side effect profile of cariprazine is different in patients with bipolar depression compared with patients with manic or mixed episodes, probably because of the differences in dosing and titration between the two sets of studies (Table 5).23–33 That is, the most common adverse reactions in the manic/mixed patients, extrapyramidal symptoms and akathisia, were present in a greater percentage of patients than in the bipolar depressed group, likely because the dose was lower and the titration much slower in the bipolar depressed group. The proportion of patients with metabolic shifts of fasting glucose, total cholesterol, and fasting triglycerides was similar to placebo and there was no meaningful increase in mean prolactin levels from baseline to endpoint. The mean weight change was 0.9–1.5 pounds across all trials. The duration of these studies evaluating the side effect profile of cariprazine range from 3 to 19 weeks; longer-term trials may be valuable.
Most common adverse effects (⩾5% and at least twice the rate of placebo). 28

Extrapyramidal symptoms excluding akathisia and restlessness.
Conclusion
Cariprazine becomes the first D3-preferring dopamine-serotonin partial agonist, and the fourth agent overall, along with the serotonin-dopamine antagonists quetiapine, olanzapine/fluoxetine combination, and lurasidone, to be FDA-approved for the treatment of bipolar depression. Cariprazine also becomes the first D3-preferring dopamine-serotonin partial agonist, and the third agent overall, along with the serotonin-dopamine antagonists quetiapine and olanzapine/fluoxetine combination, to be FDA-approved for treatment of bipolar I disorder across the spectrum from mania to depression (Figure 5). In terms of possible efficacy across the entire spectrum of bipolar I disorder from pure depression to pure mania with mixed states in between, cariprazine demonstrates efficacy for various types of mixed states, not just mixed mania depression as defined by DSM-IV, but retrospective studies suggest efficacy in mania with or without subsyndromal depressive symptoms as well as in bipolar depression with or without subsyndromal manic symptoms (Figure 5). However, the doses appear to differ for the different mood states across the spectrum, with 1.5 mg/day being perhaps the most consistently effective in bipolar depression, especially in those without subsyndromal manic symptoms, and with 1.5 mg/day or 3.0 mg/day both effective in bipolar depression with subsyndromal manic symptoms, and with 3.0 mg/day–6.0 mg/day effective in mania with or without concomitant depressive symptoms. In addition, cariprazine has one positive trial and others ongoing as an augmenting agent in patients with unipolar depression, and could potentially become the first D3-preferring dopamine serotonin partial agonist and the fifth agent overall, along with two other dopamine-serotonin partial agonists aripiprazole and brexpiprazole and the serotonin-dopamine antagonists quetiapine and olanzapine/fluoxetine combination, to be approved for augmenting or treating unipolar major depressive disorder.

Bipolar 1 spectrum.
The data for cariprazine thus inform not only the evolving notion that mood disorders are expressed across a spectrum (Figure 5), but also that the classical terms ‘antidepressant’ and ‘antipsychotic’ are confusing and possibly obsolete. That is, real patients may express mania and depression with varying degrees of each, and DSM-5 attempts to capture this, although ICD-11 does not. 2 During the DSM IV era (when many studies of mood disorders were completed, including those reviewed here for cariprazine), mood disorders were separate categories, namely, mania, depression, or full criterion depression combined with full criterion mania, called mixed mania (Figure 5). DSM-IV mixed mania was largely considered to be a form of mania and treated the same. With the introduction of DSM-5, mood disorders are now seen along a spectrum from pure depression on one end to pure mania on the other, with mixed features in between (i.e., depression with subsyndromal mania and mania with subsyndromal depression) (Figure 5). These changes have made it difficult to know how exactly to apply the data from trials of agents studied under earlier diagnostic organization, including cariprazine, to bipolar disorder diagnosed by DSM-5 or indeed by ICD-11 where the term ‘mixed’ is used differently (namely, for depression mixed with anxiety). 2 Fortunately, it does not seem to matter since cariprazine, and perhaps some other agents, appear to be effective across much of the entire spectrum from pure depression to pure mania. The next important question may be whether these same agents proven effective across the bipolar I spectrum, can be proven effective across the bipolar II spectrum as well as in unipolar depression, especially unipolar MDEs with mixed features of mania. Recent guidelines recommend use of a few of the serotonin-dopamine antagonists and none of the classical so-called antidepressant monoamine reuptake blockers for first line monotherapy treatment of unipolar MDEs with mixed features, since reuptake inhibitors are not proven to be effective and can also activate side effects, mania, and possibly suicidality, although not all guidelines agree completely on the place in treatment of antidepressants for bipolar spectrum disorders.3,34,35 No agent is yet approved for MDEs with mixed features, and studies to gain this approval are sorely needed. Since unipolar MDEs with mixed features are at high risk of converting to bipolar disorder with manic/hypomanic episodes, 3 it would be useful to see if agents such as cariprazine could not only treat unipolar MDEs with mixed features, but also prevent their conversion to bipolar disorder. The same could be said for agents such as lithium and lamotrigine, which have not been well studied in MDEs with mixed features.
Cariprazine’s actions across the mood disorder spectrum are a good example of why our nomenclature calling it an ‘antipsychotic’ because it was first approved for schizophrenia and has properties similar to other agents for schizophrenia, is a confusing if not erroneous practice since cariprazine also has robust antidepressant actions and anti-manic actions in bipolar disorder. The solution is not to call it an ‘antidepressant’ any more than an ‘antipsychotic’ but to name it for its pharmacologic properties, namely a D3-preferring dopamine serotonin partial agonist.4,9 The question remains whether the unique actions of cariprazine especially at D3 receptors, provide unique efficacy within the mood disorder spectrum, or whether its actions are a ‘class effect’ of all agents with serotonin dopamine antagonism or dopamine serotonin partial agonism. No head-to-head trials exist to address this point, but anecdotal observations that cariprazine has ‘brightening’ or ‘motivating’ actions in depressed patients and anti-anhedonia, anti-negative symptom actions in schizophrenia, 19 suggest that subpopulations of patients with these symptoms may be especially helped. Future investigations will need to sort this out.
In summary, cariprazine is now approved across the bipolar I mood spectrum, from mania with or without depressive symptoms to depression with or without manic symptoms. The entry of this new agent into the therapeutic armamentarium for treating bipolar disorder validates the clinical utility of the newer concept of bipolar disorder as a spectrum of disorders rather than discrete disorders at each end of the spectrum, and also demonstrates the wisdom of naming psychotropic drugs such as cariprazine for their pharmacologic actions, and not for one of their clinical indications.