
Abstract
Quetiapine fumarate, a first-line treatment for schizophrenia, exists in two formulations: extended release (XR) and immediate release (IR). This naturalistic, noninterventional study evaluated use of quetiapine XR/IR among in-patients with schizophrenia [ClinicalTrials.gov identifier: NCT01214135]. Data were collected from medical records. Categorical and numerical outcomes were compared using χ2 and t tests. Of 178 enrolled patients, 66% and 34% used quetiapine XR and IR respectively. Based on mean daily dose, XR was used as antipsychotic medication in 64% of patients compared with 40% of patients on IR (dose ≥ 400 mg/day; p = 0.002) and in higher doses than IR (494 versus 345 mg/day; p = 0.001; calculated averages). Schizophrenia was more commonly reported as reason for use of XR than IR (20% versus 0%; p = 0.0003). Patients with comorbid substance abuse or somatic disease were more likely to receive XR (p = 0.003; p = 0.03). Treatment cessation due to nonadherence was less common in patients on XR (3.4% versus 12%; p = 0.03). Polypharmacy was seen in 98% of patients. Quetiapine XR/IR usage varies in hospitalized patients with schizophrenia. XR is more often used in antipsychotic dosage; IR is more commonly used at lower doses as add-on therapy. Both quetiapine XR and IR have their place in clinical practice and provide treatment choice in schizophrenia.
Introduction
Schizophrenia is a debilitating mental disorder. It is associated with significant morbidity and mortality, and negatively impacts the quality of life of patients and healthcare budgets [Thieda et al. 2003; Hardeman et al. 2010]. Despite pharmacological advances, the treatment of schizophrenia remains a challenge, and suboptimal outcomes are still all too frequent [Kane and Correll, 2010] with comorbidities such as depression and anxiety being major determinants of the subjective quality of life [Hansson, 2006]. Depression, for example, occurs in up to 60% of patients with nonaffective psychosis, often precipitates hospital readmission and is predictive of relapse and suicide [Mulholland and Cooper, 2000; Carlborg et al. 2010].
Medication nonadherence is common [Goff et al. 2011] and poor adherence leads to poor outcomes, including patient relapse, rehospitalization, delayed time to remission, increased risk of attempted suicide and higher healthcare costs [Thieda et al. 2003; Leucht and Heres, 2006; Hardeman et al. 2010]. In contrast, improved adherence leads to better outcomes [Laan et al. 2010].
Atypical antipsychotics (AAPs) are recommended as first-line treatment for schizophrenia [NICE, 2002; Buchanan et al. 2010] yet their different binding properties [Gardner et al. 2005] result in different efficacy on the positive, negative and comorbid symptoms of schizophrenia and the type and extent of side effects (e.g. somnolence, extrapyramidal symptoms and weight gain) [Geddes et al. 2000; Naber and Lambert, 2009]. The different efficacy and tolerability profiles of AAPs add to the complexity of treating schizophrenia in real life and physicians do not always adhere to treatment guidelines [Kroken et al. 2009; Parks et al. 2009], but often augment first-line treatment with other drugs [Wolff-Menzler et al. 2010], combine antipsychotics [Tapp et al. 2003; Broekema et al. 2007; Barnes and Paton, 2011] or switch to other AAPs to optimize symptomatic control [Nyhius et al. 2010].
This prescribing behaviour suggests that randomized controlled trials (RCTs) upon which guidelines are based, although needed, provide limited information on how drugs are actually used and their effectiveness in clinical practice [Andrews, 1999; Wolff-Menzler et al. 2010; Barnes and Paton, 2011]. For example, select patient populations are enrolled in RCTs, which do not reflect the disease severity or comorbidities of the wider population [Simes, 2002; Gorwood, 2006]. They are also strictly monitored, which may encourage patient adherence, and often focus on monotherapy as opposed to combination therapy. Despite some recent studies [Altamura et al. 2008; Kroken et al. 2009; Barnes and Paton, 2011], real world evidence on the proven efficacy and clinical use of AAPs is clearly lacking [Gorwood, 2006; Altamura and Glick, 2010], as is the case for quetiapine fumarate, an established first-line oral AAP for schizophrenia [Riedel et al. 2007; Baldwin and Scott, 2009].
Quetiapine has two formulations with different pharmacokinetic properties: immediate release (IR) and extended release (XR). Quetiapine XR is characterized by sustained drug exposure with once-daily dosing, a faster dose titration and different pharmacological and tolerability profiles than quetiapine IR [Peuskens et al. 2007; Baldwin and Scott, 2009; Figueroa et al. 2009; Meulien et al. 2010], which is taken twice daily and over a longer dose titration period [Riedel et al. 2007]. Quetiapine XR is also associated with a lower intensity of sedation than quetiapine IR [Datto et al. 2009].
In a retrospective, noninterventional setting, we examined the real-life use of quetiapine XR/IR for treatment of hospitalized patients with schizophrenia in Sweden. The study included assessment of dose levels, add-on therapy and simultaneous use, as well as concomitant medication, disease severity and comorbidity in these patients.
Patients and methods
Study design
This noninterventional, retrospective, multicenter study was conducted at 14 sites of in-patient care in Sweden. Data were collected retrospectively by reviewing medical records during the study period (1 July 2009–30 September 2010). Sites with any kind of prescription restrictions regarding quetiapine XR or IR were not eligible for the study.
Each study site performed a manual search in the medical record system for all patients with schizophrenia who were admitted to hospital due to psychotic symptoms and had received at least one dose of quetiapine XR or quetiapine IR during hospitalization. All patients who fulfilled the eligibility criteria (specified below) were enrolled into either the quetiapine XR group or the quetiapine IR group. If a subject had received both quetiapine XR and quetiapine IR simultaneously the highest dose determined which group the patient was enrolled in.
All data were entered into a web-based data capture system according to study protocol, and were kept anonymous and identified only by an enrolment code.
The study protocol was reviewed and approved by the Regional Ethics Committee in Gothenburg, Sweden. The study [ClinicalTrials.gov identifier: NCT01214135] was performed in accordance with ethical principles consistent with the Declaration of Helsinki, International Conference on Harmonisation of Good Clinical Practice (ICH GCPs) and the applicable legislation on noninterventional studies.
Patient population
Patients of both sexes aged 18–65 years and diagnosed with schizophrenia (International Classification of Diseases 10th revision diagnosis codes F20, F23.1, F23.2, and F25) could be enrolled. They had to have been hospitalized for psychotic symptoms (admission and discharge dates available) and received at least one dose of quetiapine XR or quetiapine IR at any time during hospitalization (regardless of dose). Patients who were participating in a clinical trial during the study period or who were being treated in forensic care were excluded.
Study outcomes
The primary outcome was to evaluate the antipsychotic use of quetiapine XR and IR in patients with schizophrenia. Patients who received a total daily dose of at least 400 mg were regarded as being treated with quetiapine mainly for antipsychotic reasons, whilst those on a total daily dose of less than 400 mg were regarded as having been treated with quetiapine as an add-on to other antipsychotics. The cutoff dose of 400 mg quetiapine was chosen as quetiapine shows sufficient D2-receptor occupancy and thus antipsychotic properties throughout the dose range of 400–800 mg/day [Kapur et al. 2000].
The following secondary outcomes were also investigated: the use of quetiapine XR/IR treatment in high doses and in lower doses as add-on therapy; simultaneous treatment with quetiapine XR/IR; concomitant medication; patient demographics and comorbidities (ICD10 diagnosis); disease severity at hospital admission and discharge by the Global Assessment of Functioning (GAF) score; information about previous and current hospitalizations; and electroconvulsive therapy (ECT).
Statistical analyses
All analyses were prespecified in a statistical analysis plan and performed using the SAS software, version 9.2. Means were compared by a t test, except for GAF values when an analysis of variance was used with least squared means (LSM) and baseline GAF as covariate. Proportions were compared using a χ2 test. The percentage of patients treated with concomitant drugs was calculated using a Poison regression with length of hospital stay as offset variable.
The statistical null hypothesis was that the groups had the same average value or proportion and p values for rejecting this hypothesis were calculated. A p value below 0.05 was considered as significant.
Results
Patient demographics
A total of 178 patients were included in the study; 118 (66%) received quetiapine XR and 60 (34%) received quetiapine IR. Demographic data were equal for the two treatment groups (Table 1).
Patient demographics.
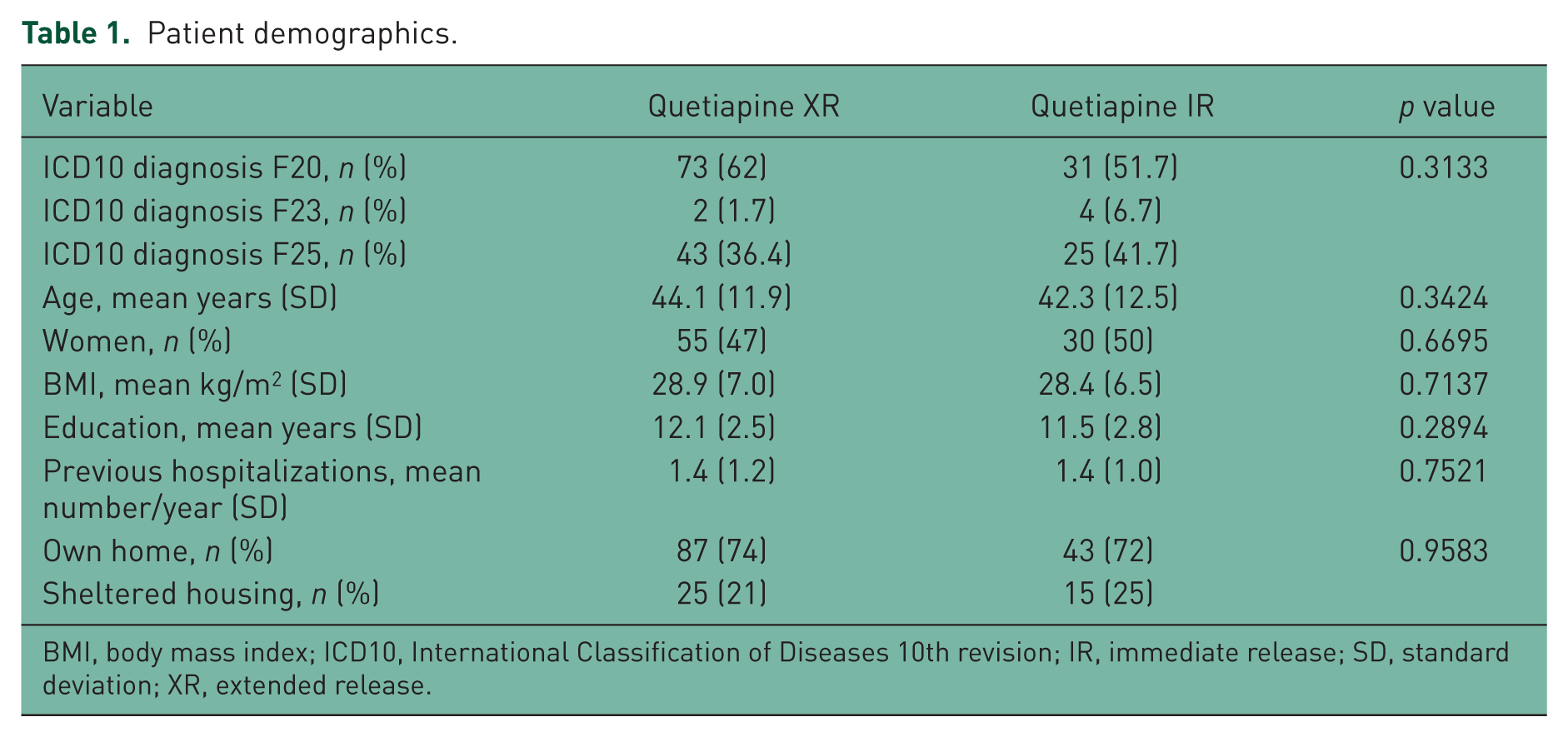
BMI, body mass index; ICD10, International Classification of Diseases 10th revision; IR, immediate release; SD, standard deviation; XR, extended release.
Differential dosing in patients on quetiapine XR versus quetiapine IR
Significantly more patients in the quetiapine XR group (64%) compared with the quetiapine IR group (40%) were treated with quetiapine in doses of at least 400 mg/day (p = 0.002) (Table 2). Significantly more patients receiving quetiapine XR than IR were also treated with doses of at least 600 mg/day (52% versus 23%, p = 0.0003). Moreover, 27% of the patients in the IR group had a mean quetiapine dose below 200 mg/day during the inpatient stay, while the same was seen in only 13% of the patients in the XR group.
High-dose quetiapine XR and quetiapine IR usage.

IR, immediate release; XR, extended release.
The mean daily dose of quetiapine XR received during hospitalization was significantly higher than that of quetiapine IR (494 mg/day versus 345 mg/day respectively; p = 0.001) (Figure 1). Furthermore, the mean dose of quetiapine XR used in patients as ongoing treatment at discharge was significantly higher than that of quetiapine IR (494 and 335 mg/day respectively; p = 0.002).
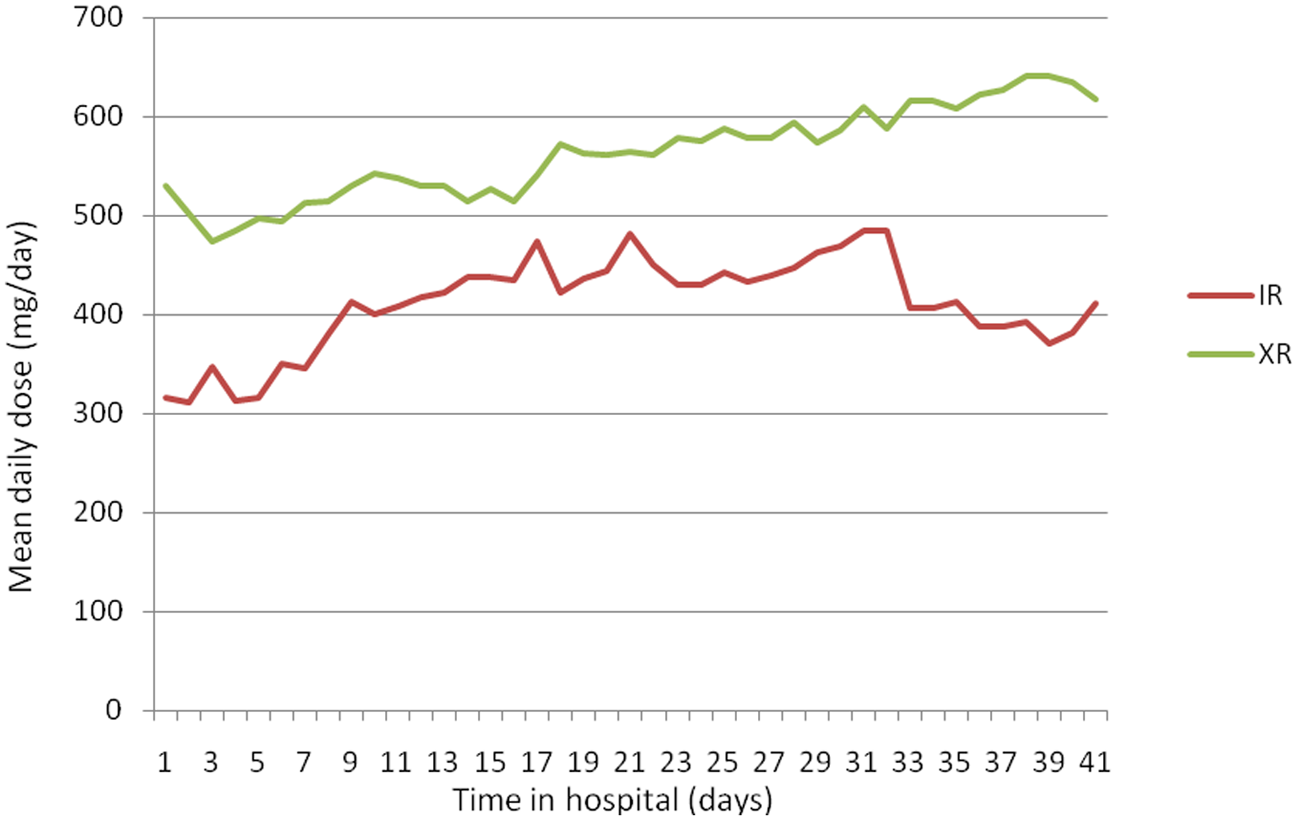
The mean daily dose (mg/days) of quetiapine extended release (XR) and quetiapine immediate release (IR) versus time in hospital (days).
Concomitant medication
The mean number of concomitant medications was 3.11 in the quetiapine XR group and 4.24 in the quetiapine IR group (27% difference, p = 0.04). Almost all patients (98%) were treated with one or more concomitant psychiatric medications during hospitalization. Of these patients, 85% in the IR group and 81% in the XR group were treated with other antipsychotics (nonsignificant).
Patients receiving quetiapine IR were to a higher degree treated with other antipsychotics both short and long term than those on quetiapine XR (Table 3). Most concomitant antipsychotic and antidepressant medications were long term, while drugs for mood stabilization, anxiety or sleep disorders were short term. There was no significant difference in the number of concomitant medications at discharge (2.28 versus 2.53 for the quetiapine XR and IR groups respectively).
Percentage of patients with other treatments per month of hospital stay, short term (≤ 7 days) and long term (> 7 days) term.
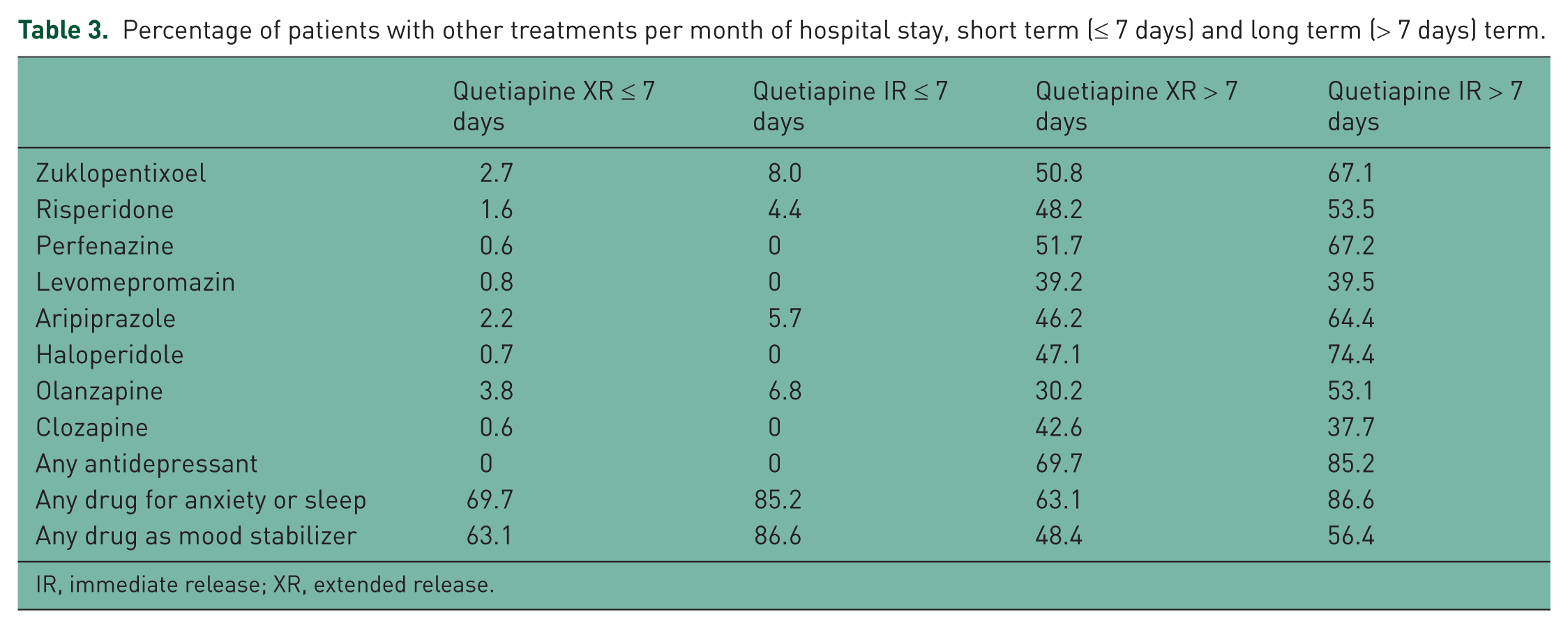
IR, immediate release; XR, extended release.
Patient assessment
No significant differences were seen with regard to GAF total score, hospitalisations, or ECT treatments. The mean GAF total score at admission for patients receiving quetiapine XR was 30.6 compared with 32.8 for those on quetiapine IR (p = 0.22); the mean GAF total score at discharge was LSM 44.8 versus 46.3 (p = 0.44); and changes in GAF total score during hospitalization were LSM 14.9 versus 15.7; p = 0.70 between the quetiapine XR and IR groups. Patients on quetiapine XR had a numerically longer duration of hospitalization than those in the quetiapine IR group (45.8 versus 33.2 days respectively; p = 0.08). ECT treatment was seen in eight patients in the quetiapine XR group versus one patient in the IR group (p = 0.11).
Patient comorbidities and reasons for treatment
Patient comorbidities and reasons for treatment were recorded for psychiatric conditions other than schizophrenia, as well as for somatic reasons. There were a number of reasons for treating other disorders, including insomnia, psychosis, anxiety, and schizophrenia per se. A total of 38% of patients on quetiapine IR and 36% of those treated with quetiapine XR had comorbidities (nonsignificant, p = 0.84).
Schizophrenia was significantly more commonly reported as a reason for treatment in patients on quetiapine XR than in those on quetiapine IR (20% versus 0% respectively; p = 0.0003). In this study quetiapine IR was more commonly used for treatment of psychosis (75% versus 52% respectively; p = 0.0019); while only numerical differences were noted for anxiety (57% versus 42% respectively; p = 0.06). There was no significant difference between the groups with respect to insomnia or sedation as reasons for treatment.
Significantly more patients had somatic disease in the quetiapine XR group than in the quetiapine IR group (31% versus 18%, p = 0.03). Patients with comorbid substance abuse were more likely to receive treatment with quetiapine XR than quetiapine IR (p = 0.003) (Table 4). Also, significantly more patients (12%) in the quetiapine IR group reported nonadherence as a reason for ceasing treatment compared with those in the quetiapine XR group (3.4%) (p = 0.03).
Comorbid substance abuse.

ICD10, International Classification of Diseases 10th revision; IR, immediate release; XR, extended release.
Sequential and simultaneous treatment with quetiapine XR and IR
A total of 33 patients used both quetiapine XR and quetiapine IR during hospitalization. Four were taking both quetiapine XR and IR when admitted to the hospital, 18 (10.2% of total study population) received quetiapine XR and IR therapy at the same time during hospitalization, and 15 (8.4% of total population) used quetiapine XR and IR sequentially. Among the 18 patients who used both quetiapine formulations in combination, 14 patients used a higher mean dose of quetiapine XR (Table 5).
Quetiapine XR and quetiapine IR usage pattern during hospitalization.

IR, immediate release; SD, standard deviation; XR, extended release.
When each treatment shift was evaluated, we found 22 shifts from quetiapine IR to XR, 9 shifts from quetiapine XR to IR, 3 shifts from quetiapine IR to a quetiapine XR/IR combination, 4 shifts from quetiapine XR to a quetiapine XR/IR combination, and 3 shifts from a quetiapine XR/IR combination to quetiapine XR monotherapy.
Discussion
This naturalistic study investigated the clinical use of quetiapine XR and quetiapine IR in 178 hospitalized patients with schizophrenia in 14 psychiatric clinics in Sweden., The present study documents a differential use of quetiapine XR compared with quetiapine IR with respect to factors such as dosing, add-on medications, comorbidity, reason for treatment, and severity of disease in patients with similar baseline characteristics who are severely ill and with a high use of concomitant medication.
The primary finding was that quetiapine XR was used in considerably higher doses than quetiapine IR. Significantly more patients received quetiapine XR at a dose of at least 400 mg/day than quetiapine IR during their hospital stay. That also held true for the number of patients receiving doses of at least 600 mg/day and less than 200 mg/day. This clear difference in dosing between the two formulations of quetiapine suggests that quetiapine XR was used more commonly for antipsychotic use, while quetiapine IR may have been used for anxiety/sedation purposes and that these patients required additional antipsychotic medication to treat schizophrenia per se.
Another important finding was the extensive use of concomitant medication in this patient population (98% of patients). Concomitant medication was significantly higher in patients on quetiapine IR during hospitalization, with 27% more concomitant medications seen than for patients on quetiapine XR. This finding supports the interpretation that quetiapine XR more often is used as the main antipsychotic drug, whereas quetiapine IR is more often used as an add-on medication in schizophrenia. Overall, patients had two or more – and in some cases up to seven or eight – antipsychotic medications during hospitalization, reflecting the typical situation faced by physicians of severely ill patients. The most common historical combination of medications in this setting is that of a typical plus an atypical antipsychotic [Bingefors et al. 2003; McCue et al. 2006]. This was also the case here, the most common typical antipsychotics being zuclopenthixol and haloperidol when used for at least 7 days.
Patients with comorbid substance abuse were significantly more likely to receive treatment with quetiapine XR than IR. Also, patients treated with quetiapine XR were reported to have more somatic disease than those on quetiapine IR.
Further, significant differences in the reported reasons for treatment between quetiapine XR and IR were seen. Patients on quetiapine XR were more often treated for schizophrenia per se and those on quetiapine IR more often for psychosis, although this result should be interpreted with caution as reported reasons for treatment may not be consistent across prescribers and patients. Further, although statistically not significant, lower GAF scores at hospital admission, longer duration of hospitalization, and higher use of ECT was reported for patients receiving quetiapine XR compared with IR.
Taken together, the present study points to a different use of quetiapine XR compared with quetiapine IR in this setting.
Medication adherence should arguably increase in importance with disease severity. In fact, adherence is a considerable challenge in schizophrenia [Goff et al. 2011]. Llorca (2008) estimates that at least 50% of patients are partially compliant or noncompliant within 1 year and 75% within 2 years of hospital discharge. However, any improvement in adherence will improve patient outcomes [Ascher-Svanum et al. 2010; Laan et al. 2010]. A complex dosing regimen is one factor that may have a considerable negative impact on drug adherence. Once daily dosing has been shown to be significantly associated with improved adherence in patients with schizophrenia, also when controlling for various covariates [Remington et al. 2007; Diaz et al. 2004]. In this study, patients receiving quetiapine IR (twice daily dosing) reported nonadherence as a reason for discontinuation of treatment significantly more often than those on quetiapine XR (once daily dosing).
Thirty-three patients (19% of total study population) used both formulations of quetiapine during their hospital stay. Of these patients, 18 used both formulations concomitantly. Although polypharmacy is common among these patients, it does not in itself explain why quetiapine XR and IR are used simultaneously, but may indicate that quetiapine XR and IR are sometimes used in a complementary as opposed to a substitutional fashion. That interpretation is further supported by the fact that 14 out of these 18 patients used quetiapine XR in considerably higher doses than IR. Clearly, quetiapine IR is more often used as an add-on medication in these patients, potentially for its sedative effect. One may also notice that, in the patients who used quetiapine XR and IR sequentially, switches from quetiapine IR to XR were far more common than switches in the other direction.
A differential use of the two formulations of quetiapine in clinical practice of schizophrenia may be explained by their different pharmacological properties. Quetiapine XR, with its smoother plasma concentration profile than quetiapine IR allowing for faster titration [Figueroa et al. 2009], reduces the time required to reach optimal dose [Peuskens et al. 2007]. A recent study investigated if the pharmacokinetic differences translate into different time curves for central D2 dopamine receptor occupancy. Peak D2 receptor occupancy was significantly higher with the IR formulation than quetiapine XR and may explain pharmacodynamic differences [Nord et al. 2011]. A divergence in receptor occupancy between the quetiapine formulations may be expected to translate to some differences in clinical effects. In fact, quetiapine XR has been associated with a lower intensity of self-reported sedation than quetiapine IR [Datto et al. 2009] as well as less orthostatic dizziness [Mamo et al. 2008].
This study has important strengths. First, our naturalistic study avoided the highly selected patient populations and arguably unrealistic setting of RCTs by enrolling schizophrenia inpatients faced by psychiatrists in their everyday clinical practice. Clinical practice differs substantially from the context of RCTs in terms of characteristics of patients (e.g. comorbidities), drug exposure (e.g. monotherapy versus polypharmacy), dosage and compliance. In addition, 50% of patients were women, which is not common in RCTs [Philip et al. 2008; Johnsen et al. 2010]. Second, there was no bias in patient selection also due to the fact that informed consent was not required. Third, a retrospective data analysis of medical records ensured that treatment choice for patients was not influenced and thus real-life clinical data were collected. Fourth, patients from 14 geographically spread out psychiatric clinics participated in the study and therefore the results should be representative for Sweden.
There are also some limitations. First, the results build on reports by the healthcare professionals and may not be fully accurate. Second, this study enrolled severely ill, hospitalized patients with schizophrenia and so the results may not be applicable to the outpatient clinical setting. Further, this study is limited to Swedish psychiatric inpatient care. It could therefore be interesting to study the clinical practice use of the quetiapine formulations in the outpatient setting as well as in other countries.
This retrospective, observational study has provided new insight into the differential use of quetiapine XR versus quetiapine IR in the clinical treatment of patients with schizophrenia in the acute, inpatient setting. Whereas quetiapine XR is used in significantly higher doses, and as a primary antipsychotic medication, quetiapine IR is used in lower doses, more often as an add-on medication, possibly for its anxiolytic or sedative effects. Polypharmacy was very common in this patient population and reflects the reality for psychiatrists who treat severe mental illness. This is an important finding because these severely ill patients are often excluded from traditional RCTs. Our study thus suggests that more knowledge is needed about treatment patterns and patient outcomes in clinical practice, to complement the picture provided by RCTs with their often highly selected patient populations.
The differential quetiapine XR/IR usage is most likely due to differences in titration, dosing, and pharmacological and tolerability profiles. Most likely it also reflects the psychiatrist’s need for treatment choice. An individualized treatment is essential for treatment success in schizophrenia. Restricting the range of drugs to which psychiatrists have access risks worsening treatment outcomes, according to European psychiatrists [Altamura et al. 2008]. Our study shows that quetiapine XR and quetiapine IR are not substitutes, but complement each other when treating schizophrenia inpatients. Both quetiapine XR and quetiapine IR are needed in clinical practice for the treatment of schizophrenia.
Footnotes
Funding
Dr Graz.yna Söderbom, Klipspringer AB, rovided medical writing support funded by AstraZeneca. This study was sponsored by AstraZeneca.
Conflict of interest statement
Lars Eriksson (Principal Investigator) has participated in clinical trials by Janssen, EliLilly, and AstraZeneca; and given lectures and participated in advisory boards for Janssen, BMS, EliLilly, and AstraZeneca. Andreas Carlborg is a consultant to and has participated in clinical trials by AstraZeneca; and given lectures for Wyeth. Teresa Hallerbäck and Leif Jørgensen are employees of AstraZeneca.
This manuscript was prepared in line with guidelines established by the International Committee of Medical Journal Editors (ICMJE) and published in its Uniform Requirements of Manuscripts Submitted to Biomedical Journals.